ORIGINAL REPORT
Real-world Effectiveness and Safety of Janus Kinase Inhibitors in Alopecia Areata: A Retrospective Cohort Study of 72 Patients
Sophie C. VAN HELMOND1#, Mathias WILLAERT1#, Viet-Hoa NGUYEN1, Tamar E.C. NIJSTEN1, Rick WAALBOER-SPUIJ1* and DirkJan HIJNEN1,2*
1Department of Dermatology, Erasmus MC University Medical Center, Rotterdam, and 2Department of Dermatology, Radboud University Medical Center, Nijmegen, the Netherlands
#These authors share first authorship and should be considered as first authors. *These authors share last authorship.
Alopecia areata (AA) is an autoimmune hair loss disorder characterized by sudden hair shedding due to immune dysregulation involving the Janus Kinase – Signal Transducer and Activator of Transcription (JAK-STAT) pathway. JAK inhibitors (JAKi) have demonstrated efficacy in clinical trials, but data from real-world settings remain scarce. This retrospective, single-centre cohort study evaluated the real-world effectiveness and safety of JAKi (abrocitinib, baricitinib, ritlecitinib, upadacitinib, and tofacitinib) in 72 patients treated between December 2017 and February 2024. Patients had a mean age of 34 years and a mean disease duration of 8 years. At time points 3, 6, 9, 12, and 18 months substantial regrowth was observed in 18 (25%), 28 (38.9%), 25 (34.7%), 22 (30.6%), and 19 (26.4%) patients respectively. Over a median follow-up of 16 months, 61% achieved substantial regrowth at a median time of 7 months. At 3, 6, 9, and 12 months, the cumulative regrowth rates were 11.1%, 40.2%, 55.6%, and 59.7%, respectively. Among non-responders who switched medications, 75% achieved substantial regrowth. Two serious adverse events occurred (sickle cell crisis and renal failure with pre-existing dysfunction). The findings indicate that JAKi are effective and safe for AA treatment in real-world settings. Further prospective studies are necessary to optimize treatment guidelines.
SIGNIFICANCE
Alopecia areata is an autoimmune condition causing sudden hair loss, significantly impacting quality of life. This study evaluates the effectiveness and safety of Janus kinase inhibitors in a real-world setting. Among 72 patients, 61% experienced significant hair regrowth, indicating a favourable therapeutic outcome. Our findings highlight that extended treatment durations may be necessary for optimal results, and switching between Janus kinase inhibitors proved effective for patients who did not respond to initial therapies. These results provide valuable insights on the management of alopecia areata in clinical practice, supporting the use of Janus kinase inhibitors as a treatment option for patients with severe disease.
Key words: alopecia areata; Janus kinase inhibitors; real-world evidence; safety; treatment outcome.
Citation: Acta Derm Venereol 2025; 105: adv42990. DOI: https://doi.org/10.2340/actadv.v105.42990.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 20, 2025; Accepted after revision: Mar 17, 2025. Published: Apr 7, 2025.
Corr: Rick Waalboer-Spuij, Department of Dermatology, Erasmus MC University Medical Center, Dr. Molewaterplein 40, NL-3015 GD Rotterdam, the Netherlands. E-mail: r.waalboer@erasmusmc.nl
Competing interests and funding: SvH: none; MW: none; HN: none; TN: none; DJH: investigator for AbbVie, Almirall, Galderma, LEO Pharma, Sanofi, and consultancies for AbbVie, Eli Lilly, Galderma, Pfizer, LEO Pharma; RWS: none.
No funding was received for conducting this study.
