REVIEW ARTICLE
Contact Dermatitis Caused by Topical Minoxidil: Allergy or Just Irritation
Alexandra JUNGE, Susanne RADONJIC-HOESLI, Simon BOSSART, Dagmar SIMON, Pierre DE VIRAGH, Robert E. HUNGER, Kristine HEIDEMEYER and S. Morteza SEYED JAFARI
Department of Dermatology, Inselspital, Bern University Hospital, Bern, Switzerland
Topical minoxidil is the mainstay of treatment for androgenic alopecia and is also used off-label for other forms of hair loss. Despite its efficacy and favourable safety profile, the use of minoxidil is associated with various side effects, the most commonly reported of which is contact dermatitis. A clear distinction between allergic contact dermatitis and irritant contact dermatitis to minoxidil is critical for management of androgenic alopecia. This article presents a systematic review of the current literature, evaluating minoxidil-induced allergic contact dermatitis. Of the 251 records identified through the database search, a total of 21 studies were included in the review. Most patients presented with classic signs of contact dermatitis, including erythema, pruritus, and increased scaling of the scalp. Of the patients with positive patch tests, a total of 54 patients showed sensitization to minoxidil itself and 12 patients to vehicle components. Patients with suspected signs of contact dermatitis such as erythema, scaling, and pruritus after minoxidil application should undergo patch testing to confirm or exclude allergy. For the test, the differential reactivity of minoxidil in various vehicles should be considered. Patients who are sensitive to propylene glycol should be offered alternative minoxidil formulations.
SIGNIFICANCE
Despite its efficacy and favourable safety profile, the topical use of minoxidil is associated with various side effects, the most commonly reported of which is contact dermatitis. A clear distinction between allergic contact dermatitis and irritant contact dermatitis to minoxidil is critical for management of androgenic alopecia. This article presents a systematic review of the current literature, evaluating minoxidil-induced contact dermatitis. Patients with suspected signs of contact dermatitis after minoxidil application should undergo patch testing to confirm or exclude allergy. For the test, the differential reactivity of minoxidil in various vehicles should be considered. Patients who are sensitive to propylene glycol should be offered alternative minoxidil formulations.
Key words: allergic contact dermatitis; androgenetic alopecia; contact allergy; contact dermatitis; irritant contact dermatitis; minoxidil.
Citation: Acta Derm Venereol 2025; 105: adv42401. DOI: https://doi.org/10.2340/actadv.v105.42401.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Nov 2, 2024. Accepted after revision: Mar 25, 2025. Published: Apr 27, 2025.
Corr: S. Morteza Seyed Jafari, PD, MD, PhD, Department of Dermatology, Inselspital, Bern University Hospital, Bern, Switzerland. E-mail: Morteza.jafari@insel.ch
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Minoxidil, also known as 2,4-pyrimidinediamine, 6-(1-piperidinyl)-, 3-oxide, was initially developed in the 1970s as a potent peripheral vasodilator for the treatment of severe refractory hypertension (1). In 1987, a topical formulation of minoxidil was developed for the treatment of androgenic alopecia (AGA), first in men and later in women (1). Today, topical minoxidil products typically contain concentrations of 2% or 5% and have become an important therapeutic option in the management of AGA and as an off-label treatment for other forms of alopecia (1–3).
Although minoxidil solutions are generally well tolerated, some patients may experience a local reaction that may result in symptoms such as pruritus and clinical signs such as erythema and eczematous skin reactions. In such cases, allergic reactions, particularly to a specific formulation, should be considered. Patch testing is used to evaluate suspected allergic contact dermatitis. While some literature suggests that contact allergy to minoxidil itself is less common than reactions to its vehicle components, others suggest the opposite (2–5).
Recently, off-label therapy with low-dose oral minoxidil has been shown to be an effective and safe treatment and has been heralded as one of the greatest therapeutic breakthroughs for AGA (6). Although not previously reported in the literature, the potential risk of systemic contact dermatitis with minoxidil should be considered in patients with sensitization to topical minoxidil. Patch testing to differentiate between irritant and allergic contact dermatitis and to identify the causative allergen of minoxidil formulation-induced allergic contact dermatitis (ACD) is essential to identify patients potentially at risk of developing systemic contact dermatitis.
