SHORT COMMUNICATION
Löfgren’s Syndrome Following BNT162b2 mRNA COVID-19 Vaccination and Subsequent Plaque-type Cutaneous Sarcoidosis after its Resolution
Masahiro OKA1 and Takeshi FUKUMOTO2
1Department of Dermatology, Kita-Harima Medical Center, 926-250 Ichiba-cho, Ono City, Hyogo 675-1392, Japan, and 2Division of Dermatology, Department of Internal Related, Kobe University Graduate School of Medicine, Kobe, Japan. E-mail: masahiro_oka@kitahari-mc.jp
Citation: Acta Derm Venereol 2025; 105: adv42566. DOI: https://doi.org/10.2340/actadv.v105.42566.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Nov 24, 2024. Accepted after revision: May 19, 2025. Published: Jun 12, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Sarcoidosis is a multisystem inflammatory disease of unknown aetiology characterized by the formation of noncaseating granulomas in various organs, including the lungs, lymph nodes, skin, eyes, liver, spleen, and bone (1). This illness can present acutely or have a chronic course. Löfgren’s syndrome (LS), initially described by Sven Löfgren in 1953 (2), is an acute form of sarcoidosis characterized by the symptom triad of bilateral hilar lymphadenopathy (BHL), polyarthritis, and erythema nodosum (1, 3, 4).
The skin is involved in 20%–35% of all cases of sarcoidosis, and it is the second or third most commonly affected organ in such cases (1, 5–7). Cutaneous sarcoidosis is classified into specific lesions with histopathologically evident noncaseating granulomas and nonspecific lesions that develop as a result of a reactive process that does not form granulomas (6, 7). Specific lesions include papules, nodules, and plaques, and nonspecific lesions include erythema nodosum, which is mostly observed with LS (1).
Several vaccines have been developed against coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (8). Recently, Rademacher et al. (9) reported 2 cases of LS that developed after COVID-19 vaccination. One patient developed LS symptoms 3 days after the second primary vaccination (first vaccination ChadOx-1, Astra Zeneca; second vaccination CX-024414, Moderna). In the other patient, the symptoms started 28 days after the first primary vaccination (ChadOx-1, Astra Zeneca). In this article, we describe the first case of LS following the mRNA-based BNT162b2 (10) COVID-19 vaccination. Interestingly, the patient in our case developed plaque-type cutaneous sarcoidosis after LS resolution.
CASE REPORT
A 57-year-old Japanese woman presented to the Department of Rheumatology of Kita-Harima Medical Center with a 1-month history of polyarthralgia in the shoulders, elbows, and wrists, as well as bilateral erythematous swelling of the lower legs with oedema and pain. Both started within 1 week of receiving the first primary dose of the BNT162b2 vaccine. She also reported 2 incidents of fever that normalized spontaneously within 1 month after vaccination. The patient had a history of diabetes mellitus and underwent follow-up at our centre’s Department of Diabetes and Endocrine Disease for more than 9 years.
On physical examination, both shoulder joints were tender without swelling, whereas both metacarpophalangeal joints were swollen but non-tender. Both lower legs were erythematous, oedematous, and tender, predominantly on the anterior side (Fig. 1A). Several diagnostic examinations were planned to determine the cause of polyarthralgia, and treatment with celecoxib was prescribed at the time of the first consultation despite the lack of a definitive diagnosis. Skin lesions of the lower legs were diagnosed as cellulitis, treated with cefdinir and celecoxib, and improved within 3 weeks.
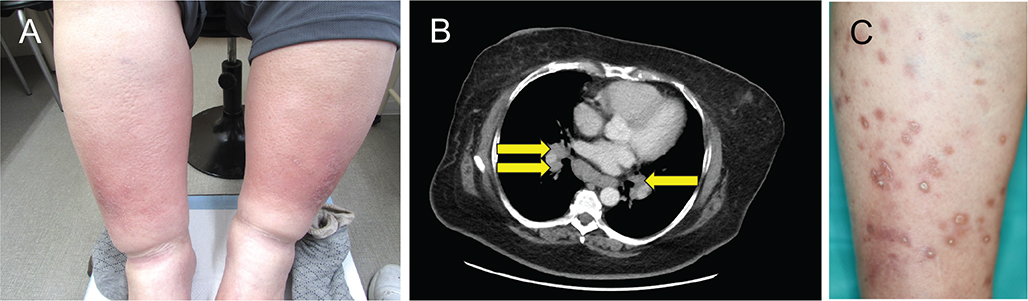
Fig. 1. Clinical and radiographic findings. (A) Clinical findings of the lower legs at the first presentation at the Department of Rheumatology. Bilateral erythematous swelling with oedema, predominantly affecting the extensor surfaces of the lower legs. (B) Radiographic findings of the chest. Chest computed tomography image shows bilateral hilar lymphadenopathy (yellow arrows). (C) Clinical findings of the skin lesions at the first presentation at the Department of Dermatology after resolution of the symptoms of Löfgren’s syndrome. Multiple circular- or oval-shaped plaques up to 1.5 cm in diameter are observed predominantly on the extensor surfaces of the lower leg, many of which have thick scales in their centre.
