ORIGINAL REPORT
Long-term Progressive Improvement of Atopic Dermatitis by an Herbal Emollient Plus Combination in a 12-week Clinical Trial
Lars HERRMANN1# , Stanislav ANDREEV1#, Ramona ZIEGLER1, Christine NEUBAUER1, Kathrin MORITZ1, Nicole MAEHLER1, Hubert STEINDL1, Stephan DAEHNHARDT-PFEIFFER2 and Christoph ABELS1
, Stanislav ANDREEV1#, Ramona ZIEGLER1, Christine NEUBAUER1, Kathrin MORITZ1, Nicole MAEHLER1, Hubert STEINDL1, Stephan DAEHNHARDT-PFEIFFER2 and Christoph ABELS1
1Bionorica SE, Neumarkt, and 2Microscopy Services Dähnhardt GmbH, Flintbek, Germany
#Authors contributed equally to this work and share first authorship.
Atopic dermatitis is a chronic inflammatory skin disease characterized by flare-ups of inflamed, dry, and itchy skin affecting over 200 million people worldwide. “Emollients plus” containing active cosmetic ingredients such as herbal extracts and phytochemicals have the potential to surpass the efficacy of conventional emollients, while avoiding side effects associated with pharmacological interventions. The reported 12-week clinical trial (NCT05790083) evaluated long-term efficacy and tolerability of oil-in-water emulsions BNO 3731 and BNO 3732 containing ginger extract and cannabidiol as basic emollient therapy for atopic dermatitis. A total of 100 adults and children with a history of atopic dermatitis were included and applied BNO 3732 (body lotion) twice daily and BNO 3731 (intensive care product) as needed. Over 12 weeks the emollients plus combination led to sustained improvement of peak pruritus and patient-reported outcome measures, i.e., “Recap of atopic eczema”. Objective dermatological evaluation showed progressive improvements for vIGA-ADTM and isolated symptoms, i.e., erythema and dryness. Instrumental analysis of intercellular lipid contents and lipid lamellae organization in the stratum corneum demonstrated recovery of the epidermal barrier integrity. The clinical results provide evidence on the efficacy of herbal emollients plus beyond mere moisturizing and occlusive properties. BNO 3731 and BNO 3732 were very well tolerated.
SIGNIFICANCE
Basic emollient treatment is a cornerstone in the long-term management of atopic dermatitis. In recent years, emollients plus with active cosmetic ingredients have emerged as effective treatment options beyond simple moisturizers and occlusives. To evaluate the efficacy of novel (cosmetic) emollients, high-quality clinical trials are essential. Therefore, a new combination of emollients (oil-in-water emulsions) containing ginger extract and cannabidiol was tested over 12 weeks in patients with atopic dermatitis. The products provided sustained itch relief, progressive improvement of visible symptoms, and substantial recovery of the skin barrier. Herbal emollients plus are able to improve basic emollient therapy beyond conventional emollients.
Key words: atopic dermatitis; basic emollient therapy; clinical trial; emollient plus; herbal ingredients; phytochemicals.
Citation: Acta Derm Venereol 2025; 105: adv43026. DOI: https://doi.org/10.2340/actadv.v105.43026.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 24, 2025. Accepted after revision: May 20, 2025. Published: Jun 18, 2025.
Corr: Christoph Abels, Bionorica SE, Kerschensteinerstraße 11–15, 92318 Neumarkt, Germany. E-mail: Christoph.Abels@bionorica.de
Competing interests and funding: LH, SA, RZ, CN, KM, NM, HS, and CA are/were employed by Bionorica SE (Neumarkt in der Oberpfalz, Germany). CA is named as inventor on a patent application for compositions containing cannabidiol and an extract from ginger (WO 2023/046730). All authors received medical writing support from co.medical (Berlin, Germany).
This trial was funded by Bionorica SE (Neumarkt in der Oberpfalz, Germany).
INTRODUCTION
A topic dermatitis (AD) is a chronic inflammatory skin disease characterized by flares of inflamed, dry, and itchy skin. The worldwide prevalence is increasing, with over 200 million people affected (1). As no cure for AD is available, the treatment goal is symptomatic management using pharmacological and non-pharmacological interventions (2). Patients suffering from AD often have a reduced quality of life, with one of the most burdensome symptoms being itch (3). Therefore, the control of itch should be the central focus of treatment and a primary therapeutic goal (4).
A key feature of the pathophysiology underlying the appearance and eczematous lesions of AD skin is a compromised skin barrier integrity, which contributes to the development of itch and is manifested by distinct physiological changes (4, 5). For instance, the amounts of certain epidermal lipids (e.g., ceramides EOS, NP and AP, cholesterol, and free fatty acids) are reduced (6). Besides, a disrupted lipid organization represented by a shortened length of lipid lamellae and enlarged areas with no or significantly reduced occurrence of lipid lamellae in the intercellular space of the stratum corneum (SC) can be observed (7–10). A reduced ratio of mature to unmature corneocytes in the SC of AD patients due to a disturbed differentiation has been reported as well (7, 11).
Basic therapy with emollients remains the cornerstone of AD treatment (12, 13), as recommended by the European guideline as well as by the 2022 consensus report by the European Federation of Allergy and Airways Diseases Patients’ Associations (EFA) (13, 14). Despite their significance, the therapeutic efficacy of conventional emollients is limited. Primarily containing moisturizing and/or occlusive agents, they effectively increase epidermal hydration and reduce transepidermal water loss; however, do not specifically target the mechanisms underlying skin irritation and barrier dysfunction, which in turn are associated with itch perception (4).