This exciting breakthrough may make systemic treatment with minoxidil more attractive in cases of irritant contact dermatitis. Therefore, a clear distinction between ACD and irritant contact dermatitis (ICD) to minoxidil and vehicles is very important. To clarify this controversial issue, this article presents a systematic review of the current literature evaluating minoxidil-induced allergic contact dermatitis.
Methods
A systematic review of the literature was performed using the PRISMA method in the PubMed database for relevant published studies from January 1990 to July 2024. The terms “minoxidil”, “patch testing”, “contact dermatitis”, “skin adverse effects”, and “allergy”, as well as their synonyms and combinations, were used in the search. Preliminary results were extracted from the databases and documented in a Microsoft Excel file (Microsoft Corp, Redmond, WA, USA), where further selection decisions were documented.
Result lists were merged and duplicates were removed. Titles, abstracts, and publication types were screened for eligibility for full-text evaluation. Exclusion criteria included non-English language, veterinary or ex vivo research, and reviews. There were no geographical restrictions. A thorough evaluation of all available full-text articles was performed using both inclusion and exclusion criteria. All articles focusing on human allergic contact dermatitis, including case reports, were included.
Data points from each publication were then identified and stratified into the following subcategories: study type, patients’ characteristics, and number of patients with allergy to minoxidil/vehicle, clinical presentation, and duration of minoxidil use (Table I).
| No. | Study | Type of study | Patients | Duration of minoxidil usage until appearance of symptoms | Allergy to minoxidil | Allergy to vehicle | Clinical presentation |
| 1 | Ruas et al., 1992 (4) | Case series | 7 female, 1 male; 24–41 years (mean age 33) | 3 weeks–1 year | 8 | 1 | Pruriginous erythema, papules and scaling of scalp and forehead, 2 patients with vesicles |
| 2 | Whitmore, 1992 (22) | Case report | 1 male; 34 years | 4 weeks | 1* | 0 | Irritation, redness, and scaling |
| 3 | Ebner et al., 1995 (21) | Case report | 1 male; 27 years | 4 months | 0 | 1 | Increasing redness, swelling, and scaling on the scalp and ears, associated with burning and itching |
| 4 | Sánchez-Motilla et al., 1998 (11) | Case report | 1 female; 26 years | 1 week | 1 | 0 | Vesicles and pustules over erythematous area on scalp, forehead, and right eyelid |
| 5 | Friedman et al., 2002 (2) | Case series | 7 female, 4 male; 21–69 years (mean age 46.7) | No info. | 4 | 9 | Pruritus and scaling of the scalp |
| 6 | Trattner et al., 2002 (9) | Case report | 1 male; 57 years | 2 years | 1 | 0 | Pigmented contact dermatitis on waist and neck |
| 7 | Sinclair et al., 2002 (14) | Case report | 1 female; 24 years | 3 months | 1 | 0 | Erythematous, scaly scalp with superficial erosions |
| 8 | Hagemann et al., 2005 (15) | Case report | 1 female; 72 years | 8 days | 1 | 0 | Pruritus and scaling of the scalp; later exudative dermatitis and oedema of forehead, periorbital region, and neck |
| 9 | Rodríguez-Martín et al., 2007 (12) | Case report | 1 male; 22 years | 6 days | 1 | 0 | Pruriginous and pustular lesions over an erythematous area on scalp and forehead |
| 10 | Tosti et al., 2009 (5) | Case series | 13 female; N/A | 5 to 26 months (12 months mean) | 7 | 0 | Scalp itching |
| 11 | Corazza et al., 2010 (23) | Case report | 1 female; 60 years | 4 months | 1 | 0 | Eczematous and moderately exudative lesions on scalp |
| 12 | García-Rodiño et al., 2015 (29) | Case report | 1 female; 59 years | 3 months | 1 | 0 | Eczematous lesions affecting face and scalp |