Bone and joint radiography findings of the extremities were normal except for mild soft tissue swelling. Musculoskeletal ultrasonography revealed neither bursitis nor tendinous synovitis. Chest radiography and chest computed tomography (CT) revealed BHL (Fig. 1B). Echocardiography findings were unremarkable. Histological examination of mediastinal lymph node samples obtained by endobronchial ultrasound-guided transbronchial needle aspiration demonstrated noncaseating epithelioid granulomas. Laboratory tests revealed an elevated C-reactive protein level (5.96 mg/dL: normal, 0–0.3 mg/dL). Other laboratory values, including angiotensin-converting enzyme level, were within the normal ranges. Therefore, sarcoidosis with pulmonary (stage I) and articular (polyarthritis) involvement was diagnosed within 2 months of the first presentation. Neither cardiac nor ocular manifestations were observed. Celecoxib treatment of polyarthritis for 11 months effectively provided nearly complete improvement. BHL resolved spontaneously within 13 months of the first presentation.
Approximately 8 months and 6 months after resolution of BHL and polyarthritis, respectively, multiple asymptomatic, scaly eruptions developed on the lower legs. The patient presented to the centre’s Department of Dermatology 2 months later. Dermatological examination revealed multiple circular and oval red-brown plaques up to 1.5 cm in diameter, predominantly on the extensor surface of the lower legs. The central portion of many of these plaques was slightly depressed and covered with thick scales (Fig. 1C). The skin surface of the distal one-third of the lower legs was covered with diffuse, faint, brown patches. Histological examination of the scaly plaques revealed prominent hyperkeratosis, mounds of parakeratosis, slight acanthosis, and slight spongiosis in the epidermis (Fig. 2A). Noncaseating epithelioid granulomas containing multinucleated giant cells were scattered from the upper dermis close to the epidermis to the lower dermis (Fig. 2B).
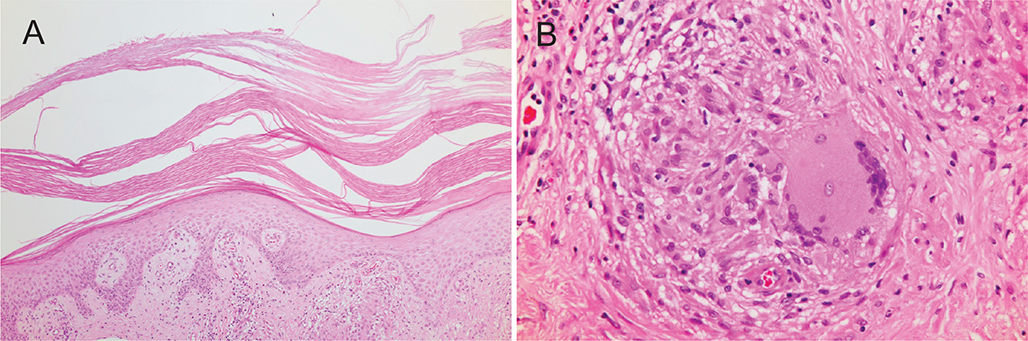
Fig. 2. Histological findings of a scaly plaque. (A) Prominent hyperkeratosis with parakeratosis and slight acanthosis in the epidermis (haematoxylin and eosin stain: original magnification ×40). (B) Noncaseating epithelioid granulomas containing multinucleated giant cells in the dermis.
Based on these clinical and histological findings, the skin lesions were diagnosed as plaque-type cutaneous sarcoidosis. Previous erythematous swelling of the lower legs was re-evaluated from a dermatological perspective, and the diagnosis of cellulitis was changed to erythema nodosum based on the symmetry, predominant presence of lesions on the anterior surface of the lower legs, and coexistence of sarcoidosis. Topical betamethasone butyrate propionate therapy was administered but did not result in improvement. After admission, the patient was treated with oral prednisolone 30 mg/day (0.33 mg/kg/day); however, the clinical response was poor, with only flattening of the plaque lesions. Pharmacotherapy was discontinued, and the skin lesions were observed without treatment.
DISCUSSION
Although the exact aetiology of LS is unknown, a genetic background has been suggested; furthermore, LS is closely related to HLA B8, HLA A1B8, and HLA DR3 (3). Unfortunately, data regarding the HLA types of our patient were not obtained. In the present case, LS developed immediately after the first primary dose of the BNT162b2 vaccine, suggesting that BNT162b2 vaccination is aetiologically associated with LS development. Although the vaccine used in the present case is different from those in the cases reported by Rademacher et al. (9), who reported the 2 cases of LS following COVID-19 vaccination, our case strengthens the authors’ suggestion that LS can occur as a de novo immunological reaction to COVID-19 vaccines, irrespective of their mode of action.