INTRODUCTION
Alopecia areata (AA) is a chronic, immune-mediated disorder with a global prevalence of 2.1% (1, 2), leading to sudden hair shedding and inhibition of hair regrowth (2). AA has been associated with a variety of autoimmune diseases (3, 4). Clinically, AA manifests as non-scarring hair loss, typically in a patchy pattern. The disease course of AA is unpredictable; approximately 50% of patients achieve spontaneous recovery within 1 year (5). In more severe cases, patchy type can evolve in total loss of scalp hair (alopecia totalis; AT), or total loss of all body hair (alopecia universalis; AU) (6). Disease severity and duration are key prognostic factors for treatment response (7). Additionally, factors such as early age of onset, ophiasis phenotype, nail involvement, comorbid atopic dermatitis, and other autoimmune diseases are associated with poorer diagnosis (8, 9). AA significantly affects quality of life, impacting self-esteem, emotions, and social interactions (10). Management of AA remains challenging; patients with severe disease (Severity of Alopecia Tool [SALT] score >50) often experience high rates of therapeutic failures and relapses. Prior to the introduction of JAK inhibitors (JAKi) for treatment of severe AA, few treatment options had been evaluated in randomized controlled trials (RCTs), which limited data on long-term efficacy and safety (11). Recent insights into AA pathogenesis implicate alopecia areata as being driven by the collapse of the immune privilege in the hair follicle, leading to attacks by T cells. Key cytokines, including interferon gamma and interleukin 15, drive immune activation and sustain an inflammatory loop via the Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway, thereby supporting the efficacy of JAKi (2, 12, 13). Several JAK inhibitors have recently been approved by the EMA and FDA for treatment of severe AA. Baricitinib (JAK 1/2 inhibitor), ritlecitinib (JAK 3/ TEC inhibitor) (14), and deuruxolitinib (JAK1/2 inhibitor) have recently been approved for severe AA treatment (15). Clinical trials apply strict inclusion criteria, yielding a homogeneous population, whereas real-world patients often present with comorbidities and concurrent medications that are excluded from trials. Recent real-world studies have begun to address the effectiveness and safety of JAKi in severe AA (16–19). However, comprehensive real-world data on JAKi treatment outcomes remain limited. This single-centre retrospective study aims to assess the real-world effectiveness and safety of JAKi for hair regrowth in AA patients treated at the Erasmus Medical Center.
MATERIALS AND METHODS
Study population
A retrospective single-centre study was conducted at the Department of Dermatology of the Erasmus University Medical Center in Rotterdam, the Netherlands. Patients with AA, including its subtypes AT, AU, and AO, who received treatment with a JAKi (abrocitinib, baricitinib, ritlecitinib, upadacitinib, or tofacitinib), most of whom also had concomitant atopic dermatitis (AD), between December 2017 and February 2024, were assessed. Local approval for data collection was obtained from the ethics committee in accordance with the ethical standards as stated in the 2013 Declaration of Helsinki.
Data collection
Demographic data and baseline clinical information were collected. Treatment response data was obtained every 3 months (window±1 month) during the first year and every 6 months (window±3 months) from the second year onwards. Treatment response was evaluated using qualitative (hair regrowth assessment “substantial regrowth”, “non-substantial regrowth”, and “no regrowth”), cumulative regrowth, and quantitative SALT outcome measures. The SALT score represents the percentage of hair loss on the scalp (7). If a SALT score was not reported during follow-up, it was calculated through photographic assessment by a panel of 2 physicians. If fewer than 3 quadrant photographic views were available, the SALT score was recorded as missing. Quantitative and qualitative analysis were combined as follows. Substantial regrowth is defined as a decrease of >20 SALT score points from baseline or in the case of missing SALT scores as a good clinical response. Non-substantial regrowth is defined as a decrease <20 SALT score points from baseline or in the case of missing SALT scores as a mild clinical response. No regrowth is defined as no decrease in SALT score points from baseline, an increase of SALT score points, or in the case of missing SALT scores as no clinical response (Table SI). Cumulative regrowth is the total number of patients who achieved substantial regrowth at any point during the study; they remain included in the cumulative regrowth group (regardless of whether they maintain the effect, are lost to follow-up, or experience relapse later). This is different from substantial regrowth percentages reported at specific time points, which indicate the proportion of patients actively exhibiting the effect at that moment. Safety treatment outcomes were reported (adverse events, reasons for discontinuation). Preliminary data were obtained if patients discontinued treatment before the 2-month mark. If a patient switched JAKi, the data on the first was enrolled in the general analysis and the second described.
Statistical analysis
Data analysis was performed in SPSS, version 29.0.0.0 (IBM Corp, Armonk, NY, USA). Categorical data were reported as number of cases and proportions. Numerical variables were assessed for normality of variable distributions using the Shapiro–Wilk test. Normally distributed variables were reported as mean (standard deviation), while non-normally distributed variables were reported as median (interquartile range). Kaplan–Meier survival analysis was performed for time to events: substantial regrowth, SALT≤20. Patients with no event at the end of follow up were censored.
RESULTS
A total of 75 patients with AA were treated with a JAKi at the Department of Dermatology at the Erasmus University Medical Center in Rotterdam. Three patients were excluded due to inactive AA at the start of the treatment as their primary indication for treatment was AD. A total of 72 patients were included in the final analysis.
