ORIGINAL REPORT
Identification of Stigmatization and Relevant Predictors in People with Alopecia Areata and Androgenetic Alopecia: A Comparative Cross-sectional Study in German-speaking Countries and the USA
Johaina KULLAB1, Caroline F. Z. STUHLMANN2,3, Stefanie ZIEHFREUND1, Hannah WECKER1, Tilo BIEDERMANN1 and Alexander ZINK1,4
1Technical University of Munich, TUM School of Medicine and Health, Department of Dermatology and Allergy, Munich, Germany, 2The Graduate Center & Hunter College, City University of New York, Department of Psychology, New York, NY, USA, 3University Medical Center Hamburg-Eppendorf, German Center for Health Services Research in Dermatology, Institute for Health Services Research in Dermatology and Nursing (IVDP), Hamburg, Germany, and 4Division of Dermatology and Venereology, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden
Stigmatization of skin conditions like alopecia areata (AA) and androgenetic alopecia (AGA) impairs quality of life (QoL), but research is limited. The aim of this study was to compare stigmatization and QoL in individuals with AA and AGA in German-speaking (GS) and US samples and identify stigmatization predictors. This cross-sectional online survey included AA and AGA participants from GS countries (April–August 2020) and the USA (May–August 2021). Stigmatization and QoL were assessed using the Perceived Stigmatization Questionnaire (PSQ) and Hairdex, along resilience, happiness, and social support assessment tools. Regression analyses evaluated disease severity, duration, age, gender, marital status, and social support as stigmatization predictors. All subgroups perceived stigmatization and impaired QoL. GS-AA (n = 423, 93.6% women) participants perceived more stigma but better QoL than GS-AGA (n = 102, 79.4% women). The US sample (AA: n = 199, 84.4% women; AGA: n = 47, 93.6% women) showed similar trends, though insignificant. GS participants reported higher stigma and US participants lower QoL. Stigmatization was associated with being male, younger, employed, severe disease, daily-life restrictions, and anxiety. Both samples were predominantly female, with the US sample being older and smaller, potentially reducing significance. In conclusion, sociodemographics and gender influence stigmatization and QoL. Interventions should enhance resilience and social support.
SIGNIFICANCE
This study explores the impact of stigmatization in 2 common types of hair loss – androgenetic alopecia and alopecia areata – in Germany and the USA. It highlights that hair loss can lead to significant stigmatization, especially in younger individuals and those with severe symptoms. While alopecia areata patients generally feel more stigmatized than those with androgenetic alopecia, they also report better quality of life. Factors like age, gender, employment, and social support influence the experience of stigma. The present findings stress the need for targeted interventions to reduce stigma of individuals affected by hair loss with regard to their sociocultural background.
Key words: alopecia areata; androgenetic alopecia; burden of disease; hair loss; quality of life; stigmatization.
Citation: Acta Derm Venereol 2025; 105: adv42278. DOI: https://doi.org/10.2340/actadv.v105.42278.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 16, 2024. Accepted after revision: Dec 17, 2024. Published: Mar 3, 2025.
Corr: Alexander Zink, MD, MPH, PhD, Technical University of Munich, TUM School of Medicine and Health, Department of Dermatology and Allergy, Biedersteiner Strasse 29, DE-80802 Munich, Germany. E-mail: alexander.zink@tum.de
Competing interests and funding: TB has received grants from Celgene-BMS, Lilly, Mylan, Novartis, Sanofi, and Regeneron, has served on an advisory board for LEO Pharma, Lilly, Mylan, and Sanofi, received consultancy or speaker’s honoraria from Lilly, Mylan, Novartis, Regeneron, and Sanofi, and is past-president of the German Society of Dermatology (unpaid). AZ has received unrestricted research grants from Novartis Pharma and Leo Pharma, has received consultancy and speaker’s honoraria from AbbVie, Almirall, Amgen, Beiersdorf Dermo Medical, Bencard Allergie, BMS, Celgene, Eli Lilly, GSK, Janssen Cilag, Leo Pharma, Miltenyi Biotec, Novartis, Pfizer, Sanofi-Aventis, Takeda Pharma, and UCB Pharma, and has held a fiduciary role for the German Society of Dermatology (unpaid). JK, CFZS, SZ, HW have no conflicts of interest to declare.
INTRODUCTION
The most common form of hair loss is androgenetic alopecia (AGA), impacting roughly 50% of Caucasian men post-puberty and 40% of Caucasian women over 40 years of age. Its multifaceted aetiology involves genetic and endocrine factors leading to irreversible hair loss (1). Racial and ethnic differences exist: Asians show a lower incidence in each decade and AGA is 4 times less frequent among Black individuals than in Caucasians (2). The second most common non-scarring alopecia is alopecia areata (AA), an autoimmune disease with an estimated worldwide lifetime incidence of 2% (3). It affects both sexes equally, and peaks in young adulthood (4). It manifests as round patches of hair loss on the scalp or body, potentially progressing to total hair loss, including facial hair (alopecia universalis) (3). A US study suggests a higher likelihood of AA in Black Americans compared with White individuals, whereas Asians had a reduced likelihood of AA.
Hair plays a significant role in identity, self-image, and self-expression; thus, hair loss can lead to psychological distress, compromising quality of life (QoL) (5). Global studies indicate a higher burden of disease for AA in young adults, females, and high socioeconomic countries (6). Recent data shows a higher AA incidence in the USA compared with Germany (92 vs 72 per 100,000 patient-years) (7), influenced by regional sociodemographic factors, healthcare resources, and awareness (8).
