REVIEW ARTICLE
Introducing Social Dermatology
Elisabeth M. M. CHRISTENSEN1,2, Gregor B.E. JEMEC1–3, Ditte Marie L. SAUNTE1–3# and Ole Steen MORTENSEN4#
1Department of Dermatology, Zealand University Hospital, Roskilde, 2Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, 3Department of Allergy, Dermatology and Venereology, Copenhagen University Hospital – Herlev and Gentofte Hospital, Hellerup, and 4Department of Public Health, Section of Social Medicine, University of Copenhagen, Copenhagen, Denmark
#Shared senior authorship.
Increasing evidence supports the idea that social determinants of health, e.g., educational attainment, employment, and community context, directly affect health status. Researchers are also beginning to explore the impact of social factors on skin diseases, though no formalized research field, to the authors’ knowledge, provides a structured framework for such practice. In this article, the novel global research field of ”Social Dermatology” is introduced to structure academic knowledge in dermatology. The aim is to outline how this paradigm shift could transform both clinical practice and scientific research. The field will explore subjects studied within the medical field of Social Medicine, adapting and applying them to the context of dermatology. Specifically the article will address the social determinants of health in dermatology, and elaborate on human functioning as an approach to a more comprehensive understanding of health in people with skin diseases. This approach enables the integration of rehabilitative aspects, with the International Classification of Functioning (ICF) guiding research and clinical practice to promote more equitable and patient-centred care. To address methodological and communicative opportunities it is suggested that a theoretical web-based social incubator be developed. A formal agreement on the values, interests, and challenges of this new field is needed for a sustainable research effort.
SIGNIFICANCE
Skin health is deeply connected to our life circumstances, and dermatological conditions can significantly impact a person’s social and emotional well-being. In this article, we propose the creation of “Social Dermatology”, a new field that focuses on the interactions between skin diseases and social factors such as the environment and socioeconomics. By addressing how life experiences influence skin conditions – and how these conditions in turn shape lives – this perspective can improve research, patient care, and outcomes. With growing scientific evidence supporting these connections, our framework provides the initial tools and language needed to foster collaboration in this important emerging field.
Key words: social dermatology; SDOH; ICF; social medicine; dermatology; rehabilitation.
Citation: Acta Derm Venereol 2025; 105: adv42622. DOI: https://doi.org/10.2340/actadv.v105.42622.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Corr: Elisabeth M.M. Christensen, MD, Department of Dermatology, Zealand University Hospital, Sygehusvej 10, DK-4000 Roskilde, Denmark. E-mail: emey@regionsjaelland.dk
Submitted: Jan 20, 2025. Accepted after revision: Feb 3, 2025. Published: Mar 3, 2025.
Competing interests and funding: EMMC and OSM have no relevant financial or non-financial conflicts of interest to declare. DMS reports personal fees and grants from Galderma, Janssen, Leo Pharma, Pfizer, UCB, AbbVie, Sanofi, and Novartis outside the submitted work. GBJ reports grants from Leo Research Foundation during the conduct of the study; personal fees from AbbVie, personal fees from Chemocentryx, personal fees from Kymera, personal fees from Leo Pharma, personal fees from Coloplast, grants and personal fees from Novartis, grants and personal fees from UCB, grants and personal fees from Inflarx, grants from Janssen-Cilag, and grants from Serono, grants from Regeneron, outside the submitted work.
This work was supported by a grant from Region Sjælland (grant number: R29-A1717).
Introduction
The ultimate goal of adapting diagnosis, prognosis, and therapy to a given individual is not restricted to a biological understanding. Health and disease are evidently impacted by the lived experience best understood in a bio-psychosocial perspective. No man is an island, and particularly not in dermatology, a unique field due to the obvious pathology immediately recognizable by society (1). It is therefore encouraging for patients that a growing body of literature is addressing the psychosocial aspects in dermatology. However, as psychosocial aspects of medicine is central to the field of social medicine (2), it is surprising how neglected the potential benefits of a shared collaborative methodological approach between dermatology and social medicine have been. We envision that such a collaboration would ensure a more qualified understanding of the factors impacting skin health.
Addressing social factors may seem time consuming and outside the scope of dermatology, but it is known that social factors such as poor living conditions and lack of appropriate care directly impact clinically relevant parameters such as the effectiveness of treatment in dermatology (3). Understanding and addressing the social factors’ effect on clinical manifestations may result in fewer flare-ups and reduced need for consultations, and help avoid unrealistic treatment options and unnecessary interventions – ultimately allowing for better allocation of time and improved adherence.
Implementing a social approach in the understanding of diseases may better prepare dermatologists to do research and clinical work that captures onset, disease outcomes, and consequences for health. When addressing onset and outcomes of skin diseases it is appropriate to address the social determinants of health (SDOH), a concept that social medicine works with innately (2). The SDOHs are “the non-medical factors that influence health outcomes. They are the conditions in the places where people live, learn, work, and play” (4). For example, SDOHs such as socioeconomic status (SES), occupation, race and ethnicity, geographic conditions, or gender play a role in disease prevalence and outcomes in dermatology (5). Studies have recently been published providing ideas on how to initially address SDOH in dermatology (6, 7), but more in-depth knowledge is needed.