Patient characteristics
The cohort consisted predominantly of females (n = 52, 72.2%). The mean ± standard deviation age at start of treatment was 34 ±15 years, range 6–69. A history of atopy was reported in 59 patients (81.9%), with active AD in 38 (52.8%). A family history of AA was noted in 19 patients (32.8%). (Table I, Table SII). The median age of onset was 23 years (IQR 21) and ranged from 4 to 54 years. The mean ± SD duration of disease was 8.6 ± 8.0 years, range 0.25–32 years), with a median baseline SALT score of 100 (IQR 9, range 15–100). Of the 50 patients, 39 (54.2%) were classified as AU, involving eyebrows and eyelashes, and 11 (15.3%) as AT. Additionally, 11 patients (15.3%) had patchy AA, and 1 had AA ophiasis type (Table II). Of the 72 patients, 8 (11.1%) received abrocitinib, 27 (37.5%) baricitinib, 6 (8.3%) ritlecitinib, 15 (20.8%) upadacitinib, and 16 (22.2%) tofacitinib as their first used JAKi. Abrocitinib was dosed at 50–200 mg/day. Baricitinib was started at a dose of 2–4 mg/day and was up titrated to 4 mg/day. Ritlecitinib was dosed at 50 mg/day. Upadacitinib was dosed at 15–30 mg/day. Tofacitinib was dosed at 5–10 mg/day. The mean ±SD follow-up period was 15.7 ± 14.7 months) (Table II).
Treatment characteristics
The number of patients present at the 3, 6, 9, 12, and 18-month follow-up points was 61 (84.7%), 44 (61.1%), 39 (54.2%), 26 (36.1%), and 22 (30.6%), respectively. The number of missing patients at each time point was 11, 28, 33, 46, and 50. At 3, 6, 9, 12, and 18 months, substantial regrowth was observed in 18 (25%), 28 (38.9%), 25 (34.7%), 22 (30.6%), and 19 (26.4%) patients, while non-substantial regrowth occurred in 28 (38.9%), 10 (13.9%), 13 (18.1%), 1 (1.4%), and 1 (1.4%) patients, respectively. No response was observed in 15 (20.8%), 6 (8.3%), 1 (1.4%), 3 (4.2%), and 2 (2.8%) patients at these time points (Fig. 1, Table SIII).
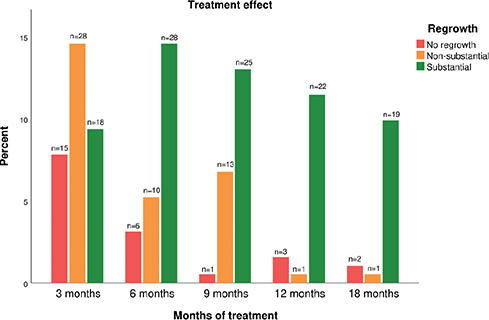
Fig. 1. Treatment outcome per follow-up moment.
Kaplan–Meier curves were plotted for time to substantial regrowth. In the total cohort of 72 patients, 44 (61%) achieved substantial regrowth: 4/8 (50%) on abrocitinib, 15/27 (56%) on baricitinib, 3/6 (50%) on ritlecitinib, 9/15 (60%) on upadacitinib, and 13/16 (81%) on tofacitinib (Table SIII). The median time to substantial regrowth was 7 months (Fig. 2). At 3, 6, 9, and 12 months, cumulative regrowth was observed in 8, 29, 40, and 43 patients, respectively.
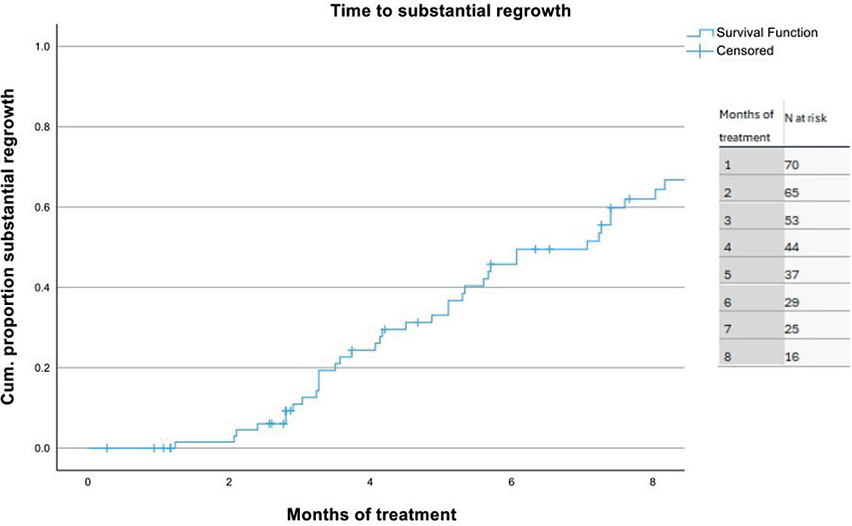
Fig. 2. Time to substantial regrowth for all Janus kinase inhibitors.