| 13 | La Placa et al., 2016 (10) | Case series | 2 female; 46 and 28 years | Several years and 1 year | 1 | 1 | Scalp psoriasiform contact dermatitis with acute telogen effluvium |
| 14 | Aleid et al., 2017 (25) | Retrospective analysis | Minoxidil was tested in 73 patients | N/A | 5 | N/A | Irritation, itching, and dryness of the scalp |
| 15 | Nagarajan et al. 2021 (24) | Case report | 1 male; 28 years | 15 days | 1 | 0 | Erythema, oedema of ears, cheeks, and infraorbital region, and erythema with papules on scalp |
| 16 | BinJadeed et al., 2021 (13) | Case report | 1 female; 27 years | 4 days | 1 | 0 | Itching scalp, painful swelling over the face |
| 17 | Feryel et al., 2022 (7) | Case report | 1 male; 23 years | 5 days | 1 | 0 | Erythema, itch, increased scaling of the scalp, and cervical lymphadenopathy |
| 18 | Navarro-Triviño et al., 2022 (32) | Case report | 1 male; 38 years | 3 months | 1 | 0 | Eczematous rash on neck |
| 19 | Therianou et al., 2022 (30) | Case series | 9 female; 22–72 years (mean age 47.2) | average of 4.8 years (range, 1–14 years) | 9 | 0 | Scalp pruritus, scaling, eczematous rash |
| 20 | Makris et al., 2023 (8) | Case report | 1 female; 31 years | 15 years on and off | 1 | 0 | Acute localized exanthematous pustulosis (ALEP) |
| 21 | Starace et al., 2023 (16) | Retrospective analysis | 10 female, 2 male, 18–78 years | N/A | 7 | N/A | Erythema, scales, vesicles, and few vascular patterns |
| *Patch testing with 2% minoxidil in alcohol and 2% minoxidil in petrolatum showed no reaction, while 2% minoxidil in propylene glycol produced papulovesicular plaques. | |||||||
Results
A total of 251 primary articles were identified. Of these, 21 articles were eligible according to the inclusion and exclusion criteria (Fig. 1).
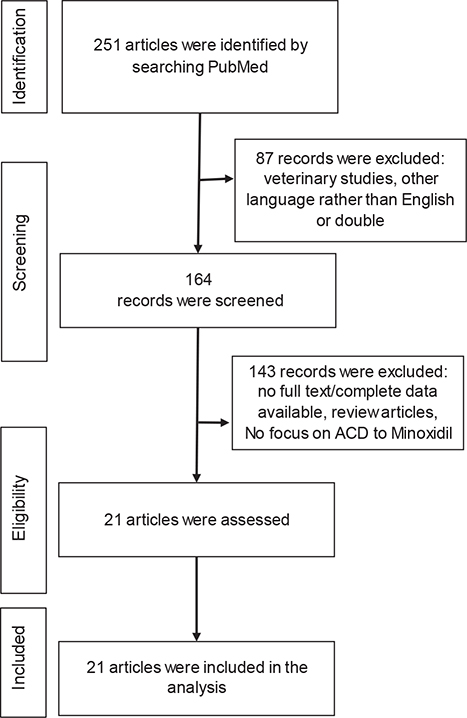
Fig. 1. Flow of information during the different phases of systematic review.
Studies and patients’ characteristics
Of the 21 included articles, 15 were case reports, 4 were case series, and 2 were retrospective analyses. The number of patients ranged from 1 to 73, with a total of 142 patients in all studies. Information on patient age was available in 19 studies, ranging from 18 to 78 years.
Clinical presentation
Onset of symptoms has been reported as early as 4 days after minoxidil administration and as late as 15 years. While most patients presented with classic signs of contact dermatitis – such as erythema, pruritus, and increased scalp scaling – several also exhibited a broader range of clinical symptoms (7–15). The main trichoscopic findings were erythema, white scales, arborizing vessels, and simple red loops (16). In addition to cutaneous manifestations, cervical lymphadenopathy was reported (7). Another interesting paper by Makris et al. (8) reported a case of acute localized exanthematous pustulosis due to contact allergy to minoxidil, while Trattner et al. (9) reported a patient with hyperpigmentation on the waist and neck associated with contact allergy to minoxidil. Furthermore, La Placa et al. (10) described 2 patients with acute telogen effluvium and psoriasiform allergic contact dermatitis.
Patch testing
Of the patients with positive patch tests, a total of 54 patients were allergic to minoxidil and 12 patients were allergic to the vehicle tested. One patient in a case series by Ruas et al. (4), and 2 patients in a case series by Friedman et al. (2), were reported to be allergic to both vehicle and minoxidil. In addition, one of the patients with vehicle allergy tested positive to both propylene glycol and butylene glycol, two different vehicles used in minoxidil formulations (2).