When addressing the consequences of social factors for skin diseases another approach commonly used in social medicine can be of use. This approach is the conceptualization of human functioning, comprising both biological health and actual lived health, called “The International Classification of Functioning” (ICF) (8).
ICF is a framework describing the multi-directionality of health and disability. It was conceptualized in 2001 and officially recognized by all 191 WHO members in 2021 as the international standard to describe and measure health and disability (8). The model consists of the following domains: “health condition”, “activities”, “participation”, “body functioning and structures”, “environmental factors”, “personal factors”. The combined impact of these components describes functioning and disability in a generic setting across medical fields, diseases, and nations (8). The model is thus designed to facilitate communication between healthcare providers across diseases and nations and thus enables dermatologists to address social factors across medical fields.
By implementing both the ICF and SDOH in dermatological practice the field has a sociological framework of working with disease onset, outcomes, and consequences in social dermatology (see Fig. 1, Part A for an illustration of the proposed framework).
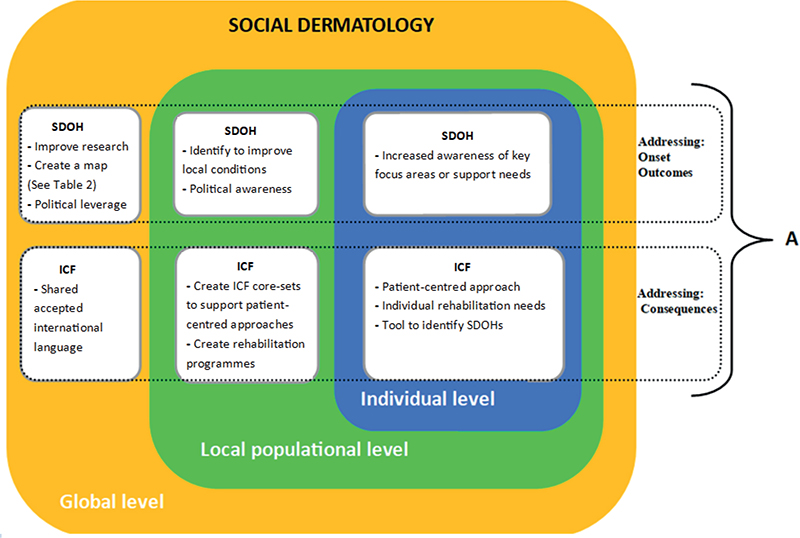
Fig. 1. Framework of social dermatology. The figure illustrates the theoretical framework of the proposed field of social dermatology. A focus on SDOH and ICF allows for a patient-centred approach with a universal language that factors in relevant social influences on health. Part A illustrates how the social determinants of health (SDOH) can be used to address disease onset and outcomes, whereas the International Classification of Functioning (ICF) by the WHO can be used to address health consequences. Furthermore, the figure illustrates examples of how to work with SDOH and ICF on 3 different levels: an individual level, a local populational level, and a global level.
The objective of this narrative review is to facilitate the integration of a social perspective in dermatological care and research. We wish to suggest the development of the research field “Social Dermatology”. This article will therefore provide a narrative overview of the current research and relevance of SDOH and ICF in dermatology and suggest how to move forward with this new proposed research field.
MATERIALS AND METHODS
PubMed was searched carefully for articles on skin diseases in relation to: (i) the ICF model OR (ii) SDOH. The search strands are listed in Tables SI–SIII. As we wished to gain an overview of research interests, we included all relevant studies in English and imposed no other restrictions.
RESULTS
Tables I and II present results on SDOH in dermatology.