The median SALT scores at baseline, 3, 6, 9, and 12 months were 100 (IQR 10, n = 62), 95 (IQR 69, n = 52), 20 (IQR 83, n = 32), 3 (IQR 86, n = 25), and 0 (IQR 23, n = 21), respectively. SALT scores were frequently missing during follow up (Fig. 3). Kaplan–Meier curves were plotted for time to SALT ≤20. In the total cohort of 72 patients, 36 (50%) achieved an absolute SALT score ≤20 with the first JAKi: 3/8 (38%) on abrocitinib, 12/27 (44%) patients on baricitinib, 3/6 (50%) on ritlecitinib, 7/15 (47%) on upadacitinib, and 11/16 (67%) on tofacitinib. At 3, 6, 9, and 12 months, the cumulative number of patients who have achieved a SALT ≤20 was 4, 19, 29, and 32 respectively. The median time to SALT ≤20 was 8.5 months. At the 9-month cut off on the Kaplan–Meier curve, there were 18 patients (25%) left in the follow up who had not achieved SALT ≤20 (i.e., N at risk) (Fig. 4).

Fig. 3. Severity of Alopecia Tool (SALT) scores per follow-up.
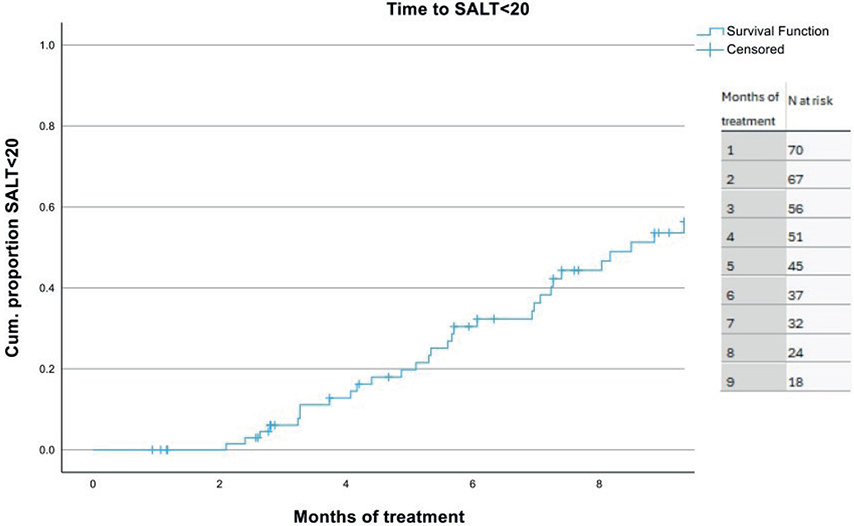
Fig. 4. Time to Severity of Alopecia Tool (SALT) <20 summarized for all Janus kinase inhibitors.
Eighteen patients maintained substantial regrowth after 12 months, and 12 maintained this effect after 24 months. Of the 43 patients who achieved substantial regrowth, 4 (9.3%) encountered loss of response (Fig. S1).
Reasons for discontinuation or switch of JAK inhibitor
Thirty-one patients discontinued treatment or switched to a different JAKi. The most common reason for discontinuation or switching was insufficient effect on comorbid AD in 13 patients (31.0%), followed by insufficient hair growth in 11 patients (26.2%), adverse events in 4 patients (9.5%), and lab abnormalities in 4 patients (9.5%). Among the 18 patients who switched to a different JAKi at least once during the observational period, 1 patient switched within the first month due to an AD exacerbation. Of the 4 patients with no regrowth on the first JAKi, 1 (25%) achieved substantial regrowth within 6 months on the second JAKi, and 1 (25%) after 2 years; 2(50%) did not achieve substantial regrowth. All 4 patients who switched due to non-substantial regrowth on the first JAKi achieved substantial regrowth on the second JAKi. From these responding patients, 1 (25%) lost response to treatment after 2 years. Five patients who initially had substantial regrowth but switched due to insufficient effect on their AD also achieved substantial regrowth on the second JAKi (Table SIV, Fig. S1).