The methods used for patch testing minoxidil showed considerable variation. Typically, concentrations of 1% and 2% in petrolatum are employed for patch testing. However, different studies have explored a range of concentrations and vehicles. For example, Hagemann et al. (15) tested 5% minoxidil in Vaseline (petrolatum), 5% minoxidil in ethanol, Regaine® 2%, and Regaine® 5%. Similarly, Rodríguez-Martín et al. (12) utilized 5% minoxidil in ethanol and 5% minoxidil in propylene glycol for their patch tests. In contrast, Ruas et al. (4) performed patch testing with minoxidil diluted to as low as 0.5%, which produced a positive reaction in 7 patients.
DISCUSSION
Topical minoxidil is the mainstay of treatment for AGA and is also used off-label for other forms of hair loss (17). Our understanding of its mechanism of action on the hair follicle is still limited (18). Its stimulatory effect on follicular keratinocytes and papilla cells in cell culture indicates effects independent of vasodilation and increased blood flow, and promotes hair growth by improving nutrient delivery to hair follicles (17, 18). Long-term use is required for sustained benefit (2). Despite its efficacy and favourable safety profile, the use of minoxidil is associated with several side effects, the most frequently reported of which are scalp irritation, pruritus, and erythema (2, 19). Common causes of these signs and symptoms include irritant and allergic contact dermatitis or exacerbation of seborrheic dermatitis (2, 19). Although clinically similar, these entities should be differentiated for optimal treatment outcome and, more importantly, to allow patients to continue to manage their therapy for hair loss (2).
Topical minoxidil is available in a variety of forms, including solution, foam, and shampoo (17). It contains vehicles that help dissolve the drug in the patient’s body and facilitate tissue absorption (1). The most common vehicle used in minoxidil formulations is propylene glycol, although other formulations based on butylene glycol, ethanol, glycerine, cetyl alcohol and polysorbate are available (2, 20). In cases of suspected allergic contact dermatitis to minoxidil, the differential reactivity of minoxidil in different vehicles should be considered (21, 22). In support of this, Whitmore (22) presented a case report in which patch testing with 2% minoxidil in alcohol and 2% minoxidil in petrolatum showed no reaction, whereas 2% minoxidil in propylene glycol produced papulovesicular plaques (22). This highlights the importance of the correct choice of vehicle for patch testing of specific substances in the evaluation of suspected allergic contact dermatitis (22). Furthermore, the varied approaches to choice of vehicle and concentration of minoxidil in patch testing highlight the complexity and lack of standardizing testing protocols for minoxidil.
Patients allergic to propylene glycol or other vehicle components but not to minoxidil itself are candidates for topical minoxidil formulations that do not contain the allergen, whereas individuals identified as allergic to minoxidil are no longer suitable candidates for the use of minoxidil as a topical treatment for their alopecia (15, 23).
ACD to topical minoxidil products is reported to be most commonly due to the solvents (such as propylene glycol, butylene glycol, and glycerol) and less frequently to the active ingredient minoxidil (23, 24). In a large retrospective study involving 73 patients, minoxidil had a 5.5% positive patch test rate, while propylene glycol showed a higher rate at 8.8% (25). Similarly, the vehicle component propylene glycol was the most common allergen in the case series by Friedman et al. (2). We did not find any literature specifically addressing in vitro sensitization assays for minoxidil. However, a study by Frydrych and Jurowski utilized in silico methods, predicting that minoxidil has a low potential for causing skin irritation (26), with possibly no correlation to sensitization. Nevertheless, data on this topic remain limited.
However, most of the other included studies reported contact allergy to minoxidil rather than to the vehicle components. Nevertheless, it should be noted that the series of allergens used in these studies were not consistent and the patient numbers were small, and a possible selection bias, as discussed later, cannot be ignored (2).
ACD is a delayed-type hypersensitivity reaction that requires an initial sensitization phase with a previously innocuous substance (27). Recent studies have shown that the immune response in ACD is hapten-specific, with both Th-1 and Th-2 responses (27, 28). Clinical manifestations of ACD are mainly eczematous skin reactions (27), but other morphologies, such as pustular allergic contact dermatitis (12), pigmented contact dermatitis (9), lymphoid hyperplasia-like reaction (29), and psoriasiform contact dermatitis (10) have also been reported.