| Eczema | In general, lower income is associated with more frequent eczema symptoms compared to patients with higher income (28). Lower income is associated with a higher risk of not having initiated any treatment. Health literacy has also been identified as a barrier for health in eczema populations with low income Furthermore, a nationwide cross-sectional survey concluded that perinatal health problems were associated with eczema, recognizing the importance of research in maternal health and childhood development (28) Atopic dermatitis (AD): A phenomenon is present in AD research where populations with higher SES, usually measured by employment and income, have an increased AD prevalence (29), though inconclusive or contradictory studies on the topic are present (30). This phenomenon may be contributed to higher health literacy (and thus higher help-seeking behaviour) of this population, and several studies indicate that lower SES is associated with more severe and persistent AD (30). Environment is another social factor that can influence AD such as air pollution, chemical exposure, wet work, contact allergies, and psychosocial stressors (14), as well as environmental exposures in utero (14) Several studies are occupied with race and ethnicity in AD and exemplify social stratification; there is not sufficient evidence to explain the genetic disparities reported among racial and ethnic groups (29), however, children with African or Latino background are more likely to have persistent AD, increasing their risk of having a greater AD burden and poorer overall health (29). Also, studies have reported lack of access to healthcare as a barrier for children with black racially backgrounds, and racially black and Latino populations have increased risk of harmful environmental exposures, which can impact the severity of AD (29). A systematic review found AD to be associated with increased sick leave and disability pension. The impact of AD on change/loss of job and educational or job choice are reported more inconclusively (31). Occupational contact dermatitis OCD: OCD is common in occupations such as cleaners, hairdressers, nurses, and metal workers (32). Though the main risk factors include environmental exposures other risk factors include not using protective gloves and having a low educational level (32, 33). |
|
| Skin cancer | In general, low SES is an independent predictor of survival in patients with skin cancer (5). Melanoma: Melanoma is diagnosed at a later stage in minorities exemplifying social stratification as patients with dark pigmented skin can be less aware of skin cancer risk, less likely to use sun protection, and less likely to undergo a full body skin examination (16). Patients with a higher educational level presents with thinner tumours (34). Physicians can be inclined to provide less knowledge to patients with lower education on melanoma risk factors, screening, and self-detection methods and be part of the reason for the limited health literacy of these patients (5). Also being uninsured or living in rural areas are risk factors for presenting with more advanced disease and being less likely to receive treatment and experience delays in diagnostics (5). There is also a geographical factor in melanoma outcomes, more specifically a correlation of melanomas and geographical longitude (35) attributed to greater sun exposure but also to the lifestyle of these provinces such as a more prominent beach culture Squamous cell carcinoma (SCC) Occupational exposure to UV is associated with an increased risk of SCC (36). |
|
| Hidradenitis suppurativa (HS) | There is a higher incidence of HS in lower SES as well as in ethnic populations, such as African Americans, according to case-control studies (37). Smoking and obesity are associated with HS, and treatment involves medicine in combination with lifestyle changes. Among lower SES and ethnic populations, there is a higher rate of both smoking and obesity (5). These lower SES populations with HS are at even more risk as HS is associated with lower rates of employment, higher overall indirect costs, and slower income growth. Furthermore, patients with HS of racially black background have been reported to hold a lower level of education (5). Patients with HS often report poor access to dermatological care, potentially attributable to the lengthy diagnostic delay, which averages 7–10 years. Moreover, the condition imposes a significant psychosocial burden, profoundly influencing social inclusion and exclusion (24). |
|
| Psoriasis | Patients are at risk of having a higher severity of psoriasis and lower disease control if they have a lower educational level (5), and employment rates in patients with psoriasis are lower compared to controls in the years prior to and following diagnosis (38). Low maternal educational attainment and income is associated with psoriasis (39). Social in-/exclusion also has an impact on psoriasis as stigma is associated with severity, poor quality of life, and psychosocial illness (40). Also, psoriasis impacts social participation (41). Health literacy has also been shown to be important for patients with psoriasis; in particular, education by healthcare professionals to achieve effective self-management has shown positive effects (42). |
|
| Acne | A smaller study found racial and ethnic minorities, as well as female gender and insurance status, to be a barrier to receiving sufficient use of systemic therapies in treatment of acne (43) And another study from China has found geographic conditions (regions: central, north, south, east, west) to be associated with acne (44). This is possibly due to differences in socioeconomic status. |
|
| Rosacea | Lower SES, psychosocial factors and lower housing quality have been found to be risk factors for developing rosacea (45). | |
| Fungal skin infections | Lower SES as well as lower parental SES have been associated with a higher risk of fungal skin infections (tinea caused by dermatophytes) (46). Tinea is linked to poor housing conditions such as overcrowding (15). |
|
| Scabies | Scabies is recognised by the WHO as a neglected tropical disease (NTD) (47). Scabies has been linked to geographical conditions such as climate, and poor hosing conditions such as overcrowding (15). A case report has associated food insecurity, immigrant status, and health literacy with scabies in infants (48), and migrants arriving by boat in the southern Mediterranean region have been observed, among other things, often to be infected with scabies (49) Smaller studies have found a geographic (in northern Australia) higher burden of scabies as well as a higher prevalence among aboriginal children compared with non-aboriginals in urban settings (50). |
|