Hair loss is more socially accepted in men, leading to a greater impact of alopecia-associated burden in women (9, 10). Both AA and AGA have unpredictable disease trajectories and medical treatments seldom reverse them (1, 11). Individuals with AA, compared with AGA, are more prone to depression and anxiety (5, 12, 13). Research suggests that individuals with hair loss commonly experience stigma, irrespective of its pathogenesis (14).
Stigmatization is the discriminating process of ascribing disapproval and humiliation to individuals based on their characteristics (external or social stigma) (12, 15). Stigmatized individuals may gradually internalize this negative evaluation and feel deficient. Behaviourally, individuals try to conceal their negatively evaluated characteristics or become socially isolated, increasing their burden (15). Stigma also hinders optimal healthcare by reducing the willingness to seek medical help and adhere to treatment (16). The German Federal Ministry of Health launched projects to destigmatize people with visible skin changes (17). Besides surveys on psoriasis, understanding of perceived stigmatization in other skin diseases (i.e., alopecia) is scarce (18). A systematic review on stigmatization shows only 4 studies using the Hairdex, and stigma subscale values varied widely (14). Opposing viewpoints (16, 18) contradict the claim that stigma and sociodemographic factors were uncorrelated. Conceptual models of stigma in visible skin diseases were derived considering sociodemographics, social interactions, disease characteristics, QoL, and coping strategies (18, 19). Younger age and being single were associated with higher stigma, while resilience and social support were considered protective factors (19). The lack of high-quality research on effective alopecia stigma-reducing approaches highlights the need for further research to develop interventions (17, 20). This study aimed to compare the stigma and disease-related QoL of individuals with AA and AGA in the context of 2 highly developed regions, i.e., a US and German-speaking (GS) sample, and to identify influencing factors on stigmatization.
MATERIALS AND METHODS
Study design, setting, and participants
This cross-sectional online study was conducted in Germany, Austria, Switzerland (GS), and the USA. Four German, 1 Austrian, and 1 Swiss alopecia patient support organizations promoted the study in their online newsletters from April to August 2020. The largest was “Alopecia Areata Deutschland e.V.” with 1,200 members. From May to August 2021, National Alopecia Areata Foundation email listservs recruited US participants. Eligible participants were 18 or older, living in the USA or a GS country, and self-reported an AA or AGA diagnosis from a doctor. Iatrogenic and scarring alopecia were excluded. Electronic informed consent was obtained from all participants via SoSci survey. The Technical University of Munich Medical Faculty’s and City University of New York’s ethics commissions approved the project.
Questionnaires
The English and German anonymous questionnaires were created consensus-based by 2 physicians, 2 epidemiologists, a psychologist, and a patient representative. Data collected included demographics, and the diagnosis (AA, AGA) using clinical cartoons to self-assess severity across 4 stages: disease duration, family history, and disease’s impact on mood.
Hairdex evaluated disease-related QoL in functioning, emotions, symptoms, self-confidence, and stigmatization (21). Stigmatization was tested using the Perceived Stigmatization Questionnaire (PSQ) (22, 23). Moreover, the Contextual Illness Support Scale (CISS) for the USA and the revised Illness-specific Social Support Scale (ISSS) for the GS sample (24, 25), the Brief Resilience Scale (BRS) (26), Ed Diener’s Satisfaction With Life (SWL) and Scale of Positive And Negative Experience (SPANE) (27, 28), the WHO-5 (29), and Generalized Anxiety Disorder 7 (GAD-7) were used (30) (Appendix S1).
Statistical analysis
Participants’ characteristics were described using mean (standard deviations [SD]) or median (interquartile ranges [IQR]), based on normality tested via Shapiro–Wilk test. Only complete cases were included (Appendix S2). Stigma and disease-related QoL were compared between groups (GS-AA vs GS-AGA; US-AA vs US-AGA, GS vs US) using the Kruskal–Wallis test. Subgroup analyses by severity, gender, and racial identity used the Mann–Whitney U test. Stigmatization scores were correlated using the Spearman coefficient. Additionally, a multiple linear regression model including all samples assessed predictors of perceived stigmatization (PSQ total) with the variables age, gender, marital status, education, employment, severity grade, disease duration, effect of alopecia on mood, emotions, self-confidence, symptoms, functioning, anxiety, positive and negative affect, describing categorized variables (see Appendix S3). Regression coefficients (β) were estimated with 95% confidence intervals (CI), and assumptions were tested (Appendix S4; Tables SI and SII). P-values < 0.005 were considered significant. Analysis was performed using R version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
A total of 525 GS participants (AA: 423, AGA: 102), mostly female, had a median age of 38 (29.0–48.0) years (Fig. 1). Table I contains all disease-specific demographics. AA severity was mostly grade IV (n = 269, 64%), while AGA severity equally ranged from grades I–III.