Although in most cases ACD takes a while to occur, in some cases rapid onset (e.g., within a week) has been reported. This reaction may be due to prior sensitization rather than de novo sensitization, which typically takes longer. This could be due to previous exposure to minoxidil in hair loss treatments/products or other formulations leading to an accelerated reaction on re-exposure. Alternatively, cross-sensitization to structurally similar compounds may explain the reaction. Covert or unrecognized previous exposure to minoxidil or related chemicals may also be a factor.
A challenging issue is whether oral minoxidil can be administered in individuals with proven contact allergy to minoxidil. In recent years, oral minoxidil has increasingly been used as an off-label treatment for AGA with good clinical efficacy and optimal tolerability (3, 30). This question is critical because systemic contact dermatitis, i.e., a widespread reaction in individuals sensitized to a contact allergen, might occur after exposure to the same allergen via a different route (30). The exact pathophysiology is unknown; an underlying type IV and possibly type III hypersensitivity reaction have been suggested (30). Cases of systemic contact dermatitis have been reported to propylene glycol, but not to minoxidil (30, 31). The possibility that patients with contact allergy to topical minoxidil could safely tolerate oral minoxidil was proposed under the assumption that systemic skin reactions to topical or oral minoxidil have never been described. Consistent with this, Therianou et al. (30) tested and demonstrated that low-dose oral minoxidil (0.25 mg twice daily) was well tolerated without adverse effects in 9 female patients with known allergy to topical minoxidil. However, the possibility of systemic contact dermatitis cannot be completely ruled out (30, 32). Indeed, some cases of minoxidil-induced Stevens–Johnson syndrome or fatal toxic epidermal necrosis have been reported after systemic minoxidil (33–35). Thus, it is advisable not only to warn patients with known cutaneous allergy to minoxidil, but also to be vigilant in all systemic minoxidil users, as the prevalence of off-label use for hair loss may easily exceed the rare patients treated for hypertension. In addition, further detailed allergologic studies are needed to evaluate the various minoxidil regimens in the context of allergic contact dermatitis to the minoxidil active ingredient and to the different minoxidil formulations. Due to the heterogeneity of test protocols, achieving consistency in this report is challenging. However, based on most studies, a patch test could be conducted using the intended minoxidil product, minoxidil 2% and/or 5% in Vaseline (petrolatum) and/or minoxidil 2% and/or 5% with the usual vehicles – typically propylene glycol, ethanol, water, butylene glycol, cetyl alcohol or glycerine – as well as the vehicle alone. The first assessment should be performed after 48 hours, followed by a second assessment at 72 hours. A possible late evaluation, depending on the substances, may be conducted later (for example, after 7 days) (36).
Limitations
The main limitation of a systematic review is the lack of sufficient data. It generally relies on case reports and studies with small sample sizes, which may introduce a selection bias by disproportionately focusing on unique or notable cases. This is because allergy testing to assess possible contact sensitization is not often performed routinely in daily clinical practice. Therefore, the exact prevalence of ACD to minoxidil remains unknown. Furthermore, a proper meta-analysis is not possible due to the heterogeneity of the studies and the patients included.
Conclusion
Patients with suspected contact dermatitis following use of minoxidil formulations should undergo patch testing to determine a causative allergen. When testing, the differential reactivity of minoxidil in the various vehicles should be considered. In the case of sensitization the advise to the patient should be based on the results of the allergy test. However, large clinical trials are needed to demonstrate its safety in patients with contact allergy to minoxidil.
ACKNOWLEDGEMENTS
Data availability: The data supporting the results of this study are presented in the current paper.
REFERENCES
- Patel P, Nessel TA, Kumar DD. Minoxidil. [Updated 2024 Feb 4]. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing, 2024.