A recent strategy to improve basic emollient therapy is the formulation of emollients with active, non-medicated substances (active cosmetic ingredients, ACIs), resulting in so-called “emollients plus”, which have been recognized by the European Guideline on Atopic Eczema (12, 13). These next-generation topicals aim to complement the mere occlusive and moisturizing properties of conventional emollients by specifically addressing bothersome symptoms such as erythema or itch and thereby reduce the need for pharmacological interventions with topical corticosteroids (TCS) or calcineurin inhibitors (TCI).
Herbal ingredients have a great potential as ACIs and, accordingly, herbal emollients plus have been suggested to exceed the effects of mere emollients (10, 15, 16). A previous publication reported synergistic anti-inflammatory and anti-oxidative properties of a ginger extract and cannabidiol (CBD) in vitro and proposed a putative mode of action of these ACIs. For instance, ginger extract and CBD reduced TNF-α-induced NF-κB activation in an epidermal cell line (HaCaT) as well as the release of inflammatory cytokines including TNF-α, IL-6, and IL-8 from primary keratinocytes (NHEK), and decreased LPS-induced NO release in macrophages (17). The oil-in-water emulsion BNO 3731, containing a combination of ginger extract and CBD, showed fast and significant improvement of visible AD symptoms such as erythema, dryness, scaling ,and papules as well as rapid reduction of peak pruritus along with very good tolerability in a 5-day clinical trial including an emollient plus comparator product (17).
The prospective interventional clinical trial reported here assessed the efficacy and tolerability of an emollient plus combination comprising both the intensive care product BNO 3731 and corresponding body lotion BNO 3732 in adults and children suffering from AD over 12 weeks. In addition to objective dermatological assessments, evaluation of itch intensity, and patient-reported outcome measures (PROMs), a focus was set on the investigation of the barrier integrity in a subgroup of adults, by assessing epidermal lipid content, lipid lamellae organization, and corneocyte maturity.
MATERIALS AND METHODS
Investigational cosmetic products
Bionorica® Derma Line “Lotion” (BNO 3732) (body lotion) and “Atopi Intensivpflege” (BNO 3731) (intensive care) are non-occlusive oil-in-water emulsions containing the ACIs ginger (lipophilic CO2 extract) and CBD (synthetic) (for details see Appendix S1). The products were blinded with black tape and the subjects were not informed about the quality of the products.
Clinical trial design
Long-term efficacy of the product combination was assessed via a prospective, interventional, monocentric trial. To assure complete epidermal turnover and demonstrate progressive long-term effects, a trial duration of 12 weeks was purposely selected, as the approximate physiological turnover of the SC is around 28 days (Fig. 1) (18). A remote real-world data (RWD) study was implemented as a concurrent external control for selected patient-reported outcomes as well as for the occurrence of flare-ups and related corticosteroid use (19). The prospective study collected and analysed RWD on disease burden and emollient use in 304 adults and children with AD, aiming to assess the real-world effectiveness of basic emollient therapy in AD and was carried out in parallel (01/2023-04/2023) with the reported trial (for details see Appendix S1).
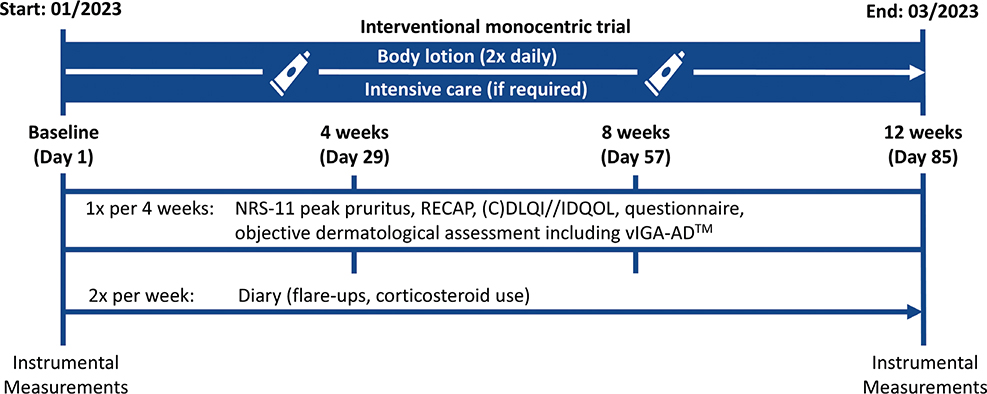
Fig. 1. Trial design of the 12-week monocentric trial.
Participant selection
A population of n = 100 patients with atopic dermatitis was enrolled with n = 94 patients analysed (5 subjects dropped out without and 1 subject dropped out with relation to test product(s)). The patients (21 male [22%], 73 female [78%]) had a history of AD with at least 2 flare-ups in the previous winter season but did not necessarily present with acute lesions at inclusion. Patients with current systemic AD therapies or regular, proactive use of TCS/TCI were excluded; therefore the population can be defined as having “mild atopic dermatitis” in accordance with the stepped-care plan of the European Guideline on Atopic Eczema (13). The population included children/adolescents (≥ 2–17 years, mean age ± SD: 8.9 ± 3.8 years) and adults (≥ 18 years, mean age ± SD: 43.6 ± 15.3 years) in a ratio of roughly 1:1 with a mean age of 27.7 ± 20.8 years (mean ± SD). Complete inclusion and exclusion criteria are provided in Appendix S1.