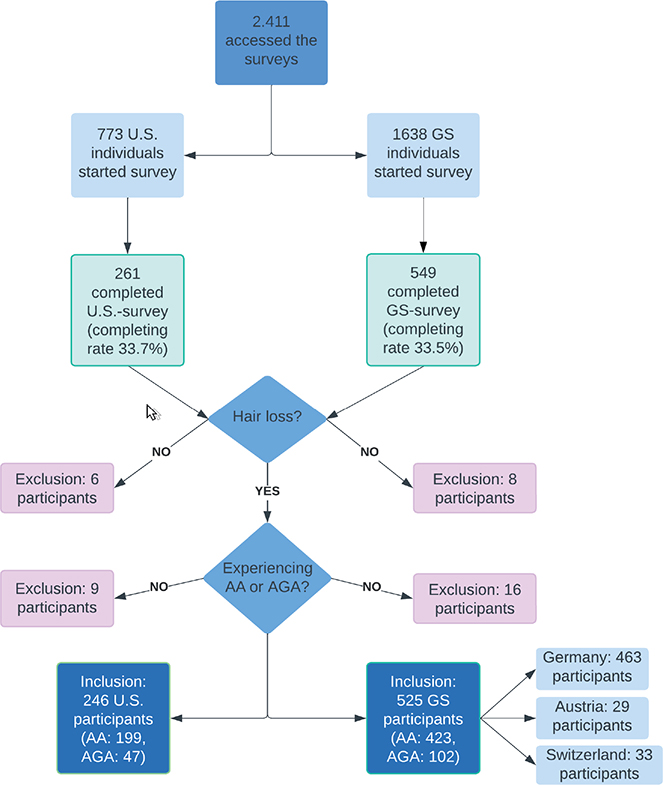
Fig. 1. Flowchart of participants. AA: alopecia areata. AGA: androgenetic alopecia. GS: German-speaking sample.
| Item | GS sample (n = 525) |
US sample (n = 246) |
| Sex, n (%) | ||
| Female | 477 (90.9) | 213 (86.6) |
| Male | 48 (9.1) | 33 (13.4) |
| Age in years, median [IQR] | 38.0 [29.0–48.0] | 52.0 [39.0–61.0] |
| Marital status, n (%)1 | ||
| In a partnership | 387 (73.7) | 151 (61.4) |
| Single | 138 (26.3) | 95 (38.6) |
| Education, n (%)2 | ||
| High | 242 (46.1) | 181 (73.5) |
| Moderate | 280 (53.4) | 59 (24.1) |
| Low | 3 (0.6) | 6 (2.4) |
| Employment, n (%) | ||
| Employed | 384 (73.1) | 138 (56.1) |
| Self-employed | 28 (5.3) | 23 (9.3) |
| Student | 61 (11.6) | 8 (3.3) |
| Unemployed | 52 (9.9) | 77 (31.3) |
| Diagnosis, n (%) | ||
| AA (alopecia areata) | 423 (80.6) | 199 (80.9) |
| AGA (androgenetic alopecia) | 102 (19.4) | 47 (19.1) |
| Effect of alopecia on mood, n (%) | ||
| High | 126 (28.3) | 104 (42.3) |
| Moderate | 112 (25.2) | 66 (26.8) |
| Low | 119 (26.7) | 56 (22.7) |
| None | 88 (19.8) | 20 (8.1) |
| Perceived extent of illness, n (%) | ||
| Low | 33 (6.3) | 11 (4.5) |
| Moderate | 175 (33.3) | 78 (31.7) |
| Severe | 317 (60.4) | 157 (63.8) |
| AA – Severity grade, n (%)3 | ||
| I | 53 (12.5) | 25 (12.6) |
| II | 54 (12.8) | 49 (24.6) |
| III | 47 (11.1) | 37 (18.6) |
| IV | 269 (63.6) | 88 (44.2) |
| AA – Duration of illness, years, median [IQR] | 11.0 [4.0–21.0] | 15.0 [6.0–30.0] |
| Relatives affected by AA, n (%) | ||
| None | 361 (85.3) | 143 (71.9) |
| Yes | 62 (14.7) | 56 (28.1) |
| AGA – Severity grade (female patients)4 | ||
| I | 31 (38.3) | 3 (6.8) |
| II | 26 (32.1) | 20 (45.5) |
| III | 24 (29.6) | 21 (47.7) |
| AGA – Severity of illness levels for male patients5 | ||
| I | 5 (23.8) | 0 |
| II | 10 (47.6) | 2 (66.7) |
| III | 6 (28.6) | 1 (33.3) |
| IV | 0 | 0 |
| AGA – Duration of illness, years, median [IQR] | 5.0 [3.0–16.0] | 15.0 [6.0–20.0] |
| Relatives affected by AGA, n (%) | ||
| None | 32 (31.4) | 24 (51.1) |
| Yes | 70 (68.6) | 23 (48.9) |
| Racial identity, n (%) | ||
| American Indian, Native American, Alaskan Native | 2 (0.8) | |
| Asian | 9 (3.7) | |
| Black or African American | 26 (10.6) | |
| White | 197 (80.1) | |
| Bi-racial or Multi-race | 5 (2.0) | |
| Other6 | 7 (2.8) | |
| Identification with Hispanic, Latino, or Spanish origin | ||
| None | 226 (91.9) | |
| Yes | 20 (8.1) | |
| 1Marital status: single (single, divorced, widowed), in a partnership (married, domestic partnership). 2High (Postgraduate [Doctorate], Master’s, Bachelor’s, Community college), Moderate (High school, Middle school, Associate’s degree, Professional degree), Low (No degree). 3Severity of illness levels: I – less than 30% of scalp affected; II – more than 30% affected; III – alopecia totalis; IV – alopecia universalis. 4Severity of illness for females affected by androgenetic alopecia after Ludwig. 5Severity of illness for males affected by androgenetic alopecia after simplified Hamilton–Norwood. 6Other racial identities: 1 East Indian, 5 Hispanic, 1 Middle Eastern. IQR: interquartile range. |
||
The median age of 246 US participants (AA: n = 199, AGA: n = 47) was 52 (39.0–61.0) years, with mostly AA severity grade IV (44%) and AGA focused on grades II and III (Fig. 1). The English Hairdex subscales correlated well with DLQI and SF-20 scores, maintaining validity (Table SIII).
