SHORT COMMUNICATION
Clinical and Histopathological Characteristics of Buschke–Ollendorff Syndrome: A Case Series
Yidong TAN#, Jinxiang YANG#, Xuanyi CHEN#, Zhirong YAO and Jianying LIANG*
Department of Dermatology, Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine, 1665 Kongjiang Road, Shanghai 200092, P.R. China. *E-mail: jianyingliang@163.com
#These authors contributed equally.
Citation: Acta Derm Venereol 2025; 105: adv42531. DOI: https://doi.org/10.2340/actadv.v105.42531.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Nov 18, 2024. Accepted after revision: Mar 20, 2025. Published: Apr 8, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
INTRODUCTION
Buschke–Ollendorff syndrome (BOS), initially described by Buschke and Ollendorff in 1928, is a rare autosomal dominant genetic disease with an estimated incidence of 1 in 20,000 (1). BOS is characterized by non-tender connective tissue naevi and sclerotic bony lesions (osteopoikilosis [OPK]). Heterozygous loss-of-function mutations in the LEMD3 gene are frequently, but not always, associated with the development of BOS (2). Given its rarity, the clinical signs and characteristic histopathological patterns of BOS have not been systematically studied. In this study, we present a retrospective analysis of 6 BOS cases managed at our institution and offer a comprehensive review of the literature on the dermatological manifestations, histopathological characteristics, and bone disorders among reported cases of BOS.
RESULTS
Clinical characteristics of Buschke–Ollendorff syndrome (BOS) in our case series
A cohort comprising 6 probands has been identified with Buschke–Ollendorff syndrome (BOS), each carrying genetic variations within the LEMD3 gene. Detailed genetic data for these patients are presented in Table SI.
Clinically, all 6 probands presented with multiple yellowish to red papules and nodules, some of which coalesced into cobblestone-like nevoid plaques (Fig. 1A). The number of nodules within each affected area varied among individuals. Probands 1, 5, and 6 presented with clusters of 5 to 18 small nodules of differing diameters, while probands 2 and 3 had only 1–2 nodules per affected area. In our case series, 3 probands had skin lesions distributed across multiple body areas, commonly affecting the thighs, abdomen, and buttocks. All skin lesions exhibited an asymmetrical distribution pattern. Notably, 4 probands developed scars after skin incisions (Fig. 1A). The precise distribution of skin lesions is detailed in Table SI and illustrated in Fig. 1B.
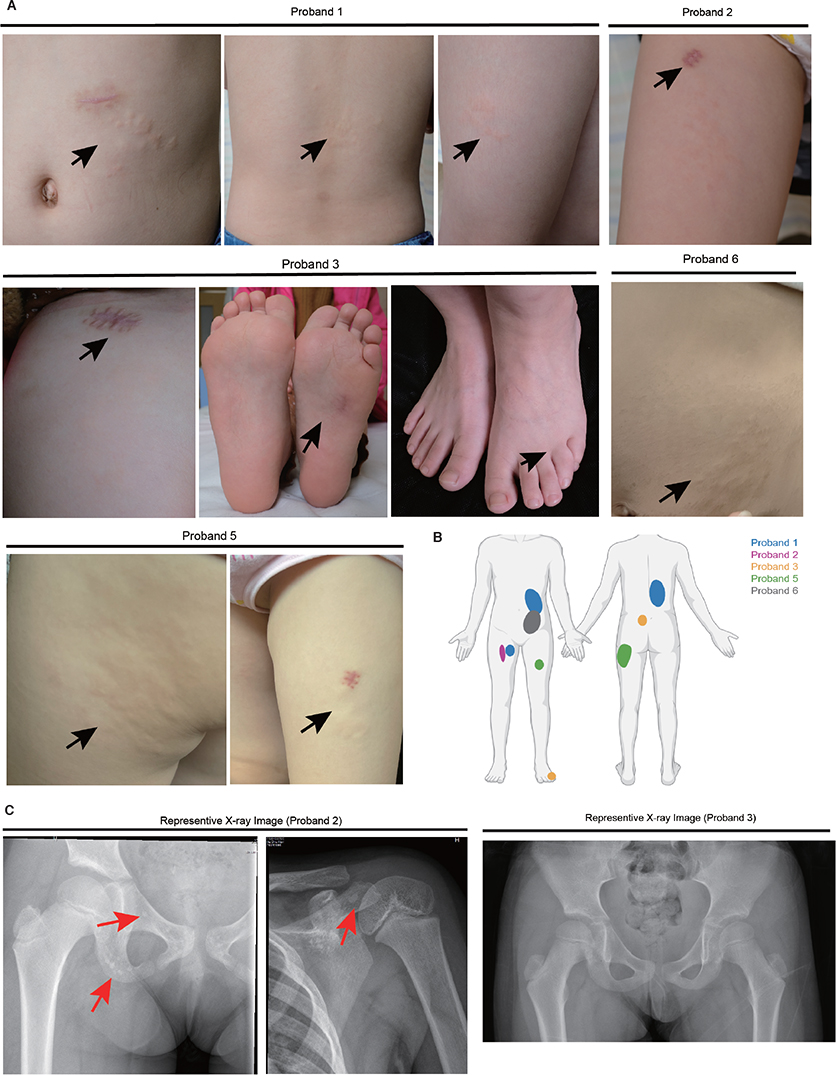
Fig. 1. Clinical characteristics of Buschke–Ollendorff syndrome (BOS) in our case series. (A) Photographs of skin lesions of the patients in our case series. Arrows indicate the location of skin lesion. (B) Diagram depicting the distribution of skin lesions across body regions in our patients. (C) X-ray images of probands 2 and 3. Arrows indicate sites of osteopoikilosis (OPK).