Treatment schedule
Patients were advised to use the body lotion twice daily (morning and evening) as needed on the whole body including the face, but at least on arms, legs, abdomen, and lower back, according to normal use conditions. Patients were instructed to use the intensive care product as required on affected body areas in addition to the body lotion.
Clinical assessment
Subjective clinical assessment followed the recommendations by the Harmonising Outcome Measures for Eczema (HOME) initiative including the validated PROMs “Recap of atopic eczema” (RECAP) (20) and (Children’s) Dermatology Quality of Life Index (CDLQI, age 4–15 years/DLQI, age ≥ 16 years)/Infants’ Dermatitis Quality of Life Index (IDQOL, age < 4 years) (21–23). Itch was evaluated by the PRO tool peak pruritus numerical rating scale (NRS-11) (24, 25). The occurrence of flare-ups and flare-up-related TCS use was documented in twice-weekly online diary reports. Visible skin alterations were assessed by experienced dermatologists as individual objective symptoms on a proprietary scale and globally via the validated Investigator Global Assessment Scale for Atopic Dermatitis (vIGA-ADTM) (26). To evaluate the epidermal barrier integrity, lipid composition and organization within the interstitial space in the SC were analysed via non-invasive Lipbarvis® sampling (7, 8) (Fig. S1). The samples were subsequently evaluated via transmission electron microscopy (TEM) based methods for mapping and visualization of the lipid lamellae. The contents of intercellular lipids (ceramides (EOS, NP, and AP), cholesterol and free fatty acids) were measured via high-performance thin-layer chromatography (HPTLC). Corneocyte maturity was determined via D-Squame® analysis with subsequent double staining (Nile red/involucrin) and evaluation of the emerging red/green signal ratio (27). Transepidermal water loss (TEWL) was measured with a closed chamber system AQUAFLUX AF200 (Biox Systems Ltd, London, UK). For details see Appendix S1.
Statistical analysis
Descriptive statistics were calculated for raw data and calculated values. A significance level of 0.05 (alpha) was chosen for statistical analysis. No adjustments for multiplicity were made. Details are provided in Appendix S1. The computation of the statistical data was carried out with SAS for Windows (SAS Institute GmbH, Heidelberg, Germany) and R V4.1.3 (see Appendix S1; R Foundation for Statistical Computing, Vienna, Austria) (28).
Ethics approval for clinical trials
The trial (NCT05790083) was reviewed by an independent institutional review board (IRB) of the executing clinical research organization (SGS proderm GmbH, Schenefeld, Germany) for ethical approval.
RESULTS
Subjective assessment and diary
The subjective AD burden was assessed using RECAP, peak pruritus NRS-11, and (C)DLQI/IDQOL. Baseline mean RECAP sum scores confirmed that the included population was representative of a patient collective suffering from AD (adults ≥ 18 years: 10.9; SD 5.4; SEM 0.8; n = 51; children/adolescents < 18 years: 10.9; SD 5.1; SEM 0.8; n = 43), being in line with literature (29) (adults ≥ 18 years: 14.0; SD 6.6; n = 218; children/adolescents < 18 years: 13.3; SD 7.4; n = 162), and proprietary data (adults ≥ 18 years: 13.0; SD 5.5; SEM 0.4; n = 159; children < 18 years: 11.4; SD 5.1; SEM 0.4; n = 145; data from concurrent external control study, see Appendix S1).
Over the 12-week trial, a significant improvement (p < 0.001) in mean RECAP sum score with a fast onset in reduction of 54% in the first 4 weeks was seen (Fig. 2A). Similarly, peak pruritus was significantly (p < 0.001) reduced by 53% after 4 weeks, with 64% of participants classifying as positive responders having reached the minimal clinically important difference (MCID) of 2 points on the NRS-11 scale (Fig. 2B/C) (24). The significant reductions for RECAP sum score and peak pruritus NRS-11 score were sustained over 12 weeks and clearly exceeded the external control response (Fig. 2A/B, dotted line; for more details see Appendix S1) (19).