Adverse events
Gastrointestinal symptoms were reported by 18 patients (25%), and 15 patients (20.8%) experienced acne. Rash or itching occurred in 9 patients (12.5%). Mild infections (e.g., upper respiratory tract infections) were reported by 22 patients (30.6%). Eight patients (11.1%) experienced an infection requiring treatment, including respiratory, urinary, and gastrointestinal infections, as well as herpes zoster and herpes simplex. Two patients were hospitalized: 1 for a sickle cell crisis and another for renal failure due to pre-existing kidney issues (Table SV).
DISCUSSION
This study aimed to assess the real-world effectiveness of JAKi in the treatment of AA, particularly among patients with severe disease (SALT >50), including 69.4% of patients with AT, a mean disease duration of 8 years, and 16-month median follow-up. In this cohort, 61% of patients achieved substantial hair regrowth with their initial JAKi regrowth at 7 months median. At 3, 6, 9, 12, and 18 months’ follow-up substantial regrowth was observed in 18 (25%), 28 (38.9%), 25 (34.7%), 22 (30.6%), and 19 (26.4%) patients, respectively. At 3, 6, 9, and 12 months, the cumulative number of patients who achieved regrowth was 11.1%, 40.2%, 55.6%, and 59.7%, respectively. Additionally, 50% of patients attained an absolute SALT ≤20, a benchmark indicating significant improvement. Sustained substantial regrowth was observed in 18 patients at 12 months, with 12 maintaining their response at 24 months. However, 9.3% of patients experienced therapeutic loss during follow-up. This retrospective analysis provides valuable insights into the long-term efficacy of JAKi in the treatment of AA within a real-world setting, further enriching the evidence base and underscoring their potential as effective therapeutic options for this challenging condition.
The efficacy of JAKi, including ritlecitinib and baricitinib for treatment of severe AA, has been well demonstrated in phase 3 clinical trials (20, 21). Ritlecitinib achieved SALT ≤20 in 17–28% of patients after 24 weeks, increasing to 25–50% at 48 weeks, with 44–80% reporting “moderate” or “great” improvement (20). Baricitinib showed SALT ≤20 achievement in 32.5–35.2% of patients at 6 months, and 36.8–40.9% at 12 months (21). In comparison, our study observed higher rates of SALT ≤20 achievement, likely due to differences in follow-up duration and inclusion of patients treated for comorbid AD, which allowed for variable treatment periods. Additionally, the inclusion of patients with more heterogeneous baseline severity and comorbid conditions, which is characteristic of real-world clinical practice, may contribute to this variation. Tofacitinib showed a 50% improvement in SALT scores in 32% of patients in early trials (22), and 55.9% achieving a 50% SALT reduction after 18 months in a retrospective study (17, 18). In our cohort, substantial regrowth was achieved in 81.3% of patients, possibly reflecting differences in baseline characteristics, population heterogeneity, and follow-up duration. Previous studies with upadacitinib demonstrated a median SALT score reduction after 24 weeks of treatment from SALT 50 to 5, which is consistent with 60% of patients experiencing substantial regrowth in the current cohort (19). The use of abrocitinib in patients with AA has been reported only in case studies (23–27). We found that 50% of patients treated with abrocitinib achieved substantial regrowth, suggesting its potential utility as a therapeutic option for AA. These findings suggest that all JAKi studied showed effectiveness for treatment of AA despite their differences in target enzyme specificity (28, 29). IFN-gamma and IL-15 signalling through JAK1, JAK2, and JAK3 are thought to be the key drivers of the disease. The ability of JAKi to target these pathways likely accounts for their broad therapeutic efficacy (28, 30, 31). Alternative mechanisms, such as beta-catenin activation and DKK1 suppression, may also enhance follicular regrowth, warranting further investigation (32). In line with studies on long-term use of baricitinib, this study confirms the progressive improvement in response rates with prolonged treatment. Baricitinib demonstrated significant long-term efficacy, with 33.7% of patients achieving a SALT ≤20 and 48.5% achieving a SALT ≤30 after 52 weeks of continuous treatment, confirming the importance of extended therapy duration in managing severe AA (33). Similarly, in our cohort, the median time to substantial regrowth was 7 months, with a median time to achieve SALT ≤20 of 8.5 months. Cumulative regrowth was observed in 40 patients by 9 months, and 43 by 12 months. These findings emphasize that significant improvement can continue beyond the standard 6-month evaluation period required by insurance policies in the Netherlands. While treatment must be assessed at 6 months, there is no strict requirement to discontinue based on a specific response threshold, allowing for ongoing therapy when clinically indicated and recognizing the potential for further improvement with prolonged treatment (34). The importance of long-term evaluation is further supported by the observation that switching JAKi may provide additional benefit in cases of suboptimal response. Some patients with non-substantial hair regrowth at 18 months continued JAKi therapy, likely due to its effectiveness in managing coexisting AD. In this study, patients who switched to a different JAKi after insufficient response often achieved substantial regrowth. This aligns with the growing evidence suggesting that failure with 1 JAKi does not predict failure with another, emphasizing the need for individualized and adaptive therapeutic approaches to optimize outcomes in AA (35).