Of the 4 patients who underwent X-ray examination, proband 1 and proband 2 demonstrated osteopoikilosis (OPK) in the pelvis (Fig. 1C), the most frequently affected site. Proband 3 and proband 5 had an X-ray examination of pelvis but did not exhibit any signs of OPK. In addition, the fathers of probands 2 and 6 and the mother of proband 1, who all carry the same mutation as their offspring, did not present with BOS-related skin lesions upon physical examination. The mother of proband 1 tested positive for the SS18-SSX2 fusion gene, a marker of synovial sarcoma, and was diagnosed with synovial sarcoma 10 years ago. Following surgical excision and radiotherapy, her health condition remains stable.
Skin biopsies were obtained from the lesional skin of 5 probands. Victoria blue staining revealed that the dermis of probands 2, 3 (buttocks), 4, 5, and 6 exhibited large, thickened, and haphazardly arrayed elastic fibres (Fig. S1A). Masson’s trichrome staining indicated collagenoma in probands 3 (foot) and 4 (Fig. S1A). Notably, biopsies from a plantar foot nodule and a buttock nodule in proband 3 presented differing histological features, suggesting that lesion location may influence pathological presentation, even within the same individual. Alcian blue staining demonstrated increased interstitial mucin in the reticular dermis of all probands (Fig. S1A). These results underscore the pathological heterogeneity of BOS. A summary of histological findings is provided in Table SI.
Review of clinical characteristics, histopathological findings and mutational spectrum of LEMD3 in documented cases
To comprehensively characterize the genetic, clinical, and histopathological features of BOS, we conducted a detailed analysis of our case series (Table SI) alongside previously documented cases (Table SII). Regarding the distribution of skin lesions, the majority of patients exhibited flesh-coloured nodules on the trunk, thighs, and buttock (Fig. S1B). Lesions on the head, occasionally accompanied by hair loss, are rare but have been documented (3, 4). Nodules on the hands were reported in 2 patients (5, 6), both of whom underwent surgery to alleviate discomfort of hand movement. The onset of skin lesions is variable, with 23% of cases reporting onset before 1 year of age (Fig. S1C), and some presenting at birth (7). Conversely, other cases show a delayed onset, with 1 patient reported to have developed skin lesions at 47 years old (8).
OPK is another defining characteristic of BOS; a summary of OPK locations revealed that the pelvis is the most commonly affected site. Interestingly, OPK also frequently appears in the hand bones (Fig. S1D). In addition to OPK, some BOS patients also exhibit melorheostosis – a form of mesenchymal dysplasia characterized by hyperdense, widening bony cortex resembling dripping candle wax (Fig. S1D). The age of onset for OPK in BOS is challenging to determine. The youngest documented BOS patient with OPK observed on X-ray was 2 years old (9). However, at least 4 documented cases under the age of 6 underwent X-ray examination without any signs of OPK (10–12). We analysed the frequency of OPK occurrence across different age groups. Our findings indicate that OPK was present in 8 out of 12 patients under 6 years of age. In contrast, all patients between the ages of 7 and 18 who underwent X-ray analysis exhibited positive signs of OPK.
Histologically, elastoma is traditionally regarded as the predominant feature of BOS. Nevertheless, an examination of reported histological manifestations in BOS cases reveals that 8% of cases exclusively presented with collagenoma, while 23% displayed a mixed phenotype encompassing both collagenoma and elastoma. Additionally, mucin deposition was observed in a subset of cases, all of which also exhibited either collagenoma or elastoma. Notably, 9% of cases demonstrated all 3 histological features (Fig. S1E). Finally, pain symptoms were reported in 5 cases, though their relationship with OPK remains unclear.
DISCUSSION
In most cases, the manifestations of BOS follow a regular pattern. However, the clinical and pathological features of BOS are highly diverse, and attention should be given to rare presentations. While most skin lesions in BOS are observed on the trunk and thighs, our findings and previous reports indicate that lesions can also appear on less typical locations, such as the feet, hands, and head. Hypertrophic scarring, though uncommon in BOS, was observed in 4 of our probands who developed scars following skin incisions. This finding aligns with a few prior reports that documented scar formation as a clinical manifestation of BOS (13).