| Cutaneous lupus erythematosus (CLE) | Race and ethnicity, as well as female gender, is associated with a higher incidence and prevalence of CLE diagnosis (51). Disease outcomes have been found to be dependent on SES, race and ethnicity, and geographic location. For example, a study found increased readmission rates for patients with lower SES, and that racially black patients had an increased length of hospital stay (52) | |
| Chronic spontaneous urticaria | Lower SES has been associated with a lower risk of chronic spontaneous urticaria (46). | |
| Leprosy | Income and race/ethnicity have been associated with the risk of leprosy (53). | |
| Pyoderma | Studies have found geographic conditions such as climate, and socioeconomic factors such as poor hygiene and low water use, as well as housing quality such as overcrowding, to be associated with pyoderma (15). | |
| A brief overview of the social determinants of health that has been reported in relation to a skin disease as identified by this study. SES: socioeconomic status. |
||
| SDOH | Diseases | ||||||||||
| Eczema/AD (14, 22, 28–33) | HS (5, 24, 37) | Cancer (5, 16, 34–36) | Psoriasis (5, 38–40, 42 | Scabies (15, 48–50) | CLE (51, 52) | Rosacea (45) | Acne (43, 44) | Tinea (15, 46) | Other (5, 15, 46, 53) | ||
| Educational access and quality | Language and literacy | ||||||||||
| Childhood development | AD | ||||||||||
| Access | AD | ||||||||||
| Attainment | AD | HS | Cancer | Psoriasis | CLE | Rosacea | Urticaria | ||||
| Social and community context | Social in-/exclusion | Psoriasis | |||||||||
| Workplace conditions | OCD | Cancer | Leukoderma | ||||||||
| Gender | HS | CLE | Acne | ||||||||
| Race and ethnicity | Eczema AD |
HS | Cancer | Scabies | CLE | Acne | Leprosy Impetigo |
||||
| Neighbourhood and built environment |
Geographic conditions | HS | Cancer | Scabies | CLE | Acne | Impetigo | ||||
| Transport | |||||||||||
| Access to healthy food and water | Scabies | ||||||||||
| Air quality | AD | ||||||||||
| Housing quality | AD | Scabies | Rosacea | Tinea | Pyoderma | ||||||
| Economic stability |
Employment | AD | HS | Cancer | Psoriasis | Leukoderma | |||||
| Food security | |||||||||||
| Housing stability | Scabies | ||||||||||
| Income | AD | HS | Cancer | Psoriasis | Scabies | CLE | Rosacea | Tinea | Leprosy Urticaria Pyoderma |
||
| Health care access and quality | Insurance | AD | HS | CLE | Acne | ||||||
| Health literacy | Eczema | Cancer | Psoriasis | ||||||||
| Access | AD | HS | Cancer | CLE | |||||||
| Results of the study presented in a matrix for easy identification of combinations of relevant social determinants of health (SDOH) and dermatoses. The illustrated categories for the SDOHs are from the healthy people 2030 infographic (54). This study employed a narrative review methodology, incorporating studies identified by their authors as addressing the social determinants of health. It presents a replicable approach that could be further refined and expanded upon by future studies, including systematic reviews or analyses conducted as research in this area becomes more structured and comprehensive. The table thus provides an overall indication of the research interests of the field on a global scale. AD: atopic dermatitis; HS: hidradenitis suppurativa; CLE: cutaneous lupus erythematosus. |
|||||||||||
The use of ICF in dermatology is not a common practice. This review identified 4 studies employing the ICF in dermatology (9–12). Three of the studies focused on patients with lymphoedema, while 1 study addressed patients with psoriasis. All studies regarded ICF as a valuable reference tool and reported intentions of creating ICF core sets in the future. To our knowledge, no ICF core sets exist for a dermatological population.
DISCUSSION
Social determinants of health in dermatology
As illustrated by this review, a wide range of SDOHs are relevant in dermatology for studies on onset and outcomes of skin diseases. The SDOH also has direct clinical importance that can be exemplified by the “RICHER” programme (Responsive Intersectoral Child and Community Health Education and Research) from 2006, which addresses disparities in healthcare access of marginalized children, youth, and families. The programme, located in Vancouver at British Columbia children’s hospital, consists of healthcare providers from 6 medical specialties who provides relational, trauma-integrated care. In 2012 dermatology was integrated into the programme due to high-frequency visits of patients with skin diseases. Reports from the programme state that skin diseases are of great importance for these socially marginalized families (13).
When working with socially marginalized families, different SDOHs can often be addressed. The relevance of these SDOHs will vary globally as they are often intrinsic to other determinants such as geographic location, healthcare system, and social system, as well as the type of skin disease in question. For instance, the impact of access to clean air and housing on scabies or atopic disease (14, 15), the impact of obesity on hidradenitis suppurativa and psoriasis (5), or the impact of access to healthcare on cancer in skin of colour (16) are all examples of situations where a skin disease in combination with an SDOH can be speculated to manifest with different significance globally.
The literature search presented in this article was systematic but did not employ the methodology of a systematic review, as this was beyond the purpose of this narrative review. The results on SDOH in dermatology in this review are thus likely scarce considering the presumed volume of studies. Nevertheless, when it proves difficult to find research on SDOH in dermatology it should serve as inspiration for researchers to be mindful of labelling their work with “SDOH” when relevant. This would assimilate the research output and facilitate the recognition of which SDOHs are important for specific skin diseases, in varying global settings. As such Table II should not be regarded as complete but provides an overview of the current research-interest identified in this review, as well as recognizing possible prioritized areas in dermatology such as occupational attainment, income, race, and ethnicity. In this aspect dermatology does not differ significantly from social medicine, where these determinants also appear with high frequency (17). Bridging the fields of dermatology and social medicine could provide a conceptualized methodological approach to research and implementation.
Social medicine and human functioning
In the efforts to bridge dermatology with social medicine a basic acquaintance with each field seems in order. The field of dermatology is presumably recognizable by the intended readers, and attention will thus be drawn to the field of social medicine.