German-speaking sample
Mean total PSQ score was 2.22 (0.56), while mean Hairdex subscale values ranged from 22.4 (18.5) for symptoms to 45.4 (25.7) for emotions (Table II). In both alopecia groups PSQ scores increased with disease severity (Fig. 2; Table SIV). Increased severity (AA: I vs IV) was linked to higher QoL impairment in symptoms (H(3) = 23.94, p = 0.006), emotions (H(3)=19.91, p = 0.010), self-confidence (H(3) = 45.42, p < 0.001), but lower in stigma (H(3) = 13.75, p = 0.003, Figs 1–2). For GS-AA, longer disease duration negatively correlated with QoL subscales (–0.18 ≤ r ≤ – 0.06, p < 0.001), except for subscale stigma. Similarly, the AGA sample showed a negative trend. Men had higher PSQ scores than women (AA: 2.27 (0.79) vs 2.22 (0.55), z = 0.18, p = 0.93; AGA: 2.09 (0.46) vs 1.95 (0.46) z = 0,20, p = 0.18), though not significantly.
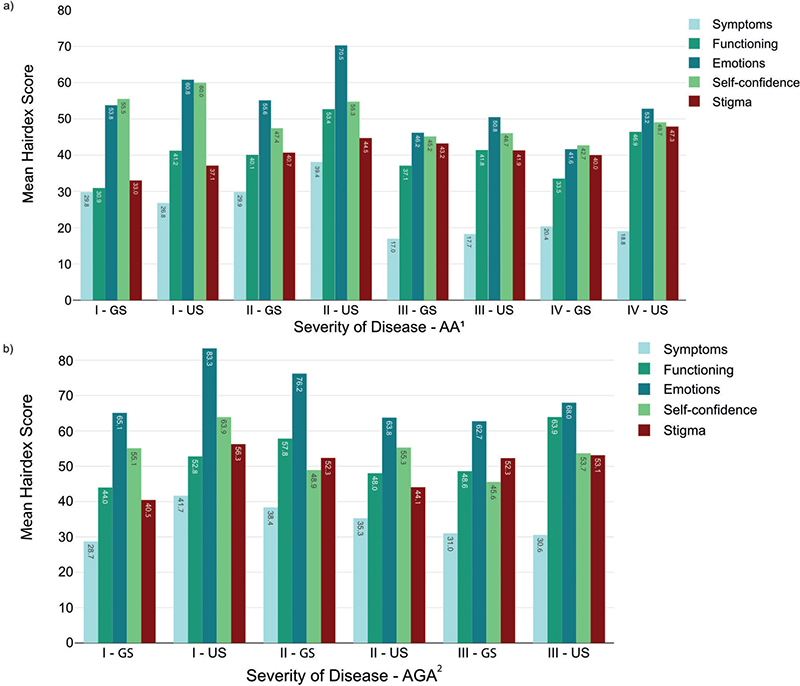
Fig. 2. Hairdex subscale scores for different severity grades of (A) alopecia areata and (B) androgenetic alopecia in the German-speaking and US samples. AA: alopecia areata. AGA: androgenetic alopecia. GS: German-speaking sample. ¹Severity of disease levels: I – less than 30% of scalp affected; II – more than 30% affected; III – Alopecia totalis; IV – Alopecia universalis. 2Severity of disease levels: adapted Hamilton–Norwood/Ludwig scale.
Women reported higher QoL impairment for the subscales symptoms (AA: z = 0.21, p = 0.06, AGA: z = 0.20, p = 0.16) and self-confidence (AA: z = 0.21, p = 0.065, AGA: z = 0.01, p = 0.98) than men, without differences in other subscales. Employed AA participants reported more stigma than self-employed ones (PSQ-score 2.23 (0.57) vs 1.77 (0.41); H(3) = 3.42, p = 0.01), without differences in the AGA sample.
GS-AA vs GS-AGA
Hairdex scores were lower in individuals with AA than AGA (p < 0.001 for all scores; Table II). AA participants reported higher overall stigma (2.22 (0.56)) than AGA participants (1.98 (0.48); p < 0.001; Fig. 2, Fig. 3). AA individuals perceived more positive support (3.96 (0.76) vs 3.53 (0.95); p < 0.001) and less problematic support (2.30 (0.68) vs 2.51 (0.75); p < 0.009) than the AGA sample. The AA sample had higher satisfaction with life (24.6 (6.62) vs 22.2 (6.96); p = 0.002) with a better balance in positive and negative affect (4.52 (9.75) vs –1.04 (10.04); p < 0.001). Differences in anxiety and resilience between AA and AGA were minimal (Table II).

Fig. 3. Perceived Stigmatization Questionnaire subscales scores for different severity grades of (A) alopecia areata and (B) androgenetic alopecia in the German-speaking and US samples. AA: alopecia areata, GS: German-speaking sample. PSQ: Perceived Stigmatization Questionnaire, Sc: Subscale. ¹Severity of disease levels: I – less than 30% of scalp affected; II – more than 30% affected; III – alopecia totalis; IV – alopecia. Severity of disease levels: adapted Hamilton–Norwood/Ludwig scale.