The most frequently observed adverse events (AE) in this study were upper respiratory tract infections, gastrointestinal symptoms, and acne, consistent with the BRAVE-AA1, BRAVE-AA2, and ALLEGRO trials (21, 33, 36). Two serious AE occurred, a sickle cell crisis and renal failure in a patient with pre-existing renal dysfunction and sickle cell disease, highlighting the need for dose adjustments in moderate-to-severe renal impairment (37). Treatment discontinuation or switching of JAKi was primarily due to insufficient efficacy for AD, or hair regrowth, followed by adverse events, and laboratory abnormalities (21). These findings emphasize the importance of close monitoring, particularly in patients with comorbidities, to optimize safety and efficacy in JAKi therapy.
This study highlights the real-world effectiveness and safety of JAKi in treating severe AA. Substantial hair regrowth was achieved in 61% of patients with their initial JAKi, and 50% attained a SALT ≤20. Extended treatment durations were often required to achieve optimal outcomes, with responses continuing to improve beyond 12 months in some cases. Importantly, this study demonstrates that, in addition to the currently registered JAKi baricitinib and ritlecitinib, other JAKi, including abrocitinib, tofacitinib, and upadacitinib, can be effective for treating AA. This broadens the therapeutic landscape for AA patients with comorbid AD, particularly for patients demonstrating inadequate response to JAKi registered for AA. Adverse events were predominantly mild to moderate and consistent with those reported in clinical trials. Despite limitations inherent in its retrospective design, such as missing data and variability in documentation, this study provides valuable insights into the practical application of JAKi. Future prospective research is needed to optimize long-term management, identify prognostic factors, and evaluate the impact of these treatments on patient quality of life.
ACKNOWLEDGEMENTS
IRB approval status: This study was approved by the Institutional Review Board (IRB), the Medical Scientific Research Ethical Committee of the Erasmus University Medical Center, reference number MEC-2024-0173.
REFERENCES
- Lee HH, Gwillim E, Patel KR, Hua T, Rastogi S, Ibler E, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: a systematic review and meta-analysis. J Am Acad Dermatol 2020; 82: 675–682. https://doi.org/10.1016/j.jaad.2019.08.032
- Olayinka JJT, Richmond JM. Immunopathogenesis of alopecia areata. Curr Res Immunol 2021; 2: 7–11. https://doi.org/10.1016/j.crimmu.2021.02.001
- Barahmani N, Schabath MB, Duvic M, National Alopecia Areata R. History of atopy or autoimmunity increases risk of alopecia areata. J Am Acad Dermatol 2009; 61: 581–591. https://doi.org/10.1016/j.jaad.2009.04.031
- Chu SY, Chen YJ, Tseng WC, Lin MW, Chen TJ, Hwang CY, et al. Comorbidity profiles among patients with alopecia areata: the importance of onset age, a nationwide population-based study. J Am Acad Dermatol 2011; 65: 949–956. https://doi.org/10.1016/j.jaad.2010.08.032
- Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update: part I. Clinical picture, histopathology, and pathogenesis. J Am Acad Dermatol 2010; 62: 177–188, quiz 189–190. https://doi.org/10.1016/j.jaad.2009.10.032
- Cranwell WC, Lai VWY, Photiou L, Meah N, Wall D, Rathnayake D, et al. Treatment of alopecia areata: an Australian expert consensus statement. Australas J Dermatol 2019; 60: 163–170. https://doi.org/10.1111/ajd.12941
- Olsen EA, Hordinsky MK, Price VH, Roberts JL, Shapiro J, Canfield D, et al. Alopecia areata investigational assessment guidelines – Part II. National Alopecia Areata Foundation. J Am Acad Dermatol 2004; 51: 440–447. https://doi.org/10.1016/j.jaad.2003.09.032
