ORIGINAL REPORT
Impact of Alopecia Areata on Major Life-changing Decisions: Prevalence and Associated Factors
Daniel MUÑOZ-BARBA1,2, Alberto SOTO-MORENO1,2, Sofia HASELGRUBER-DE FRANCISCO1,2, Manuel SÁNCHEZ-DÍAZ1–3, and Salvador ARIAS-SANTIAGO1–4
1Dermatology Unit, Hospital Universitario Virgen de las Nieves, IBS Granada, Granada, Spain, 2Dermatology Department, School of Medicine, University of Granada, Granada, Spain, 3Institute of Biosanitary Research IBS, Granada, Spain, and 4Trichology Clinic, Hospital Universitario Virgen de las Nieves, Granada, Spain
Alopecia areata is a prevalent autoimmune condition causing non-scarring alopecia, with significant impacts on quality of life. However, the long-term effects on major life-changing decisions remain understudied. A cross-sectional study was performed including patients with alopecia areata who attended the Dermatology Department of the Virgen de las Nieves University Hospital. Patients were asked to complete questionnaires to assess the impact of alopecia areata on major life-changing decisions and quality of life. A total of 70 patients were included: 71% were female and 29% were male. The mean age was 38.70 (SD 14.32). The most affected major life-changing decisions were couple relationships and dressing; followed by job performance, social relationships, lifestyle changes, and sports practice. Female gender, higher therapeutic burden, or Dermatology Life Quality Index scores, and lower World Health Organization Five Well Being Index rating were significantly associated with greater major life-changing decisions impairment (p < 0.05). Disease severity and duration did not correlate with increased impact in most major life-changing decisions (p > 0.10). In conclusion, there are some major life-changing decisions that appear to be significantly affected in patients with alopecia areata. The identification of factors associated such us female gender, therapeutic burden, or alterations in mental well-being is crucial to explore and limit the long-term negative effects of the disease.
SIGNIFICANCE
Alopecia areata is an autoimmune disease that causes hair loss, which has a significant impact on patients’ quality of life. A study of 70 patients revealed that alopecia areata often affects important major life-changing decisions, especially couple relationships and dressing, but also job performance, social interactions, lifestyle, and sports practice. Women, people undergoing more lines of treatment, and those with poorer mental well-being reported greater impact on major life-changing decisions. Interestingly, severity or duration of illness was not associated with a greater impact on major life-changing decisions as might be expected. The results highlight the importance of addressing emotional and social factors in alopecia areata care to minimize long-term effects.
Key words: alopecia areata; major life-changing decisions; quality of life.
Citation: Acta Derm Venereol 2025; 105: adv43039. DOI: https://doi.org/10.2340/actadv.v105.43039.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 26, 2025. Accepted after revision: Sep 1, 2025. Published: Sep 10, 2025.
Corr: Manuel Sánchez Díaz, Dermatology Department, Hospital Universitario Virgen de las Nieves, Avenida de las Fuerzas Armadas s/n, ES-18014 Granada, Spain. E-mail: manolo.94.sanchez@gmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Alopecia areata (AA) is an autoimmune disease of the hair follicle that causes non-scarring alopecia and may affect more than 2% of the population (1). There are currently several treatment alternatives, some with very promising results, such as JAK inhibitors (2, 3). Despite these therapeutic developments, AA frequently has a significant negative influence on patients’ quality of life (QoL). The impact of AA on the different psychosocial spheres of both patients and people who live with patients of AA has been extensively studied by several authors (4–7). These studies have been conducted following a traditional health-related QoL research model. This model is characterized by a cross-sectional approach to studying the physical, psychological, and social impact of the disease focusing exclusively on the weeks immediately preceding the clinical consultation. However, new directions in health-related QoL research are moving towards an approach that allows us to assess how certain diseases can have a potentially irreversible long-term impact on the patient’s QoL (8–10).