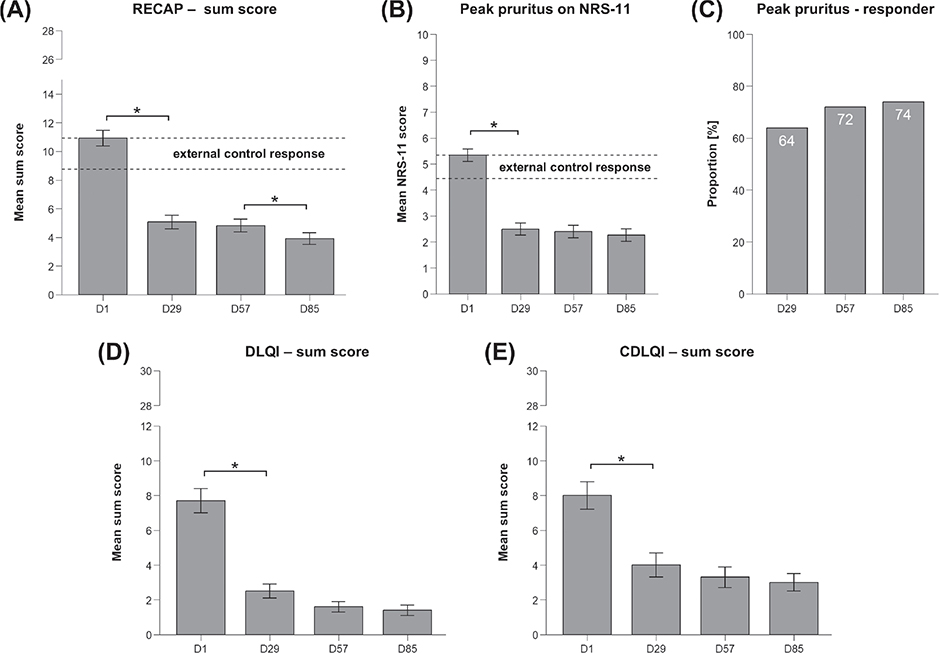
Fig. 2. Subjective evaluation and quality of life. (A) RECAP sum score, n = 92–94, two-sided paired t-test, data represent mean ± SEM, *p ≤ 0.05, Banding (30): 0–1: completely controlled, 2–5: mostly controlled, 6–11: moderately controlled, 12–19: a little controlled, 20–28: not at all controlled, dotted line: external control response (see Appendix S1). (B) Subjective evaluation of peak pruritus according to NRS-11 scale, n = 92–94, two-sided paired Wilcoxon signed-rank test, data represent mean ± SEM, *p ≤ 0.05, dotted line: external control response (see Appendix S1). (C) Proportion of positive responders (%) according to an improvement of peak pruritus by ≥ 2 points defined as responder achieving MCID (24). (D) DLQI sum score, n = 45–48 (age ≥ 16 years), two-sided paired t-test, data represent mean ± SEM, *p ≤ 0.05, Banding: (31): 0–1: no effect at all on patient’s life, 2–5: small effect, 6–10: moderate effect, 11–20: very large effect, 21–30: extremely large effect on patient’s life. (E) CDLQI sum score, n = 38–39, two-sided paired t-test, data represents mean ± SEM, *p ≤ 0.05, Banding (32): 0–1: no effect on child’s life, 2–6: small effect, 7–12: moderate effect, 13–18: very large effect, 19–30: extremely large effect on child’s life.
The skin-related quality of life for adults (≥ 16 years) and children (4–15 years) significantly increased in the first 4 weeks according to the DLQI and CDLQI, respectively, followed by a slight, yet progressive improvement over the remaining 8 weeks (Fig. 2D/E). The data for infants (< 4 years, IDQOL) were not analysed due to the small number of participants (n = 3).
Only 35% of subjects (n = 33) documented at least 1 flare-up in the online diary within the 12 weeks and in only 12% of these cases did the participant use a TCS in relation to the flare-up. Overall, 93% of participants did not use any TCS during the trial. Conversely, in the analogous online diary of the 12-week concurrent RWD control, 96% of participants reported at least 1 flare-up and 73% of participants reporting a flare-up subsequently used a TCS at least once (19).
At the end of the reported trial (D85), more than 90% of the participants were (very) satisfied with the product combination BNO 3731 and BNO 3732 and over 96% of participants stated that the test products were well tolerated.
Objective assessment
In order to substantiate the subjective results, objective AD symptoms were assessed by trained dermatologists at the study centre at the beginning and every 4 weeks thereafter. Significant improvements in erythema, dryness, scaling, and papules were observed at the first assessment (D29) and were sustained and/or, in most cases, even progressive over the following 8 weeks of product application (Fig. 3A/B). Correspondingly, mean vIGA-ADTM scores significantly decreased by 63% over 12 weeks (Fig. 3C). At the end of the trial, 88% of participants were classified as vIGA-ADTM responders (MCID: reduction ≥ 1 point) (26) and 59% had achieved vIGA-ADTM success (improving from score 4/3/2 at baseline by ≥ 2 points to score 1/0) (26) reflecting (almost) complete skin clearance (Fig. 3D).
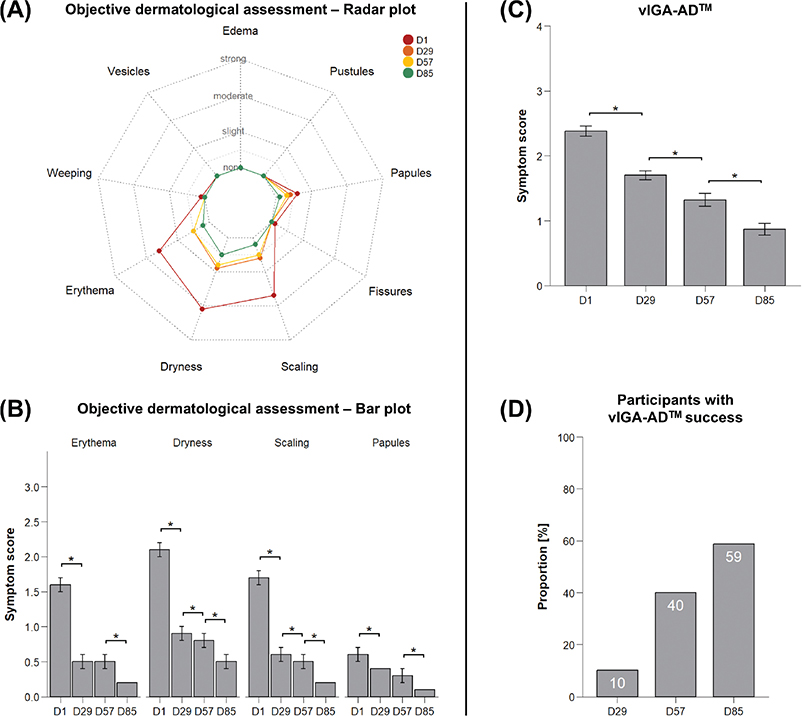
Fig. 3. Objective dermatological evaluation. (A) Radar plot of all parameters of objective dermatological assessment. (B) Symptom score for erythema, dryness, scaling, and papules objectively assessed by a dermatologist, n = 92–94, two-sided paired Wilcoxon signed-rank test, data represent mean ± SEM, *p ≤ 0.05; scoring: 0 = none, 0.5 = very slight, 1 = slight, 2 = moderate, 3 = strong. (C) vIGA-ADTM score, n = 92–94, test: Wilcoxon signed-rank test, data represent mean ± SEM, *p ≤ 0.05, scoring (26): 0: clear, 1: almost clear, 2: mild, 3: moderate, 4: severe. (D) Proportion of subjects achieving vIGA-ADTM success (improvement from score ≥ 2 at baseline (n = 79–80) by ≥ 2 points to vIGA-ADTM score of ≤ 1 at later assessment time) (26) in %.