- Lee S, Lee WS. Management of alopecia areata: updates and algorithmic approach. J Dermatol 2017; 44: 1199–1211. https://doi.org/10.1111/1346-8138.13933
- Meah N, Wall D, York K, Bhoyrul B, Bokhari L, Asz-Sigall D, et al. The Alopecia Areata Consensus of Experts (ACE) study part II: Results of an international expert opinion on diagnosis and laboratory evaluation for alopecia areata. J Am Acad Dermatol 2021; 84: 1594–1601. https://doi.org/10.1016/j.jaad.2020.09.028
- Mostaghimi A, Napatalung L, Sikirica V, Winnette R, Xenakis J, Zwillich SH, et al. Patient perspectives of the social, emotional and functional impact of alopecia areata: a systematic literature review. Dermatol Ther (Heidelb) 2021; 11: 867–883. https://doi.org/10.1007/s13555-021-00512-0
- Mateos-Haro M, Novoa-Candia M, Sanchez Vanegas G, Correa-Perez A, Gaetano Gil A, Fernandez-Garcia S, et al. Treatments for alopecia areata: a network meta-analysis. Cochrane Database Syst Rev 2023; 10: CD013719. https://doi.org/10.1002/14651858.CD013719.pub2
- Gilhar A, Laufer-Britva R, Keren A, Paus R. Frontiers in alopecia areata pathobiology research. J Allergy Clin Immunol 2019; 144: 1478–1489. https://doi.org/10.1016/j.jaci.2019.08.035
- Zhou C, Li X, Wang C, Zhang J. Alopecia areata: an update on etiopathogenesis, diagnosis, and management. Clin Rev Allergy Immunol 2021; 61: 403–423. https://doi.org/10.1007/s12016-021-08883-0
- Rudnicka L, Arenbergerova M, Grimalt R, Ioannides D, Katoulis AC, Lazaridou E, et al. European expert consensus statement on the systemic treatment of alopecia areata. J Eur Acad Dermatol Venereol 2024; 38: 687–694. https://doi.org/10.1111/jdv.19768
- Ltd. SPI. U.S. FDA approves LEQSELVI™ (deuruxolitinib), an oral JAK inhibitor for the treatment of severe alopecia areata. 2024. https://sunpharma.com/wp-content/uploads/2024/07/Sunpharma-LEQSELVI-Approval-Scenario-Press-Release.pdf
- Vignoli CA, Gargiulo L, Ibba L, Balato A, Barbareschi M, Barruscotti S, et al. Baricitinib for the treatment of severe alopecia areata: results from a 52-week multicenter retrospective real-world study. J Dermatolog Treat 2025; 36: 2444494. https://doi.org/10.1080/09546634.2024.2444494
- Cranwell W, Meah N, Wall D, Bevin B, Laita B, Sinclair RD. Real-world effectiveness and safety of tofacitinib for alopecia areata: a retrospective cohort study of 202 patients. Australas J Dermatol 2024; 65: 505–513. https://doi.org/10.1111/ajd.14325
- Huang J, Qian P, Tang Y, Li J, Liu F, Shi W. Effectiveness and predictive factors of response to tofacitinib therapy in 125 patients with alopecia areata: a single-centre real-world retrospective study. Acta Derm Venereol 2023; 103: adv12425. https://doi.org/10.2340/actadv.v103.12425
- Flora A, Kozera E, Frew JW. Treatment of alopecia areata with the Janus kinase inhibitor upadacitinib: a retrospective cohort study. J Am Acad Dermatol 2023; 89: 137–138. https://doi.org/10.1016/j.jaad.2022.12.056
- Hordinsky M, Hebert AA, Gooderham M, Kwon O, Murashkin N, Fang H, et al. Efficacy and safety of ritlecitinib in adolescents with alopecia areata: results from the ALLEGRO phase 2b/3 randomized, double–blind, placebo-controlled trial. Pediatr Dermatol 2023; 40: 1003–1009. https://doi.org/10.1111/pde.15378
- Kwon O, Senna MM, Sinclair R, Ito T, Dutronc Y, Lin CY, et al. Efficacy and safety of baricitinib in patients with severe alopecia areata over 52 weeks of continuous therapy in two phase III trials (BRAVE-AA1 and BRAVE-AA2). Am J Clin Dermatol 2023; 24: 443–451. https://doi.org/10.1007/s40257-023-00764-w
- Kennedy Crispin M, Ko JM, Craiglow BG, Li S, Shankar G, Urban JR, et al. Safety and efficacy of the JAK inhibitor tofacitinib citrate in patients with alopecia areata. JCI Insight 2016; 1: e89776. https://doi.org/10.1172/jci.insight.89776