Diverse cutaneous adverse reactions associated with COVID-19 vaccines have been reported (11, 12). In addition, many cases of COVID-19 vaccines-triggered systemic and ocular sarcoidosis without cutaneous sarcoidosis have been reported (13). However, reports of cutaneous sarcoidosis triggered by COVID-19 vaccines are very rare (13). Our patient developed plaque-type cutaneous sarcoidosis after the resolution of LS. Although it remains unclear whether the plaque-type cutaneous sarcoidosis is triggered by BNT162b vaccination or not, this is the first reported case of a patient with LS developing erythema nodosum along with a different type of cutaneous sarcoidosis at different time points.
Patients with typical LS have the symptom triad of BHL, polyarthritis, and erythema nodosum. However, many sarcoidosis patients with BHL and polyarthritis but not erythema nodosum have been identified and diagnosed with an LS variant (3, 14, 15). In the present case, the skin lesions on the lower legs were diagnosed as cellulitis without a histological examination at the first presentation to the Department of Rheumatology. It has been recognized that the lesions of erythema nodosum appear similar to cellulitis in many LS cases (14). If the erythematous swelling of the lower legs at the first presentation was not erythema nodosum, the patient’s diagnosis would have been an LS variant.
REFERENCES
- Sève P, Pacheco Y, Durupt F, Jamilloux Y, Gerfaud-Valentin M, Isaac S, et al. Sarcoidosis: a clinical overview from symptoms to diagnosis. Cells 2021; 10: 766. https://doi.org/10.3390/cells10040766
- Löfgren S. Primary pulmonary sarcoidosis. I. Early sign and symptoms. Acta Med Scand 1953; 142: 424–431. https://doi.org/10.1111/j.0954-6820.1953.tb07039.x
- Mañá J, Gomez-Vaquero C, Montero A, Salazar A, Marcoval J, Valverde J, et al. Löfgren’s syndrome revisited: a study of 186 patients. Am J Med 1999; 107: 240–245. https://doi.org/10.1016/S0002-9343(99)00223-5
- Flores R, Caridade S. Löfgren’s syndrome: clinical presentation, clinical course, and literature review. Cureus 2023; 15: e33651. https://doi.org/10.7759/cureus.33651
- Marchell R, Judson MA. Chronic cutaneous lesions of sarcoidosis. Clin Dermatol 2007; 25: 295–302. https://doi.org/10.1016/j.clindermatol.2007.03.007
- Haimovic A, Sanchez M, Judson MA, Prystowsky S. Sarcoidosis: a comprehensive review and update for the dermatologist. Part I. Cutaneous disease. J Am Acad Dermatol 2012; 66: 699.e1–699.e18. https://doi.org/10.1016/j.jaad.2011.11.965
- Koneti J, Cherukuri SP, Gadde S, Kalluru R, Chikatimalla R, Dasaradhan T. Sarcoidosis and its dermatological manifestations: a narrative review. Cureus 2022; 14: e28053. https://doi.org/10.7759/cureus.28053
- Sharif N, Alzahrani KJ, Ahmed SN, Dey SK. Efficacy, immunogenicity and safety of COVID-19 vaccines: a systematic review and meta-analysis. Front Immunol 2021; 12: 714170. https://doi.org/10.3389/fimmu.2021.714170
- Radmacher JG, Tampe B, Korsten P. First report of two cases of Löfgren’s syndrome after SARS-CoV-2 vaccination: coincidence or causality? Vaccines 2021; 9: 1313. https://doi.org/10.3390/vaccines9111313
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020; 383: 2603–2615. https://doi.org/10.1056/NEJMoa2034577
- McMahon DE, Amerson E, Rosenbach M, Lipoff JB, Moustafa D, Tyagi A, et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: a registry-based study of 414 cases. J Am Acad Dermatol 2021; 85: 46–55. https://doi.org/10.1016/j.jaad.2021.03.092
- Avallone G, Quaglino P, Cavallo F, Roccuzzo G, Ribero S, Zalaudek I, et al. SARS-CoV-2 vaccine-related cutaneous manifestations: a systematic review. Int J Dermatol 2022; 61: 1187–1204. https://doi.org/10.1111/ijd.16063
- Seol JE, Jang SH, Yun HW, Ahn SW, Kim H. A case of cutaneous sarcoidosis with pulmonary involvement after SARS-CoV-2 mRNA vaccination. JAAD Case Rep 2024; 50: 47–50. https://doi.org/10.1016/j.jdcr.2024.05.019
- Caplan HI, Katz WA, Rubenstein M. Periarticular inflammation, bilateral hilar adenopathy and a sarcoid reaction. Arthritis Rheum 1970; 13: 101–111. https://doi.org/10.1002/art.1780130201
- Torralba KD, Quismorio FP Jr. Sarcoid arthritis: a review of clinical features, pathology, and therapy. Sarcoidosis Vasc Diffuse Lung Dis 2003; 20: 95–103.