US sample
The mean total PSQ score was 1.95 (0.65), and disease-related QoL subscale scores varied from 26.4 (21.6) for symptoms to 59.7 (27.7) for emotions. Stigma scores increased with severity in the AA sample, but not in the AGA sample (grade I PSQ: 2.68 (1.13) higher than grade II, III (p = 0.10, Fig. 3, Table SV). Hairdex subscales symptoms (H(3) = 32.76, p < 0.001), emotions (H(3) = 16.82, p < 0.001), and self-confidence (H(3) = 19.82, p < 0.001) were higher for AA grades I, II compared with III, IV, peaking at grade II (Fig. 2, Table SV). In AA, disease duration correlated negatively with disease-related QoL subscales (excluding stigma) (–0.30 ≤ r ≤ –0.12, p < 0.001), while AGA showed a similar but weaker trend. Women topped men on QoL subscales symptoms (AA: z = 0.29, p = 0.01; AGA: z = 0.24, p = 0.41), whereas men (PSQ total: AA = 2.23 (0.74), AGA = 3.09 (0.90)) reported higher stigma than women (AA = 1.87 (0.54), z = 0.28, p = 0.02; AGA = 1.97 (0.79), z = 0.72, p = 0.087). Full-time employees reported more stigma than self-employed individuals (PSQ total: 2.01 (0.64) vs 1.77 (0.51), p = 0.02), largely due to the subscale confusing/staring behaviour (p = 0.018), without difference for unemployed participants. No racial differences were found in comparisons for stigma, QoL, disease severity, and well-being.
US-AA vs US-AGA
All AA Hairdex subscale scores were significantly lower than AGA values (0.007 ≤ p ≤.123, Table III). AA had a slightly lower mean PSQ total score than AGA (1.93 (0.60) vs 2.02 (0.84), p = 0.99). The AA group reported stronger positive support (3.35 (1.20) vs AGA: 3.08 (1.16), p = 0.10). Both groups scored similarly in satisfaction with life, positive and negative affect, resilience, mental health, and anxiety.
GS sample vs US sample
The GS sample had higher stigma scores than the US sample (2.22 (0.56) vs 1.98 (0.48); p < 0.001), while the US sample had significantly lower QoL. The GS sample showed higher satisfaction with life (24.63 (6.62) vs 22.24 (6.96); p < 0.001, Table SVI).
Predictors for perceived stigmatization
Resilience, positive social support, satisfaction with life, and Hairdex subscale self-confidence were negatively correlated with perceived stigmatization in both samples (GS: –0.359 ≤ r ≤ –0.264, p < 0.001; US: –0.380 ≤ r ≤ –0.161, p < 0.001, Tables SI and SII).
Predictors included male sex (β =0.135), younger age (β = –0.055), being employed vs self-employed (β =0.225), higher severity (β =0.332), restriction in daily-life function (β =0.007), negative affect (β = 0.023), anxiety (β = 0.011), and higher mood-effect (β =–0.216; Table IV). Family history (β = –0.061), disease duration (β = –0.002), education (β = –0.007), and marital status (β = –0.061) were not significant predictors. Adjusted R2 of model summary was 0.318.
| Predictor | Coefficient | SE | t | p-value | 95% CI |
| Intercept | 1.987 | 0.333 | 5.956 | < 0.001 | |
| Age | –0.055 | 0.002 | –2.005 | 0.045 | [–0.09;–0.001] |
| Gender (reference: female) | 0.135 | 0.085 | 1.996 | 0.017 | [0.07;0.27] |
| Education (reference: low) | |||||
| Moderate | 0.062 | 0.081 | .772 | 0.440 | [–0.44;0.06] |
| High | –0.007 | 0.077 | –0.160 | 0.919 | [–0.15;0.01] |
| Employment (reference: employed) | |||||
| Self-employed | –0.225 | 0.098 | –2.295 | 0.022 | [0.01;0.34] |
| Student | –0.040 | 0.091 | –0.441 | 0.659 | [–0.12;0.14] |
| Unemployed | –0.112 | 0.068 | –1.644 | 0.101 | [–0.22;0.23] |
| Marital status (reference: single) | |||||
| Partnership/Marriage | –0.005 | 0.056 | –0.090 | 0.928 | [–0.11;0.08] |
| Duration of disease | 0.002 | 0.001 | 1.316 | 0.189 | [–9.70e–4;0.01] |
| Family history (reference: yes) | –0.061 | 0.051 | –1.179 | 0.239 | [–0.15;0.04] |
| Severity grades (reference: IV)a | |||||
| l | –0.332 | 0.081 | –4.095 | < 0.001 | [–0.33;0.06] |
| II | –0.176 | 0.060 | –2.900 | 0.004 | [–028.;0.06] |
| III | –0.011 | 0.060 | 1.864 | 0.063 | [–0.06;0.02] |
| Effect of alopecia on mood (reference: High) | |||||
| Moderate | 0.180 | 0.070 | 2.566 | 0.011 | [0.08;0.33] |
| Low | 0.173 | 0.080 | 2.149 | 0.032 | [0.11;0.46] |
| None | 0.216 | 0.105 | 2.047 | 0.041 | [0.18;0.35] |
| Screened Anxiety (GAD–7) | 0.011 | 0.006 | 1.864 | 0.013 | [0.003;0.02] |
| Positive Experience (SPANE–P) | –0.011 | 0.007 | –1.498 | 0.135 | [–0.02;0.01] |
| Negative Experience (SPANE–N) | 0.023 | 0.014 | 2.568 | 0.048 | [0.01;0.07] |
| Emotions (Hairdex) | –0.002 | 0.001 | –1.427 | 0.154 | [–0.004;0.02] |
| Self-confidence (Hairdex) | –0.003 | 0.002 | –1.616 | 0.107 | [–0.007;0.01] |
| Symptoms (Hairdex) | 1.68e–4 | 0.001 | 0.114 | 0.909 | [–0.003;0.09] |
| Functioning (Hairdex) | 0.007 | 0.001 | 3.941 | < 0.001 | [0.01;0.02] |
| Note. R² = 0.318, Adjusted R² = 0.282, F(26,498) = 8.93; aself-reported. 95% CI: 95% confidence intervals; GAD-7: Generalized Anxiety Disorder 7; SPANE-P: Scale of Positive and Negative Experience – Positive Experiences; SPANE-N: Negative Experiences. |
|||||
DISCUSSION
This study examined perceived stigmatization, disease-related QoL, and its predictors among individuals with AA and AGA in GS countries. AA subgroups reported more stigma, but higher QoL than AGA groups. A similar tendency was found in the US sample. The GS sample experienced more stigma but reported higher QoL compared with the US sample. Perceived alopecia-associated stigmatization could be predicted by sociodemographic (male sex, younger age, being employed) and disease-related (higher perceived disease severity, restriction in daily-life function, negative affect, anxiety, and effect on mood) factors. No differences in stigma were found with family history or relationship status.