Histologically, elastoma is regarded as the predominant feature of BOS; however, our analysis and prior literature indicate that collagenoma and mucin deposition can also be present (14). Notably, 1 proband in our series exhibited lesions on the plantar surface, which showed distinct histopathological characteristics compared with lesions on other body sites, suggesting that lesion location may influence pathological appearance. However, this observation is limited, and further studies are needed to confirm whether mechanical forces at particular body sites may contribute to these variations. In our series, mucin deposition was consistently observed across cases, which highlights a potentially overlooked feature of BOS pathology. Although the presence of mucin in BOS is intriguing, its clinical significance remains uncertain, as does the potential regulatory role of LEMD3 in mucin production. Further studies are essential to explore the mechanisms underlying mucin deposition in BOS.
ACKNOWLEDGEMENT
IRB approval status: The study was performed with the approval of the Ethics Committee of the Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine. Written informed consent was obtained from all patients prior to their participation in the study.
REFERENCES
- Pope V, Dupuis L, Kannu P, Mendoza-Londono R, Sajic D, So J, et al. Buschke–Ollendorff syndrome: a novel case series and systematic review. Br J Dermatol 2016; 174: 723–729. https://doi.org/10.1111/bjd.14366
- Hellemans J, Preobrazhenska O, Willaert A, Debeer P, Verdonk PCM, Costa T, et al. Loss-of-function mutations in LEMD3 result in osteopoikilosis, Buschke–Ollendorff syndrome and melorheostosis. Nature Genetics 2004; 36: 1213–1218. https://doi.org/10.1038/ng1453
- Darr-Foit S, Schliemann S, Schulz S, Elsner P. Buschke–Ollendorff syndrome due to a novel LEMD3 mutation: an unusual case of alopecia. J Dtsch Dermatol Ges 2018; 16: 348–349. https://doi.org/10.1111/ddg.13446
- Aroni K, Kyriazi E, Aivaliotis M, Davaris P. Familial localized connective tissue nevus of the scalp with alopecia (report of a very unusual case). J Eur Acad Dermatol Venereol 2004; 18: 340–341. https://doi.org/10.1111/j.1468-3083.2004.00865.x
- Kobus RJ, Lubbers LM, Coleman CR. Connective tissue nevus and osteopoikilosis in the hand: the Buschke–Ollendorff syndrome. J Hand Surgery 1989; 14: 535–538. https://doi.org/10.1016/S0363-5023(89)80019-X
- Brodbeck M, Yousif Q, Diener PA, Zweier M, Gruenert J. The Buschke–Ollendorff syndrome: a case report of simultaneous osteo-cutaneous malformations in the hand. BMC Res Notes 2016; 9: 294. https://doi.org/10.1186/s13104-016-2095-2
- Waller B, Al-Jasser M, Lam JM. An 8-year-old boy with multiple yellow papules and bony lesions. Pediatr Dermatol 2013; 30: 261–262. https://doi.org/10.1111/j.1525-1470.2012.01762.x
- Trattner A, David M, Rothem A, Ben-David E, Sandbank M. Buschke–Ollendorff syndrome of the scalp: histologic and ultrastructural findings. J Am Acad Dermatol 1991; 24: 822–824. https://doi.org/10.1016/0190-9622(91)70123-J
- Fernández-Faith E, Kress D, Piliang M, Sachdeva M, Vidimos A. Buschke–Ollendorff syndrome and bilateral cutaneous syndactyly. Pediatr Dermatol 2012; 29: 661–662. https://doi.org/10.1111/j.1525-1470.2011.01417.x
- Condorelli A, Musso N, Scuderi L, Condorelli DF, Barresi V, De Pasquale R. Juvenile elastoma without germline mutations in LEMD3 gene: a case of Buschke–Ollendorff syndrome? Pediatr Dermatol 2017; 34: e345–e346. https://doi.org/10.1111/pde.13287
- Kratzsch J, Mitter D, Ziemer M, Kohlhase J, Voth H. Identification of a novel point mutation in the LEMD3 gene in an infant with Buschke–Ollendorff syndrome. JAMA Dermatol 2016; 152: 844–845. https://doi.org/10.1001/jamadermatol.2016.0350
- Yadegari M, Whyte MP, Mumm S, Phelps RG, Shanske A, Totty WG, et al. Buschke–Ollendorff syndrome: absence of LEMD3 mutation in an affected family. Arch Dermatol 2010; 146: 63–68. https://doi.org/10.1001/archdermatol.2009.320
- Korekawa A, Nakano H, Toyomaki Y, Takiyoshi N, Rokunohe D, Akasaka E, et al. Buschke–Ollendorff syndrome associated with hypertrophic scar formation: a possible role for LEMD3 mutation. Br J Dermatol 2012; 166: 900–903. https://doi.org/10.1111/j.1365-2133.2011.10691.x
- Xu Z, Yang C, Xue R. Buschke–Ollendorff syndrome with LEMD3 germline stopgain mutation p.R678* presenting as multiple subcutaneous nodules with mucin deposition. J Cutan Pathol 2021; 48: 77–80. https://doi.org/10.1111/cup.13771