Instrumental measurements
Stratum corneum sampling by cyanoacrylate stripping (Lipbarvis®) in an adult subpanel (n = 16) and subsequent HPTLC analysis found increased contents of all measured intercellular SC-lipids after 12 weeks of test product application, reaching the level of significance (p ≤ 0.05) for ceramide EOS, ceramide NP, free fatty acids, and cholesterol (Fig. 4).

Fig. 4. Lipid analysis. Contents of intercellular lipids at baseline (D1) and after 12 weeks (D85) of test product(s) application in [ng/133 mm2]; n = 16, test: two-sided paired t-test, data represent mean±SEM, *p ≤ 0.05.
Accordingly, TEM analysis of Lipbarvis® samples indicated a significant (p < 0.001) increase in the mean length of lipid lamellae (D1: mean ± SEM: 61.08 ± 2.17 nm/1,000 nm2 to D85: 196.23 ± 4.01 nm/1,000 nm2; n = 16) (Fig. 5C), reaching a value comparable to healthy skin (approx. 200 nm/1,000 nm2) after 12 weeks (8). Finally, a novel analysis method quantified areas with no or substantially reduced lipid lamellae versus areas with regular lipid lamellae structure (Fig. 5A). The mean area of impaired lipid lamellar structure, indicative of epidermal barrier defects, was significantly (p < 0.001) decreased by 94% (from 53% to 3%) at D85 (Fig. 5B). Taken together, the Lipbarvis® sampling-based evaluations evidenced complete recovery of the intercellular lipid organization in the evaluated subpanel of adults.

Fig. 5. Analysis of lipid lamellae and corneocyte maturity. (A) Colored TEM picture of Lipbarvis® samples taken at baseline (D1) and after 12 weeks (D85), dark brown: corneocyte, orange/brown: areas with regular lipid lamellae, grey: areas with no or substantially reduced lipid lamellae. (B) Proportion of areas with no or substantially reduced lipid lamellae at baseline (D1) and after 12 weeks of test product(s) application (D85) as percentage of total intercellular area, n = 16, two-sided paired t-test, data represent mean±SEM, *p ≤ 0.05. (C) Length of intercellular lipid lamellae (nm/1,000 nm2) at baseline (D1) and after 12 weeks of test product(s) application (D85), n = 16, two-sided paired t-test, data represent mean±SEM, *p ≤ 0.05, indication of skin condition according to Dähnhardt et al. (8). (D) Microscope image of exemplary D-Squame® corneocyte samples (of 1 subject) post-staining at baseline (D1) and after 12 weeks of test product(s) application (D85), red: mature corneocytes, green: immature corneocytes.
In a larger subpanel of adult and child participants (n = 32), D-Squame® analysis was carried out to assess the corneocyte maturity in the epidermis. The ratio of mature to immature corneocytes was significantly (p < 0.001) increased after 12 weeks of test product application (D1: mean ± SEM: 1.260 ± 0.025 to D85: 1.378 ± 0.019; n = 32; Fig. 5D), indicating that the test products supported physiological corneocyte differentiation (11).
Despite the clear improvements seen for all measurements assessing epidermal barrier integrity in a direct manner, the TEWL was not significantly reduced for the evaluated subpanel (n = 32) at the end of the trial period (mean values ± SEM; D1: 13.9 ± 0.7 g/m²h; D85: 13.3 ± 0.8 g/m²h; p = 0.325). Of note, TEWL values for healthy subjects on the lower leg (shin and calf) have been estimated to be in the range of around 2.8–10.2 g/m2h (33, 34) and reported to be increased up to 30 times for compromised epidermis (35).
DISCUSSION
The reported trial assessed the long-term efficacy and tolerability of oil-in-water emulsions BNO 3732 and BNO 3731 containing the ACIs ginger extract and CBD in adults and children suffering from AD. Combining vehicle-type substances with ACIs (13), emollients plus have the potential to exceed the effects of ordinary emollients and skin care routines in basic emollient therapy for AD, which has been indicated in previous clinical studies (10, 16, 36, 37).