As disease severity increased, stigmatization worsened across all subgroups, possibly due to increasing visibility and difficulty concealing hair loss as known for other skin conditions like psoriasis and atopic dermatitis (31, 32), whereas disease-related QoL seemed to improve with increasing severity. The severity of AGA increases over time, while AA is more likely to stagnate or progress. The longer the disease duration, the less it affected the QoL of participants with AA, likely due to a form of habituation and acceptance (33). This key difference between the QoL development and perception of stigma throughout the course of the disease highlights the need to investigate stigma and QoL as separate concepts. Despite assumptions that alopecia-related stigma impacts women more (13), our study revealed that men reported perceiving higher levels of stigma and aligns with recent findings (18). The previously described interpretation of negative emotions as weakness among men may lead to self-stigma and decreased help-seeking (34). Study populations have been primarily women, which may understate stigma among men (14).
Women scored higher on the Hairdex subscales for symptoms and self-confidence than men, possibly attributed to women attaching greater importance to appearance, while male baldness is more socially accepted and prevalent (10).
In the US and GS-AA groups, younger participants felt more stigmatized. Age-related changes of perception in stigmatization were reported and attributed to the changed importance of appearance in partner search and ageing (18, 35, 36). Employment predicted stigmatization, especially when compared with self-employed individuals, who may have higher hierarchical positions, and control over schedules and work environment. In previous research, employment-associated stigmatization was primarily influenced by a PSQ subscale describing “:confused/staring behaviour” (18, 23).
Moreover, we encountered a reciprocal effect aligning with the literature: individuals who were more resilient, happy, and socially supported experienced less stigma and QoL impairment (18). This was consistent for AA and AGA of both samples. A relationship emerged as the primary factor contributing to higher levels of resilience, happiness, and social support. However, marital status did not significantly impact stigma in our work, whereas other studies affirmed this association (18, 37).
In the GS sample, the AA group perceived higher stigma, but experienced higher QoL than the AGA group. Gonul et al. similarly observed AA patients having better QoL than AGA patients, without differences in the overall stigma (13). Another study found higher impairment in AA than in AGA, considering the disease’s relapses (5). Although many participants experienced high severity in our study, it shows more perceived stigma in AA than AGA regarding disease progression and phenotypical presentation.
The PSQ was developed for adult burn survivors, showing a mean score of 1.99 (0.55) in the German validation study, similar to the values of this study (AA-GS: 2.22 (0.57), AGA-GS: 1.98 (0.49)) (23), pointing to a similar level of perceived stigma in AA or AGA, making it comparable to disfiguring burns. Prior studies solely utilized the Hairdex, lacking validation for the stigma subscale, or the Internalized Stigma Scale (ISS), validated only for psychiatric disorders (9, 13, 21, 38). Temel et al. (38) compared stigmatization in hair loss with other visible dermatological entities. ISS values in AA patients were comparable to acne vulgaris and higher than in vitiligo patients (38). The course of diseases may explain differences in stigma. AA and acne vulgaris have pronounced and quickly changing clinical appearances, whereas AGA is less reversible. In contrast, vitiligo is slow-progressing, stable, and can affect non-visible areas. Further research suggests different perceptions of stigma across skin conditions, with psoriasis being more affected by social reactions like disgusted faces and alopecia by disease-related internalized self-stigma (32). Van Beugen et al. (18) recently used the PSQ to quantify stigmatization in dermatological entities, including 83 AA patients, with a healthy control group. The AA sample’s mean PSQ total score mirrored our results (18). Contrasting our findings, longer disease duration was a predictor for stigma, suggesting entity-specific effects were lost in the regression averaged over all entities. Longer disease duration and symptoms like pain or itch enhance psychological burden, which in turn intensifies stigmatization, adding mental health stigma (18, 39). Similar to prior findings, the GS and US samples showed differences in stigma, prompting the need to analyse stigma within their respective sociocultural contexts (8). For instance, no differences in stigmatization and QoL impairment were observed across racial identities in the US sample, but may be underestimated by limitations such as unequal sample sizes, known disparities in access to support and education, and the underrepresentation of minority groups in dermatology (40).
To our knowledge, this is the first study to measure stigmatization in AA and AGA in a sample number of this size with tools to measure resilience, social support, happiness, and anxiety. Our study’s strength is identifying predictors and being the first comparing stigma with disease severity and QoL scales for 2 prevalent alopecia types in 2 highly developed regions.
The GS and US samples were predominantly female, with comparable severity, consistent with past studies (9). However, the US sample had a notably older median age and smaller group size, which may have reduced significance. We tested the DLQI only in the US survey for the unvalidated English Hairdex for control purposes. Furthermore, diagnosis, severity, and all other statements were self-reported without medical verification. Severe illness may impact participation, causing potential selection bias.