According to the specialty description in Denmark (2) social medicine is occupied with living conditions and health, environmental medicine, psychosocial relationships, lifestyle, health, connection to the employment market, the structure of the healthcare system, patient safety, and legal regulations concerning healthcare. Social medicine traditionally utilizes both epidemiological and qualitative research methods and has a strong foundation for research in complex health interventions (2).
The core of social medicine is human functioning capacity, visualized by the ICF. It has been argued that societies, including the healthcare sector, can profit by implementing the notion of human functioning systematically (18). When an individual encounters disability, the theory integrated in functioning capacity can be used to identify possibilities of support known as rehabilitation. The WHO defines rehabilitation as “a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment” (19). Rehabilitation is a highly intersectoral effort, facilitated by social medicine, and dependent on a country’s social policy (19). Several rehabilitation programmes have, for example, been shown to reduce pain intensity for chronic diseases (20), something from which patients with skin diseases, such as individuals with hidradenitis suppurativa (HS), could benefit from. A few studies have also shown a positive effect of rehabilitation on psoriasis and chronic pruritus (21, 22).
As social medicine focuses on rehabilitation efforts aimed at reconnecting patients with the labour market, it overlaps with the field of occupational medicine. Similarly, the proposed research field of social dermatology, inspired by social medicine, intersects with the established field of occupational dermatology (23). Occupational dermatology addresses pathological skin conditions for which workplace exposure is a significant contributing factor, such as hand eczema (23). However, to our knowledge, no field within dermatology systematically addresses patients whose functional capacity and relationship with the labour market are affected by their skin disease.
International Classification of Functioning, Disability and Health (ICF)
The 4 preliminary studies found in this review report that the ICF model is relevant in dermatology and simple to use. As an unelaborated guide to the model, HS will serve as a reference disease. In the ICF context the disease, HS, would figure in the domain: “health condition”. A global survey (n = 1,299) (24) found that patients with HS can have difficulties with the domain “activities” to such an extent that 17.5% reported that HS interfered “extremely” with their ability to walk and sit down (23.0%), and with getting dressed (22.2%). 21.1% reported an extreme impact on their ability to work or study and limitations in what type of work or study they engaged in, thus impacting the domain “participation”. The symptoms of HS such as pain or fatigue are classified under the domain “body functioning and structures”. For the domain “environmental factors” it is relevant that 37.0% of the patients in the study rated it extremely difficult to gain access to a dermatologist – or that mean delay in diagnoses was 10.2 ± 8.9 years. The domain “personal factors” entails content such as educational attainment, health literacy, and coping strategies.
To illustrate the simplicity yet thorough overview that ICF provides, Fig. 2 compares 1 factor each for patients with HS and patients with skin cancer. Though overlapping concepts are present, the framework quickly summarizes how important prevention and psychological support are to skin cancer patients, whereas patients with HS could need psychical and social care. It is apparent how a systematic approach could elaborate on the different ICF categories.
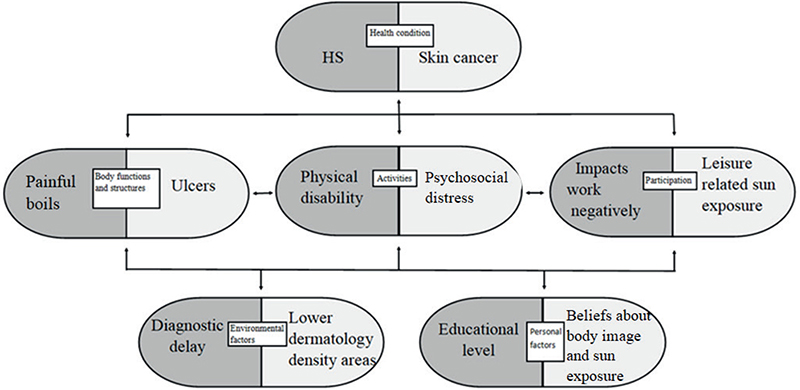
Fig. 2. ICF framework from WHO comparing 2 dermatological diseases by 1 factor. This model is grounded in a replication of the International Classification of Functioning (ICF) developed by the World Health Organization (WHO). The model comprises 5 categories that influence one another and collectively provide insights into health and disability. These categories are interconnected and dynamic in nature. The model can be applied at both the individual and populational levels. In this theoretical example, we compare populations affected by hidradenitis suppurativa (HS) and skin cancer. For each category, HS is represented on the left and skin cancer on the right. While numerous factors are relevant to each category, for the sake of simplicity, only 1 randomly selected factor per disease is illustrated in each category.
Using the ICF in a clinical setting ensures that healthcare is directly relevant to the lived experience of the patients, in line with the WHO’s call for “people-centered healthcare” (18). As systematic use of the model can be time-consuming, predefined disease-specific ICF core sets for patient populations can be of use. A few examples of diseases with formally established ICF core sets in other medical specialties includes head and neck cancer, breast cancer, obesity, depression, sleep disorders, and back pain (25).
Multiple tools have been created as “linking rules” to map collected data on functioning into ICF categories. Tools to enable a quicker approach to the ICF model also exist, such as the “Work Rehabilitation Questionnaire (WORQ)” (26), which can reflect functioning capacity in relation to workability based on generic ICF values.