- Friedman ES, Friedman PM, Cohen DE, Washenik K. Allergic contact dermatitis to topical minoxidil solution: etiology and treatment. J Am Acad Dermatol 2002; 46: 309–312. https://doi.org/10.1067/mjd.2002.119104
- Seyed Jafari SM, Heidemeyer K, Hunger RE, de Viragh PA. Safety of antiandrogens for the treatment of female androgenetic alopecia with respect to gynecologic malignancies. J Clin Med 2024; 13: 3052. https://doi.org/10.3390/jcm13113052
- Ruas E, Gonçalo M, Figueiredo A, Gonçalo S. Allergic contact dermatitis from minoxidil. Contact Dermatitis 1992; 26: 57–58. https://doi.org/10.1111/j.1600-0536.1992.tb00876.x
- Tosti A, Donati A, Vincenzi C, Fabbrocini G. Videodermoscopy does not enhance diagnosis of scalp contact dermatitis due to topical minoxidil. Int J Trichology 2009; 1: 134–137. https://doi.org/10.4103/0974-7753.58557
- Ly NY, Fruechte S, Hordinsky MK, Sadick N, Arruda S, Farah RS. Medical and procedural treatment of androgenetic alopecia – where are we? J Am Acad Dermatol 2023; 89: S36–S39. https://doi.org/10.1016/j.jaad.2023.05.004
- Feryel A, Mouna K, Nesrine BS, Hichem B, Jameleddine Z. Unusual clinical presentation of allergic contact dermatitis to topical minoxidil. Contact Dermatitis 2022; 87: 192–193. https://doi.org/10.1111/cod.14117
- Makris M, Kanelleas A, Papapostolou N, Pisimisi M, Katoulis AC. Acute localized exanthematous pustulosis (ALEP) caused by topical application of minoxidil. J Clin Med 2023; 12: 831. https://doi.org/10.3390/jcm12030831
- Trattner A, David M. Pigmented contact dermatitis from topical minoxidil 5%. Contact Dermatitis 2002; 46: 246. https://doi.org/10.1034/j.1600-0536.2002.460416.x
- La Placa M, Balestri R, Bardazzi F, Vincenzi C. Scalp psoriasiform contact dermatitis with acute telogen effluvium due to topical minoxidil treatment. Skin Appendage Disord 2016; 1: 141–143. https://doi.org/10.1159/000441622
- Sánchez-Motilla JM, Pont V, Nagore E, Rodríguez-Serna M, Sánchez JL, Aliaga A. Pustular allergic contact dermatitis from minoxidil. Contact Dermatitis 1998; 38: 283–284. https://doi.org/10.1111/j.1600-0536.1998.tb05747.x
- Rodríguez-Martín M, Sáez-Rodríguez M, Carnerero-Rodríguez A, et al. Pustular allergic contact dermatitis from topical minoxidil 5%. J Eur Acad Dermatol Venereol 2007; 21: 701–702. https://doi.org/10.1111/j.1468-3083.2006.01996.x
- BinJadeed H, Almudimeegh AM, Alomran SA, Alshathry AH. A case of contact allergic dermatitis to topical minoxidil. Cureus 2021; 13: e12510. https://doi.org/10.7759/cureus.12510
- Sinclair RD, Mallari RS, Tate B. Sensitization to saw palmetto and minoxidil in separate topical extemporaneous treatments for androgenetic alopecia. Australas J Dermatol 2002; 43: 311–312. https://doi.org/10.1046/j.1440-0960.2002.00620.x
- Hagemann T, Schlütter-Böhmer B, Allam JP, Bieber T, Novak N. Positive lymphocyte transformation test in a patient with allergic contact dermatitis of the scalp after short-term use of topical minoxidil solution. Contact Dermatitis 2005; 53: 53–55. https://doi.org/10.1111/j.0105-1873.2005.00456b.x
- Starace M, Bruni F, Marcondes MT, Alessandrini A, Piraccini BM. The identification of trichoscopic features of allergic scalp contact dermatitis: a pilot-study of a single center. Ital J Dermatol Venerol 2023; 158: 334–340. https://doi.org/10.23736/S2784-8671.23.07578-3
- Ntshingila S, Oputu O, Arowolo AT, Nonhlanhla P. Khumalo NP. Androgenetic alopecia: an update. JAAD Int 2023; 13: 150–158. https://doi.org/10.1016/j.jdin.2023.07.005
- Messenger AG, Rundegren J. Minoxidil: mechanisms of action on hair growth. Br J Dermatol 2004; 150: 186–194. https://doi.org/10.1111/j.1365-2133.2004.05785.x