- Liu X, Song B, Jin H. Abrocitinib improved dupilumab-resistant severe atopic dermatitis with comorbid mild alopecia areata in a 12-year-old boy: a case report with 1-year follow-up. J Asthma Allergy 2024; 17: 305–311. https://doi.org/10.2147/JAA.S458684
- Zhang J, Zuo YG. Successful treatment of alopecia universalis with abrocitinib: a case report. J Dermatolog Treat 2023; 34: 2242706. https://doi.org/10.1080/09546634.2023.2242706
- Bennett M, Moussa A, Sinclair R. Successful treatment of chronic severe alopecia areata with abrocitinib. Australas J Dermatol 2022; 63: 274–276. https://doi.org/10.1111/ajd.13836
- Huang J, Liu O. Effective treatment of refractory alopecia areata in pediatric patients with oral abrocitinib. J Cosmet Dermatol 2024; 23: 348–349. https://doi.org/10.1111/jocd.15896
- Zhao J, Liu L. A case of atopic dermatitis with alopecia universalis in a patient treated with abrocitinib. JAAD Case Rep 2022; 22: 99–100. https://doi.org/10.1016/j.jdcr.2022.02.027
- Lensing M, Jabbari A. An overview of JAK/STAT pathways and JAK inhibition in alopecia areata. Front Immunol 2022; 13: 955035. https://doi.org/10.3389/fimmu.2022.955035
- Mattsson J, Israelsson E, Bjorhall K, Yrlid LF, Thorn K, Thoren A, et al. Selective Janus kinase 1 inhibition resolves inflammation and restores hair growth offering a viable treatment option for alopecia areata. Skin Health Dis 2023; 3: e209. https://doi.org/10.1002/ski2.209
- Zhang X, Zhao Y, Ye Y, Li S, Qi S, Yang Y, et al. Lesional infiltration of mast cells, Langerhans cells, T cells and local cytokine profiles in alopecia areata. Arch Dermatol Res 2015; 307: 319–331. https://doi.org/10.1007/s00403-015-1539-1
- Kasumagic-Halilovic E, Cavaljuga S, Ovcina-Kurtovic N, Zecevic L. Serum levels of interleukin-2 in patients with alopecia areata: relationship with clinical type and duration of the disease. Skin Appendage Disord 2018; 4: 286–290. https://doi.org/10.1159/000486462
- Shin JM, Sung Y, Hong D, Jung KE, Seo YJ, Kim CD, et al. Differences in activation of beta-catenin in outer root sheath cells between the type of JAK inhibitor: an alternative mechanism promoting hair growth by JAK inhibitors in alopecia areata. J Dermatol Sci 2024; 114: 148–150. https://doi.org/10.1016/j.jdermsci.2024.04.005
- Senna M, Mostaghimi A, Ohyama M, Sinclair R, Dutronc Y, Wu WS, et al. Long-term efficacy and safety of baricitinib in patients with severe alopecia areata: 104-week results from BRAVE-AA1 and BRAVE-AA2. J Eur Acad Dermatol Venereol 2024; 38: 583–593. https://doi.org/10.1111/jdv.19665
- Dutch Health Institute (Nederland ZI, GVS). Recommendation on baricitinib (Olumiant) for severe alopecia areata. https://www.zorginstituutnederland.nl/publicaties/adviezen/2024/07/31/gvs-advies-baricitinib-olumiant-bij-ernstige-alopecia-areata
- Peterson D, Powell M, King B. Less is more? Failure of one JAK inhibitor does not predict failure of another one in a patient with alopecia areata. Dermatol Ther 2021; 34: e15062. https://doi.org/10.1111/dth.15062
- King B, Soung J, Tziotzios C, Rudnicka L, Joly P, Gooderham M, et al. Correction to: Integrated safety analysis of ritlecitinib, an oral JAK3/TEC family kinase inhibitor, for the treatment of alopecia areata from the ALLEGRO Clinical Trial Program. Am J Clin Dermatol 2024; 25: 689. https://doi.org/10.1007/s40257-024-00864-1
- Nakayama Y, Onishi A, Yamamoto W, Yoshikawa A, Shiba H, Yoshida N, et al. Safety of Janus kinase inhibitors compared to biological DMARDs in patients with rheumatoid arthritis and renal impairment: the ANSWER cohort study. Clin Exp Med 2024; 24: 97. https://doi.org/10.1007/s10238-024-01360-w