In dermatology, the ICF model could be used to examine experienced biological health and consequences of disability. Functioning can be used as framework in disease management and perception, patient educational endeavours, clinical consultations, dermatological rehabilitation programmes, or in organizational planning of the care provided by medical departments. All of these are areas that have previously been highlighted as important in dermatological practice (6, 7).
Implications
In conclusion, we suggest the concept of “social dermatology”, exemplified by SDOH, human functioning, and rehabilitation, be introduced to dermatology as illustrated by Fig. 1. Academic innovative chances require organizational rearrangements within the field of dermatology. As seen in the field of social paediatrics (27), we suggest implementing a social theoretical incubator where tools, methodological guidance, implementation, and clinical examples can be shared.
The greatest obstacle moving forward with social dermatology is to establish formal agreement on the values, interests, advantages, and not least challenges for this proposed research field to ultimately go from theory to practice ensuring that the concept of skin disease moves to a bio-psychosocial approach.
ACKNOWLEDGEMENTS
EMMC is a member of the European Reference Network on Rare and Undiagnosed Skin Disorders, and member of the European Hidradenitis Suppurativa Foundation.
Data availability statement: All original data are presented in this study and included in Appendix 1. Please direct any further inquiries to the corresponding author.
REFERENCES
- Donne J. No man is an island. Meditation XVII, 1624.
- About the specialty – DASAMS [accessed 22 Nov 2024]. Available from: https://www.dasams.dk/om-dasams/om-specialet/
- Chosidow O, Chang AY. The skin of people experiencing homelessness: more (known) is less (neglected). Br J Dermatol 2003; 188: 694–695 https://doi.org/10.1093/bjd/ljad088
- Social determinants of health [accessed 22 Nov 2024], Available from: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1
- Bowers S, Chang AY. The social determinants of health and their impact on dermatologic health, part 1: the social determinants of health and their dermatologic implications. Dermatol Clin 2023; 41: 309–316. https://doi.org/10.1016/j.det.2022.10.002
- Venkatesh KP, Jothishankar B, Nambudiri VE. Incorporating social determinants of health into medical decision-making-implications for dermatology. JAMA Dermatol 2023; 159: 367–368. https://doi.org/10.1001/jamadermatol.2022.6475
- Williams J, Amerson EH, Chang AY. How dermatologists can address the structural and social determinants of health – from awareness to action. JAMA Dermatol 2022; 158: 351–352. https://doi.org/10.1001/jamadermatol.2021.5925
- International Classification of Functioning, Disability and Health (ICF). [Accessed 22 Nov 2024.] Available from: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health
- Viehoff PB, Gielink PDC, Damstra RJ, Heerkens YF, Van Ravensberg DC, Neumann MHA. Functioning in lymphedema from the patients’ perspective using the International Classification of Functioning, Disability and health (ICF) as a reference. Acta Oncol 2015; 54: 411–421. https://doi.org/10.3109/0284186X.2014.952389
- Campbell A, Hocking C, Taylor WJ. The experience of having psoriasis through the lens of the International Classification of Functioning, Disability and Health (ICF). Australas J Dermatol 2014; 55: 241–249. https://doi.org/10.1111/ajd.12103
- Viehoff PB, Hidding JT, Heerkens YF, Van Ravensberg CD, Neumann HAM. Coding of meaningful concepts in lymphedema-specific questionnaires with the ICF. Disabil Rehabil 2013; 35: 2105–2112. https://doi.org/10.3109/09638288.2013.771710
- Viehoff PB, Potijk F, Damstra RJ, Heerkens YF, Van Ravensberg CD, Van Berkel DM, et al. Identification of relevant ICF (International Classification of Functioning, Disability and Health) categories in lymphedema patients: a cross-sectional study. Acta Oncol (Madr) 2015; 54: 1218–1224. https://doi.org/10.3109/0284186X.2014.1001873
- Rehmus W, Zarbafian M, Alobaida S, Bland C, Hanson D, McIntosh G, et al. Integrating dermatology services into a social pediatrics network: 8 years of experience in the RICHER (Responsive, Interdisciplinary/Intersectoral, Child/Community, Health, Education and Research) program. Pediatr Dermatol 2021; 38: 174–178. https://doi.org/10.1111/pde.14762