Future research should explore psychological confounders with stigmatization for a clearer understanding and improved assessment of interventions adapted to their cultural contexts over the long term, i.e., cognitive behavioural therapy (20) to combat anxiety and negative affect, patient education, as well as group interventions strengthening social support and acceptance. This study reveals stigma disparities by entities, gender, and geography besides the visible disease severity. Resilience and social support may mitigate alopecia-related stigma. This research highlights crucial psychosocial aspects pertaining to alopecia, laying the groundwork for stigma-reduction trials.
ACKNOWLEDGEMENTS
Without the support of the Alopecia Areata Deutschland e.V., the National Alopecia Areata Foundation, and the other organizations, this work would not have been possible and the authors are most grateful to them. Moreover, they would like to express their gratitude to Dr Maximilian Schielein for his valuable and helpful recommendations during the planning stage of this research project.
IRB approval status: Reviewed and approved by TUM (Reference: 529/19 S) and the City University of New York (Reference: 2020-0450).
REFERENCES
- Otberg N, Finner AM, Shapiro J. Androgenetic alopecia. Endocrinol Metab Clin North Am 2007; 36: 379–398. https://doi.org/10.1016/j.ecl.2007.03.004
- Khumalo NP, Jessop S, Gumedze F, Ehrlich R. Hairdressing and the prevalence of scalp disease in African adults. Br J Dermatol 2007; 157: 981–988. https://doi.org/10.1111/j.1365-2133.2007.08146.x
- Villasante Fricke AC, Miteva M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol 2015; 8: 397–403. https://doi.org/10.2147/CCID.S53985
- Lee H, Jung SJ, Patel AB, Thompson JM, Qureshi A, Cho E. Racial characteristics of alopecia areata in the United States. J Am Acad Dermatol 2020; 83: 1064–1070. https://doi.org/10.1016/j.jaad.2019.06.1300
- Titeca G, Goudetsidis L, Francq B, Sampogna F, Gieler U, Tomas-Aragones L, et al. ‘The psychosocial burden of alopecia areata and androgenetica: a cross-sectional multicentre study among dermatological out-patients in 13 European countries. J Euro Acad Dermatol Venereol 2020; 34: 406–411. https://doi.org/10.1111/jdv.15927
- Wang H, Pan L, Wu Y. Epidemiological trends in alopecia areata at the global, regional, and national levels. Front Immunol 2022; 13: 874677. https://doi.org/10.3389/fimmu.2022.874677
- Mostaghimi A, Gao W, Ray M, Bartolome L, Wang T, Carley C, et al. Trends in prevalence and incidence of alopecia areata, alopecia totalis, and alopecia universalis among adults and children in a US employer-sponsored insured population. JAMA Dermatol 2023; 159: 411–418. https://doi.org/10.1001/jamadermatol.2023.0002
- Karimkhani C, Boyers LN, Naghavi M, Coffeng LE, Lott JP, Wulf S, et al. The global burden of disease associated with alopecia areata. Br J Dermatol 2015; 172: 1424–1426. https://doi.org/10.1111/bjd.13559
- Schielein MC, Tizek L, Ziehfreund S, Sommer R, Biedermann T, Zink A. Stigmatization caused by hair loss: a systematic literature review. J Dtsch Dermatol Ges 2020; 18: 1357–1368. https://doi.org/10.1111/ddg.14234
- Quittkat HL, Hartmann AS, Dusing R, Buhlmann U, Vocks S. Body dissatisfaction, importance of appearance, and body appreciation in men and women over the lifespan. Front Psychiatry 2019; 10: 864. https://doi.org/10.3389/fpsyt.2019.00864
- Strazzulla LC, Wang EHC, Avila L, Lo Sicco K, Brinster N, Christiano AM, et al. Alopecia areata: an appraisal of new treatment approaches and overview of current therapies. J Am Acad Dermatol 2018; 78: 15–24. https://doi.org/10.1016/j.jaad.2017.04.1142
- Okhovat JP, Marks DH, Manatis-Lornell A, Hagigeorges D, Locascio JJ, Senna MM. Association between alopecia areata, anxiety, and depression: a systematic review and meta-analysis. J Am Acad Dermatol 2023; 88: 1040–1050. https://doi.org/10.1016/j.jaad.2019.05.086
- Gonul M, Cemil BC, Ayvaz HH, Cankurtaran E, Ergin C, Gurel MS. Comparison of quality of life in patients with androgenetic alopecia and alopecia areata. An Bras Dermatol 2018; 93: 651–658. https://doi.org/10.1590/abd1806-4841.20186131
- Schielein MC, Tizek L, Ziehfreund S, Sommer R, Biedermann T, Zink A. Stigmatization caused by hair loss: a systematic literature review. J Dtsch Dermatol Ges 2020; 18: 1357–1368. https://doi.org/10.1111/ddg.14234
- Goffman E. Stigma: notes on the management of spoiled identity. New York: Simon & Schuster, 2009.