Regular application of the test products over 12 weeks significantly improved eczema control, skin-related quality of life, and itch perception as evaluated by PROMs and peak pruritus NRS-11 beyond an external control response derived from complementary RWD of conventional skin care regimes (19). In particular, itch, reportedly the most prevalent, severe, and burdensome symptom of AD, was strongly reduced within the first 4 weeks and remained at a low level throughout the application period with BNO 3731 and BNO 3732 (3). These results complement the previously reported rapid effects in short-term application of the intensive care product BNO 3731 alone, where significant improvements were already observed after 24 h (17). As alleviating itch is the primary therapeutic goal of AD patients, emollients plus providing both fast and long-lasting relief of pruritus are particularly valuable in long-term AD control, e.g., to reduce the need for pharmacological intervention (3). This is substantiated by the diary reports, as merely 12% of participants documented applying TCS in direct relation to a flare-up during the 12‑week application of the emollient plus combination BNO 3731 and BNO 3732. In the concurrent RWD study evaluating individually established skin care regimes, 96% of participants reported at least 1 flare-up during the 12-week period and 73% of these applied a TCS related to a documented flare-up (19).
The sustained subjective improvements were complemented by progressive amelioration of objective AD manifestations including erythema, dryness, scaling, and papules. In respect of the global assessment, 59% of participants with a vIGA-ADTM score of ≥ 2 at baseline achieved complete or almost complete skin clearance by means of the vIGA-ADTM treatment success.
Furthermore, instrumental SC analysis in a subpanel of adults revealed a significant increase of epidermal lipids along with reconstitution of the lipid lamellar structural organization (8, 38). Notably, these lipids were not utilized as individual excipients for BNO 3732 or BNO 3731. Thus, the increased contents indicate de novo lipid synthesis (9, 39). Such changes in the SC lipid composition have already been reported after 5-week application of a marketed body lotion and attributed to the probable ability of human skin to produce elongated fatty acids when provided with suitable precursors (39). Moreover, the physiological lipid synthesis and corneocyte differentiation are very likely supported by anti-inflammatory activity associated with a modulation of the endocannabinoid system, as discussed earlier for the ACI combination ginger extract and cannabidiol (17).
In the present trial, a novel approach towards the assessment of barrier integrity by direct quantification of areas with no or substantially reduced lipid lamellae illustrated the recovery of structural defects in lipid organization of compromised AD skin, as shown in Fig. 5. Notably, the enhanced epidermal barrier integrity was not associated with a significant TEWL decrease. However, as baseline TEWL values were in the range of the skin of healthy subjects, it is plausible that the implemented methodology was not sensible for the included population. Additionally, TEWL represents an indirect barrier measure that does not necessarily reflect barrier integrity compared with electron microscopic visualization (7).
Poor patient adherence is a major hindrance to AD control and has been reported to be insufficient in the real-world setting, particularly for basic emollient therapy (40). Based on the long-lasting efficacy, the high tolerability (only 1 subject with treatment-related adverse events), and the patient-reported product satisfaction, high adherence under real-world conditions can be expected for BNO 3732 and BNO 3731, especially in light of the general acceptance of sustainable plant-based formulations (41).
Limitations
Limitations of the reported trial include the absence of a dedicated control group, which was addressed by the implementation of an external RWD control. Furthermore, the subpanel for instrumental skin barrier analysis was reduced compared with the complete study population (n = 32/16); nevertheless the observed results were significant. Lastly, there were no instructions regarding the amount of products to be used, so a correlation between the magnitude of the effects and the used amounts of the product combination cannot be drawn.
CONCLUSION
Oil-in-water emulsions BNO 3732 and BNO 3731 containing the ACIs ginger extract and cannabidiol with anti-inflammatory and antioxidative in vitro activities are efficacious beyond mere moisturizing and occlusive properties by providing sustained relief of itch, long-lasting improvement of objective AD symptoms, and stabilization of the epidermal permeability barrier. The results show clearly that herbal emollients plus specifically addressing epidermal irritation and pruritus are able to improve basic emollient therapy and offer additional benefits to AD patients beyond conventional emollients. Considering the rising therapeutic significance of emollients plus in AD, clinical studies comparing different products will be of increasing interest for identifying superior formulations in future.
ACKNOWLEDGEMENTS
Medical writing support was provided by Dr. Michael Wördehoff (co.medical, Berlin, Germany).
IRB approval status: The trial was reviewed by an independent institutional review board for ethical approval (SGS proderm GmbH, Schenefeld, Germany).
REFERENCES
- Tian J, Zhang D, Yang Y, Huang Y, Wang L, Yao X, et al. Global epidemiology of atopic dermatitis: a comprehensive systematic analysis and modelling study. Br J Dermatol 2024; 190: 55–61. https://doi.org/10.1093/bjd/ljad339
- Saeki H, Ohya Y, Furuta J, Arakawa H, Ichiyama S, Katsunuma T, et al. English version of Clinical Practice Guidelines for the Management of Atopic Dermatitis 2021. J Dermatol 2022; 49: e315–e375. https://doi.org/10.1111/1346-8138.16527
- Silverberg JI, Mohawk JA, Cirulli J, Nograles K, Punzalan JC, Kelly KM, et al. Burden of disease and unmet needs in atopic dermatitis: results from a patient survey. Dermatitis 2023; 34: 135–144. https://doi.org/10.1089/derm.2022.29015.jsi
- Yosipovitch G, Misery L, Proksch E, Metz M, Ständer S, Schmelz M. Skin barrier damage and itch: review of mechanisms, topical management and future directions. Acta Derm Venereol 2019; 99: 1201–1209. https://doi.org/10.2340/00015555-3296
- Fölster-Holst R, Reimer R, Neumann C, Proksch E, Rodriguez E, Weidinger S, et al. Comparison of epidermal barrier integrity in adults with classic atopic dermatitis, atopic prurigo and non-atopic prurigo nodularis. Biology 2021; 10: 1008. https://doi.org/10.3390/biology10101008
- Fujii M. The pathogenic and therapeutic implications of ceramide abnormalities in atopic dermatitis. Cells 2021; 10: 2386. https://doi.org/10.3390/cells10092386
- Daehnhardt-Pfeiffer S, Surber C, Wilhelm KP, Daehnhardt D, Springmann G, Boettcher M, et al. Noninvasive stratum corneum sampling and electron microscopical examination of skin barrier integrity: pilot study with a topical glycerin formulation for atopic dermatitis. Skin Pharmacol Physiol 2012; 25: 155–161. https://doi.org/10.1159/000336789
- Dähnhardt D, Surber C, Dähnhardt-Pfeiffer S. Influence of topical formulations: lipid lamella organization and lipid composition of stratum corneum as a surrogate marker for barrier integrity. pH of the skin: issues and challenges. Basel: Karger AG, 2018: p. 166–172.