- Shadi Z. Compliance to topical minoxidil and reasons for discontinuation among patients with androgenetic alopecia. Dermatol Ther (Heidelb) 2023; 13: 1157–1169. https://doi.org/10.1007/s13555-023-00919-x
- Tata S, Flynn GL, Weiner ND. Penetration of minoxidil from ethanol/propylene glycol solutions: effect of application volume and occlusion. J Pharm Sci 1995; 84: 688–691. https://doi.org/10.1002/jps.2600840605
- Ebner E, Müller E. Allergic contact dermatitis from minoxidil. Contact Dermatitis 1995; 32: 316. https://doi.org/10.1111/j.1600-0536.1995.tb00798.x
- Whitmore SE. The importance of proper vehicle selection in the detection of minoxidil sensitivity. Arch Dermatol 1992; 128: 653–656. https://doi.org/10.1001/archderm.1992.01680150083011
- Corazza M, Borghi A, Ricci M, Sarno O, Virgili A. Patch testing in allergic contact dermatitis from minoxidil. Dermatitis 2010; 21: 217–218. https://doi.org/10.2310/6620.2010.10026
- Nagarajan H, Rai R. Contact dermatitis to minoxidil. Contact Dermatitis 2021; 84: 57. https://doi.org/10.1111/cod.13670
- Aleid NM, Fertig R, Maddy A, Tosti A. Common allergens identified based on patch test results in patients with suspected contact dermatitis of the scalp. Skin Appendage Disord 2017; 3: 7–14. https://doi.org/10.1159/000453530
- Frydrych A, Jurowski K. Toxicity of minoxidil – comprehensive in silico prediction of main toxicity endpoints: acute toxicity, irritation of skin and eye, genetic toxicity, health effect, cardiotoxicity and endocrine system disruption. Chem Biol Interact 2024; 393: 110951. https://doi.org/10.1016/j.cbi.2024.110951
- Tramontana M, Hansel K, Bianchi L, Sensini C, Malatesta N, Stingeni L. Advancing the understanding of allergic contact dermatitis: from pathophysiology to novel therapeutic approaches. Front Med 2023; 10: 1184289. https://doi.org/10.3389/fmed.2023.1184289
- Simon D, Aeberhard C, Erdemoglu Y, Simon HU. Th17 cells and tissue remodeling in atopic and contact dermatitis. Allergy 2014; 69: 125–131. https://doi.org/10.1111/all.12351
- García-Rodiño S, Espasandín-Arias M, Suárez-Peñaranda JM, Rodríguez-Granados MT, Vázquez-Veiga H, Fernández-Redondo V. Persisting allergic patch test reaction to minoxidil manifested as cutaneous lymphoid hyperplasia. Contact Dermatitis 2015; 72: 413–416. https://doi.org/10.1111/cod.12371
- Therianou A, Vincenzi C, Tosti A. How safe is prescribing oral minoxidil in patients allergic to topical minoxidil? J Am Acad Dermatol 2022; 86: 429–431. https://doi.org/10.1016/j.jaad.2020.04.027
- McGowan MA, Scheman A, Jacob SE. Propylene glycol in contact dermatitis: a systematic review. Dermatitis 2018; 29: 6–12. https://doi.org/10.1097/DER.0000000000000307
- Navarro-Triviño FJ, Pegalajar-García MD, Gil-Villalba A, Ruiz-Villaverde R. Allergic contact dermatitis due to minoxidil in a patient with alopecia areata. Actas Dermosifiliogr 2022; 113: S8–S9. https://doi.org/10.1016/j.ad.2021.08.009
- DiSantis DJ, Flanagan J. Minoxidil-induced Stevens–Johnson syndrome. Arch Intern Med 1981; 141: 1515. https://doi.org/10.1001/archinte.1981.00340120123025
- Callen EC, Church CO, Hernandez CL, Thompson ED. Stevens–Johnson syndrome associated with oral minoxidil: a case report. J Nephrol 2007; 20: 91–93.
- Karaoui LR, Chahine-Chakhtoura C. Fatal toxic epidermal necrolysis associated with minoxidil. Pharmacotherapy 2009; 29: 460–467. https://doi.org/10.1592/phco.29.4.460
- Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, Bruze M, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing: recommendations on best practice. Contact Dermatitis 2015; 73: 195–221. https://doi.org/10.1111/cod.12432