- Stangl AL, Earnshaw VA, Logie CH, van Brakel W, Leickness CS, Barré I, et al. The Health Stigma and Discrimination Framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med 2019; 17: 31. https://doi.org/10.1186/s12916-019-1271-3
- Topp J, Andrees V, Weinberger NA, Schäfer I, Sommer R, Mrowietz U, et al. Strategies to reduce stigma related to visible chronic skin diseases: a systematic review. J Eur Acad Dermatol Venereol 2019; 33: 2029–2038. https://doi.org/10.1111/jdv.15734
- Van Beugen S, Schut C, Kupfer J, Bewley AP, Finlay AY, Gieler U, et al. Perceived stigmatization among dermatological outpatients compared with controls: an observational multicentre study in 17 European countries. Acta Derm Venereol 2023; 103: adv6485. https://doi.org/10.2340/actadv.v103.6485
- Germain N, Augustin M, François C, Legau K, Bogoeva N, Desroches M, et al. Stigma in visible skin diseases: a literature review and development of a conceptual model. J Eur Acad Dermatol Venereol 2021; 35: 1493–1504. https://doi.org/10.1111/jdv.17110
- Traxler J, Stuhlmann CFZ, Graf H, Rudnik M, Westphal L, Sommer R. Interventions to reduce skin-related self-stigma: a systematic review. Acta Derm Venereol 2024; 104: adv40384. https://doi.org/10.2340/actadv.v104.40384
- Fischer TW, Schmidt S, Strauss B, Elsner P. Hairdex: Ein Instrument zur Untersuchung der krankheitsbezogenen Lebensqualität bei Patienten mit Haarerkrankungen. Hautarzt 2001; 52: 219–227. https://doi.org/10.1007/s001050051293
- Lawrence JW, Fauerbach JA, Heinberg LJ, Doctor M, Thombs BD. The reliability and validity of the Perceived Stigmatization Questionnaire (PSQ) and the Social Comfort Questionnaire (SCQ) among an adult burn survivor sample. Psychol Assess 2006; 18: 106–111. https://doi.org/10.1037/1040-3590.18.1.106
- Müller A, Smits D, Claes L, Jasper S, Berg L, Ipaktchi R, et al. Validation of the German version of the Perceived Stigmatization Questionnaire/Social Comfort Questionnaire in adult burn survivors. Burns 2016; 42: 790–796. https://doi.org/10.1016/j.burns.2016.01.001
- Revenson TA, Schiaffino KM, Majerovitz SD, Gibofsky A. Social support as a double-edged sword: the relation of positive and problematic support to depression among rheumatoid arthritis patients. Soc Sci Med 1991; 33: 807–813. https://doi.org/10.1016/0277-9536(91)90385-P
- Ramm GC, Hasenbring M. Die deutsche Adaptation der Illness-specific Social Support Scale und ihre teststatistische Überprüfung beim Einsatz an Patienten vor und nach Knochenmarktransplantation. Z Med Psychol 2003; 12: 29–38.
- Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med 2008; 15: 194–200. https://doi.org/10.1080/10705500802222972
- Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess 1985; 49: 71–75. https://doi.org/10.1207/s15327752jpa4901_13
- Diener E, Wirtz D, Tov W, Kim-Prieto C, Choi D-w, Oishi S, et al. New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res 2010; 97: 143–156. https://doi.org/10.1007/s11205-009-9493-y
- Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother Psychosom 2015; 84: 167–176. https://doi.org/10.1159/000376585
- Spitzer RL Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166: 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
- Schlachter S, Sommer R, Augustin M, Tsianakas A, Westphal L. A comparative analysis of the predictors, extent and impacts of self-stigma in patients with psoriasis and atopic dermatitis. Acta Derm Venereol 2023; 103: adv3962. https://doi.org/10.2340/actadv.v103.3962
- van Beugen S, Maas J, van Laarhoven AI, Galesloot TE, Rinck M, Becker ES, et al. Implicit stigmatization-related biases in individuals with skin conditions and their significant others. Health Psychol 2016; 35: 861–865. https://doi.org/10.1037/hea0000404
- Tabolli S, Mozzetta A, Antinone V, Alfani S, Cianchini G, Abeni D. The health impact of pemphigus vulgaris and pemphigus foliaceus assessed using the Medical Outcomes Study 36-item short form health survey questionnaire. Br J Dermatol 2008; 158: 1029–1034. https://doi.org/10.1111/j.1365-2133.2008.08481.x
- Zucchelli F, Sharratt N, Montgomery K, Chambers J. Men’s experiences of alopecia areata: a qualitative study. Health Psychology Open 2022; 9: 20551029221121524. https://doi.org/10.1177/20551029221121524
- Ginsburg IH, Link BG. Feelings of stigmatization in patients with psoriasis. J Am Acad Dermatol 1989; 20: 53–63. https://doi.org/10.1016/S0190-9622(89)70007-4
- Sawant N, Chikhalkar S, Mehta V, Ravi M, Madke B, Khopkar U. Androgenetic alopecia: quality-of-life and associated lifestyle patterns. Int J Trichology 2010; 2: 81–85. https://doi.org/10.4103/0974-7753.77510
- Jankowiak B, Kowalewska B, Krajewska-Kułak E, Khvorik DF. Stigmatization and quality of life in patients with psoriasis. Dermatol Ther (Heidelb) 2020; 10: 285–296. https://doi.org/10.1007/s13555-020-00363-1
- Temel A, Bozkurt S, Senol Y, Alpsoy E. Internalized stigma in patients with acne vulgaris, vitiligo, and alopecia areata. Turkish J Dermatol 2019; 13: 109–116. https://doi.org/10.4103/TJD.TJD_14_19
- Mian M, Silfvast-Kaiser AS, Paek SY, Kivelevitch D, Menter A. A review of the most common dermatologic conditions and their debilitating psychosocial impacts. Int Arch Intern Med 2019. https://doi.org/10.23937/2643-4466/1710018
- Narla S, Heath CR, Alexis A, Silverberg JI. Racial disparities in dermatology. Arch Dermatol Res 2023; 315: 1215–1223. https://doi.org/10.1007/s00403-022-02507-z