- Blaak J, Dähnhardt D, Bielfeldt S, Theiss C, Simon I, Wilhelm K-P, et al. Improvement of human epidermal barrier structure and lipid profile in xerotic- and atopic-prone skin via application of a plant-oil and urea containing pH 4.5 emulsion. Cosmetics 2023; 10: 95. https://doi.org/10.3390/cosmetics10040095
- Oláh A, Szabó-Papp J, Soeberdt M, Knie U, Dähnhardt-Pfeiffer S, Abels C, et al. Echinacea purpurea-derived alkylamides exhibit potent anti-inflammatory effects and alleviate clinical symptoms of atopic eczema. J Dermatol Sci 2017; 88: 67–77. https://doi.org/10.1016/j.jdermsci.2017.05.015
- Hirao T, Terui T, Takeuchi I, Kobayashi H, Okada M, Takahashi M, et al. Ratio of immature cornified envelopes does not correlate with parakeratosis in inflammatory skin disorders. Exp Dermatol 2003; 12: 591–601. https://doi.org/10.1034/j.1600-0625.2003.00007.x
- Araviiskaia E, Pincelli C, Sparavigna A, Luger T. The role of a novel generation of emollients, ‘emollients plus’, in atopic dermatitis. Clin Cosmet Investig Dermatol 2022; 15: 2705–2719. https://doi.org/10.2147/CCID.S389697
- Wollenberg A, Kinberger M, Arents B, Aszodi N, Avila Valle G, Barbarot S, et al. European guideline (EuroGuiDerm) on atopic eczema – part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol 2022; 36: 1904–1926. https://doi.org/10.1111/jdv.18429
- European Federation of Allergy and Airways Diseases Patients’ Associations. The burden of atopic eczema. European consensus report 2022. 2022 [last accessed 24 September 2024]. Available from: https://www.efanet.org/inform/patient-evidence/atopic-eczema-consensus-europe/report
- Arora P, Shiveena B, Garg M, Kumari S, Goyal A. Curative potency of medicinal plants in management of eczema: a conservative approach. Phytomedicine Plus 2022; 2: 100256. https://doi.org/10.1016/j.phyplu.2022.100256
- Angelova-Fischer I, Rippke F, Richter D, Filbry A, Arrowitz C, Weber T, et al. Stand-alone emollient treatment reduces flares after discontinuation of topical steroid treatment in atopic dermatitis: a double-blind, randomized, vehicle-controlled, left–right comparison study. Acta Derm Venereol 2018; 98: 517–523. https://doi.org/10.2340/00015555-2882
- Neubauer C, Kragl M, Braun T, Filipek P, Rad EB, Grander J, et al. An oil-in-water emulsion containing a combination of ginger extract and synthetic cannabidiol with potent in vitro anti-inflammatory effects ameliorates symptoms of atopic dermatitis in a clinical trial. Eur J Dermatol 2024; 34: 416–424. https://doi.org/10.1684/ejd.2024.4738
- Blicharz L, Rudnicka L, Czuwara J, Waśkiel-Burnat A, Goldust M, Olszewska M, et al. The influence of microbiome dysbiosis and bacterial biofilms on epidermal barrier function in atopic dermatitis: an update. Int J Mol Sci 2021; 22: 8403. https://doi.org/10.3390/ijms22168403
- Andreev S, Neubauer C, Mähler N, Moritz K, Ziegler R, Apfelbacher C, et al. 50th Annual Meeting of the Arbeitsgemeinschaft Dermatologische Forschung (ADF): Therapeutic effects and impact of individual skin care regimes as basic therapy in the management of atopic dermatitis: a remote prospective observational study in adults and children suffering from AD. Exp Dermatol 2024; 33: e14994, P14059. https://doi.org/10.1111/exd.14994
- Howells LM, Chalmers JR, Gran S, Ahmed A, Apfelbacher C, Burton T, et al. Development and initial testing of a new instrument to measure the experience of eczema control in adults and children: recap of atopic eczema (RECAP). Br J Dermatol 2020; 183: 524–536. https://doi.org/10.1111/bjd.18780
- Basra MKA, Fenech R, Gatt RM, Salek MS, Finlay AY. The Dermatology Life Quality Index 1994–2007: a comprehensive review of validation data and clinical results. Br J Dermatol 2008; 159: 997–1035. https://doi.org/10.1111/j.1365-2133.2008.08832.x
- Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol 1995; 132: 942–949. https://doi.org/10.1111/j.1365-2133.1995.tb16953.x
- Lewis-Jones MS, Finlay AY, Dykes PJ. The Infants’ Dermatitis Quality of Life Index. Br J Dermatol 2001; 144: 104–110. https://doi.org/10.1046/j.1365-2133.2001.03960.x
- Yosipovitch G, Reaney M, Mastey V, Eckert L, Abbé A, Nelson L, et al. Peak Pruritus Numerical Rating Scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol 2019; 181: 761–769. https://doi.org/10.1111/bjd.17744