- Kantor R, Silverberg JI. Environmental risk factors and their role in the management of atopic dermatitis. Expert Rev Clin Immunol 2016; 13: 15. https://doi.org/10.1080/1744666X.2016.1212660
- Andrews RM, McCarthy J, Carapetis JR, Currie BJ. Skin disorders, including pyoderma, scabies, and tinea infections. Pediatr Clin North Am 2009; 56: 1421–1440. https://doi.org/10.1016/j.pcl.2009.09.002
- Sauaia A, Dellavalle RP. Health care inequities: an introduction for dermatology providers. Dermatol Clin 2009; 27: 103–107. https://doi.org/10.1016/j.det.2008.12.001
- Department of Social Medicine [accessed 18 Feb 2025]. Available from: https://ifsv.ku.dk/om-instituttet/socialmedicin/
- Bickenbach J, Rubinelli S, Baffone C, Stucki G. The human functioning revolution: implications for health systems and sciences. Front Sci 2023; 1: 1118512. https://doi.org/10.3389/fsci.2023.1118512
- Rehabilitation [accessed 22 Nov 2024]. Available from: https://www.who.int/news-room/fact-sheets/detail/rehabilitation
- Chamberlain MA, Moser VF, Ekholm KS, O’Connor RJ, Herceg M, Ekholm J. Vocational rehabilitation: an educational review. J Rehabil Med 2009; 41: 856–869. https://doi.org/10.2340/16501977-0457
- Péter I, Jagicza A, Ajtay Z, Boncz I, Kiss I, Szendi K, et al. Balneotherapy in psoriasis rehabilitation. In Vivo 2017; 31: 1163–1168. https://doi.org/10.21873/invivo.11184
- von Martial S, Kok L, Gründel S, Augustin M, Blome C, Zeidler C, et al. Introduction of a specific dermatological rehabilitation programme for patients with chronic pruritus: a pilot study. Acta Derm Venereol 2022; 102: adv00831. https://doi.org/10.2340/actadv.v102.2930
- Fowler JF. Occupational dermatology. Curr Probl Dermatol 1998; 10: 211–244. https://doi.org/10.1016/S1040-0486(98)90000-X
- Garg A, Neuren E, Cha D, et al. Evaluating patients’ unmet needs in hidradenitis suppurativa: Results from the Global Survey of Impact and Healthcare Needs (VOICE) Project. J Am Acad Dermatol 2020; 82: 366–376. https://doi.org/10.1016/j.jaad.2019.06.1301
- Selb M, Kohler F, Robinson Nicol MM, Riberto M, Stucki G, Kennedy C, et al. ICD-11: a comprehensive picture of health, an update on the ICD-ICF joint use initiative. J Rehabil Med 2015; 47: 2–8. https://doi.org/10.2340/16501977-1928
- Finger ME, Escorpizo R, Bostan C, De Bie R. Work Rehabilitation Questionnaire (WORQ): development and preliminary psychometric evidence of an ICF-based questionnaire for vocational rehabilitation. J Occup Rehabil 2014; 24: 498–510. https://doi.org/10.1007/s10926-013-9485-2
- Singh G. ‘Rules for radicals’: a subversive’s guide to putting social paediatrics into practice. Paediatr Child Health 2022; 32: 101–109. https://doi.org/10.1016/j.paed.2021.12.005
- Apfelbacher CJ, Diepgen TL, Schmitt J. Determinants of eczema: population-based cross-sectional study in Germany. Allergy 2011; 66: 206-213.
- Croce EA, Levy ML, Adamson AS, Matsui EC. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol 2021; 148: 1104–1111. https://doi.org/10.1016/j.jaci.2021.09.015
- Ofenloch RF, Schuttelaar ML, Svensson Å, Bruze M, Naldi L, Cazzaniga S et al. Socioeconomic status and the prevalence of skin and atopic diseases in five European countries. Acta Derm Venereol 2019; 1: 99: 309–314. https://doi.org/10.2340/00015555-3082
- Nørreslet LB, Ebbehøj NE, Ellekilde Bonde JP, Thomsen SF, Agner T. The impact of atopic dermatitis on work life: a systematic review. J Eur Acad Dermatol Venereol 2018; 32: 23–38. https://doi.org/10.1111/jdv.14523
- Jamil W, Svensson Å, Josefson A, Lindberg M, von Kobyletzki LB. Incidence rate of hand eczema in different occupations: a systematic review and meta-analysis. Acta Derm Venereol 2022; 102: adv00681. https://doi.org/10.2340/actadv.v102.360
- Sedeh FB, Michaelsdóttir TE, Jemec GBE, Mortensen OS, Ibler KS. Prevalence, risk factors, and prevention of occupational contact dermatitis among professional cleaners: a systematic review. Int Arch Occup Environ Health 2023; 96: 345–354. https://doi.org/10.1007/s00420-022-01937-6
- Cortez JL, Vasquez J, Wei ML. The impact of demographics, socioeconomics, and health care access on melanoma outcomes. J Am Acad Dermatol 2021; 84: 1677–1683. https://doi.org/10.1016/j.jaad.2020.07.125
- Alcalá Ramírez del Puerto A, Hernández-Rodriguez JC, Sendín-Martín M, Ortiz-Alvarez J, Conejo-Mir Sánchez J, Pereyra-Rodriguez JJ. Skin cancer mortality in Spain: adjusted mortality rates by province and related risk factors. Int J Dermatol 2023; 62: 776–782. https://doi.org/10.1111/ijd.16618
- Schmitt J, Diepgen T, Bauer A. Occupational exposure to non-artificial UV-light and non-melanocytic skin cancer: a systematic review concerning a new occupational disease. J Dtsch Dermatol Ges 2010; 8: 250–263. https://doi.org/10.1111/j.1610-0387.2009.07260.x
- Choi ECE, Phan PHC, Oon HH. Hidradenitis suppurativa: racial and socioeconomic considerations in management. Int J Dermatol 2022; 61:1452–1457. https://doi.org/10.1111/ijd.16163
- Thomsen SF, Skov L, Dodge R, Hedegaard MS, Kjellberg J. Socioeconomic costs and health inequalities from psoriasis: a cohort study. Dermatology 2019; 235: 372–379. https://doi.org/10.1159/000499924
- Groot J, Nybo Andersen AM, Adam A, Tind Nielsen TE, Blegvad C, Skov L. Associations between maternal socioeconomic position and psoriasis: a cohort study among the offspring of the Danish National Birth Cohort. Br J Dermatol 2019; 180: 321–328. https://doi.org/10.1111/bjd.17091
- Alpsoy E, Polat M, FettahlıoGlu-Karaman B, et al. Internalized stigma in psoriasis: a multicenter study. J Dermatol 2017; 44: 885–891. https://doi.org/10.1111/1346-8138.13841
- Desthieux C, Granger B, Balanescu AR, Balint P, Braun J, Canete JD et al. Determinants of patient–physician discordance in global assessment in psoriatic arthritis: a multicenter European study. Arthritis Care Res (Hoboken) 2017; 69: 1606–1611. https://doi.org/10.1002/acr.23172
- Larsen MH, Strumse YS, Andersen MH, Borge CR, Wahl AK. Associations between disease education, self-management support, and health literacy in psoriasis. J Dermatolog Treat 2021; 32: 603–609. https://doi.org/10.1080/09546634.2019.1688233
- Barbieri JS, Shin DB, Wang S, Margolis DJ, Takeshita J. Association of race/ethnicity and sex with differences in health care use and treatment for acne. JAMA Dermatol 2022; 156: 312–319. https://doi.org/10.1001/jamadermatol.2019.4818
- Zhu L, Shen MX, Samran E, Tu YT, Chen X, Tao J, et al. Prevalence of acne in Chinese college students and its associations with social determinants and quality of life: a population-based cross-sectional study. Chin Med J (Engl) 2021; 134: 1239–1241. https://doi.org/10.1097/CM9.0000000000001292
- Chen P, Yang Z, Fan Z, Wang B, Tang Y, Xiao Y, et al. Associations of polysocial risk score with incident rosacea: a prospective cohort study of government employees in China. Front Public Health 2023; 11: 1096687. https://doi.org/10.3389/fpubh.2023.1096687
- Xiao Y, Huang X, Jing D, Huang Y, Chen L, Zhang X, et al. The prevalence of atopic dermatitis and chronic spontaneous urticaria are associated with parental socioeconomic status in adolescents in China. Acta Derm Venereol 2019; 99: 321–326. https://doi.org/10.2340/00015555-3104
- Neglected tropical diseases – GLOBAL. [Accessed 18 Jan 2025.] Available from: https://www.who.int/health-topics/neglected-tropical-diseases#tab=tab_1.
- Chang AY. On the importance of social determinants of health: a second look at scabies and failure to thrive in an immigrant female infant. Int J Womens Dermatol 2021; 7: 853. https://doi.org/10.1016/j.ijwd.2021.07.004
- Padovese V, Knapp A. Challenges of managing skin diseases in refugees and migrants. Dermatol Clin 2021; 39: 101–115. https://doi.org/10.1016/j.det.2020.08.010
- Davidson L, Knight J, Bowen AC. Skin infections in Australian Aboriginal children: a narrative review. Med J Aust 2019; 212: 231. https://doi.org/10.5694/mja2.50361
- Walker AM, Lu G, Clifton SC, Ogunsanya ME, Chong BF. Influence of socio-demographic factors in patients with cutaneous lupus erythematosus. Front Med (Lausanne) 2022; 9: 916134. https://doi.org/10.3389/fmed.2022.916134
- Himed S, Gilkey T, Trinidad J, Shipp D, Kaffenberger B, Korman AM. Impact of social determinants of health on hospital patient outcomes in cutaneous lupus erythematosus. Int J Dermatol 2023; 62: e51–e53. https://doi.org/10.1111/ijd.16029
- Simionato de Assis I, Arcoverde MAM, Ramos ACV, Alves LS, Berra TZ, Arroyo LH, et al. Social determinants, their relationship with leprosy risk and temporal trends in a tri-border region in Latin America. PLoS Negl Trop Dis 2018; 12: e0006407. https://doi.org/10.1371/journal.pntd.0006407
- Social Determinants of Health – Healthy People 2030 | odphp.health.gov. [Accessed 18 Jan 2025.] Available from: https://odphp.health.gov/healthypeople/priority-areas/social-determinants-health.
- Richard MA, Paul C, Nijsten T, Gisondi P, Salavastru C, Taieb C, et al. Prevalence of most common skin diseases in Europe: a population-based study. J Eur Acad Dermatol Venereol 2022; 36: 1088. https://doi.org/10.1111/jdv.18050