- Thomas KS, Apfelbacher CA, Chalmers JR, Simpson E, Spuls PI, Gerbens LAA, et al. Recommended core outcome instruments for health-related quality of life, long-term control and itch intensity in atopic eczema trials: results of the HOME VII consensus meeting. Br J Dermatol 2021; 185: 139–146. https://doi.org/10.1111/bjd.19751
- Simpson EL, Bissonnette R, Paller AS, King B, Silverberg JI, Reich K, et al. The Validated Investigator Global Assessment for Atopic Dermatitis (vIGA-AD™): a clinical outcome measure for the severity of atopic dermatitis. Br J Dermatol 2022; 187: 531–538. https://doi.org/10.1111/bjd.21615
- Hirao T, Denda M, Takahashi M. Identification of immature cornified envelopes in the barrier-impaired epidermis by characterization of their hydrophobicity and antigenicities of the components. Exp Dermatol 2001; 10: 35–44. https://doi.org/10.1034/j.1600-0625.2001.100105.x
- R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
- Bhanot A, Peters TJ, Ridd MJ. Assessing the validity, responsiveness and reliability of the Recap measure of eczema control. Br J Dermatol 2021; 184: 955–957. https://doi.org/10.1111/bjd.19709
- Zhang J, Ragamin A, Romeijn GLE, Loman L, Oosterhaven JAF, Schuttelaar MLA. Validity, reliability, responsiveness and interpretability of the Recap of atopic eczema (RECAP) questionnaire. Br J Dermatol 2023; 189: 578–587. https://doi.org/10.1093/bjd/ljad247
- Hongbo Y, Thomas CL, Harrison MA, Sam Salek M, Finlay AY. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol 2005; 125: 659–664. https://doi.org/10.1111/j.0022-202X.2005.23621.x
- Waters A, Sandhu D, Beattie P, Ezughah F, Lewis-Jones S. PA-8: Severity stratification of Children’s Dermatology Life Quality Index (CDLQI) scores. Br J Dermatol 2010; 163: 118–130. https://doi.org/10.1111/j.1365-2133.2010.09733.x
- Kottner J, Lichterfeld A, Blume-Peytavi U. Transepidermal water loss in young and aged healthy humans: a systematic review and meta-analysis. Arch Dermatol Res 2013; 305: 315–323. https://doi.org/10.1007/s00403-012-1313-6
- Akdeniz M, Gabriel S, Lichterfeld-Kottner A, Blume-Peytavi U, Kottner J. Transepidermal water loss in healthy adults: a systematic review and meta-analysis update. Br J Dermatol 2018; 179: 1049–1055. https://doi.org/10.1111/bjd.17025
- Boer M, Duchnik E, Maleszka R, Marchlewicz M. Structural and biophysical characteristics of human skin in maintaining proper epidermal barrier function. Adv Dermatol Allergol 2016; 1: 1–5. https://doi.org/10.5114/pdia.2015.48037
- Quadri M, Lotti R, Bonzano L, Ciardo S, Guanti MB, Pellacani G, et al. A novel multi-action emollient plus cream improves skin barrier function in patients with atopic dermatitis: in vitro and clinical evidence. Skin Pharmacol Physiol 2021; 34: 8–18. https://doi.org/10.1159/000513055
- Magnolo N, Jaenicke T, Tsianakas A, Czech W, Thaçi D, Pinter A, et al. Comparison of different skin care regimens in patients with moderate to severe atopic dermatitis receiving systemic treatment: a randomized controlled trial. J Eur Acad Dermatol Venereol 2023; 37: 18–26. https://doi.org/10.1111/jdv.18949
- Bouwstra JA, Nădăban A, Bras W, McAbe C, Bunge A, Gooris GS. The skin barrier: an extraordinary interface with an exceptional lipid organization. Prog Lipid Res 2023; 92: 101252. https://doi.org/10.1016/j.plipres.2023.101252
- Murphy B, Grimshaw S, Hoptroff M, Paterson S, Arnold D, Cawley A, et al. Alteration of barrier properties, stratum corneum ceramides and microbiome composition in response to lotion application on cosmetic dry skin. Sci Rep 2022; 12: 5223. https://doi.org/10.1038/s41598-022-09231-8
- Tier HL, Balogh EA, Bashyam AM, Fleischer AB, Spergel JM, Masicampo EJ, et al. Tolerability of and adherence to topical treatments in atopic dermatitis: a narrative review. Dermatol Ther 2021; 11: 415–431. https://doi.org/10.1007/s13555-021-00500-4
- Maleki-Yazdi KA, Heen AF, Zhao IX, Guyatt GH, Suzumura EA, Makhdami N, et al. Values and preferences of patients and caregivers regarding treatment of atopic dermatitis (eczema): a systematic review. JAMA Dermatology 2023; 159: 320–330. https://doi.org/10.1001/jamadermatol.2022.6045