Within this new perspective, the term Cumulative Life Course Impairment (CLCI) proposed by Kimball et al. has been used to refer to the progressive, cumulative consequences of a chronic condition over time, which may affect an individual’s psychological well-being and overall life trajectory. It is the result of an interaction between stigmatization, physical and psychological comorbidities of the disease, and coping strategies and external factors (11). This interaction often conditions a number of critical decisions in the patient’s life. Bhatti et al. define this set of decisions as Major Life Changing Decisions (MLCDs) (12). They encompass high-stakes, discrete decisions made at specific life stages such as pursuing a career, forming couple relationships, or deciding to have offspring; as well as longer-term everyday choices (e.g., clothing, job performance) all of which may be influenced, postponed, or even avoided due to the burden imposed by a chronic illness. Whereas MLCDs represent identifiable decision points, CLCI reflects the broader longitudinal burden that shapes the context in which these decisions are made and ultimately impacts their long-term outcomes. Subsequently, several studies have been carried out to assess the impact in this context on different dermatological conditions (13–16).
However, to date, scientific evidence regarding the long-term impact of AA on QoL remains scarce (17). Based on the hypothesis that AA exerts a significant CLCI and may condition several MLCDs, the objectives of the present study were: (a) to describe the impact of AA on MLCDs in a cohort of AA patients; (b) to explore the sociodemographic and clinical factors associated with the most affected MLCDs; and (c) to evaluate potential tools to predict deterioration regarding MLCDs in order to assess this aspect in real clinical practice.
MATERIALS AND METHODS
Study design
A cross-sectional study was performed including patients with AA who attended the Dermatology Department between December 2023 and December 2024. Sequential sampling was performed. Patients were asked to complete a series of questionnaires to assess the impact of AA on QoL and mood disturbances.
Inclusion criteria
Inclusion criteria were: (i) patients with a clinical diagnosis of AA, regardless of disease severity, duration, and previous or current treatments; (ii) being diagnosed with AA for almost 6 months; (iii) age 18 years or older; (iv) informed consent to be included in the study; (v) understanding of Spanish language so as to make it possible to complete the questionnaires.
Exclusion criteria
Exclusion criteria were: (i) patient’s refusal to participate in the study; (ii) patients who had any other major disease that may have impacted their mood or MLCDs.
Ethics
The current study was approved by the Research Ethics Committee of Granada and was performed in accordance with the principles of the Declaration of Helsinki.
Variables of interest
Main variables:
(a) Variables related to MLCDs, QoL, and mood disturbances. The following validated questionnaires were collected:
(i) MLCDs Questionnaire: Includes 29 closed questions with 4 possible answers (“Not at all”, “A little”, “Moderately” and “A lot”) corresponding to a Likert scale ranging from 1 to 4 (where 1 corresponded to “Not at all”, and 4 to “A lot”) (18). The questions are grouped into the following domains similar to those proposed by Bhatti et al.: education, professional level, personal relationships, reproductive desires and sexuality, housing and holidays choice, lifestyle changes and sports activity, and toxic habits (19). Two questions are also included to assess the self-perceived severity of AA at the time of the interview and the long-term impact throughout the patient’s life. Finally, an open-ended question was included on what tools have helped the patient to reduce the negative effect of AA on QoL.
(ii) Dermatology Life Quality Index (DLQI): this index serves as a measure of the general dermatological well-being among individuals aged 16 and above. The survey comprises 10 queries, rated on a Likert scale ranging from 0 to 3, where 0 indicates minimal impairment and 3 indicates the most severe. The questions pertain to the preceding week (20, 21).
(iii) World Health Organization Five Well Being Index (WHO-5): It´s a tool to measure the mental well-being experienced by the patient during the last 2 weeks. It consists of 5 questions, with Likert-type scores (0–5), with a higher score corresponding to a greater feeling of well-being. The result of each question is multiplied by 4 and added to the rest to obtain a score of 0–100. Scores < 13 indicate low mental well-being (22, 23).
(iv) Hospital Anxiety and Depression Scale (HADS): This validated survey comprises 14 statements where patients express their level of agreement/disagreement. Each question is rated on a Likert scale. It is divided into 2 sections, with odd-numbered questions assessing anxiety and even-numbered ones evaluating depression. A score of ≥ 8 on either subsection indicates the presence of anxiety or depression, respectively (24, 25).
(b) Variables related to the severity and characteristics of the disease, as evaluated by doctors:
(i) Severity of Alopecia Tool (SALT): This metric indicates the proportion of the scalp impacted by AA (26).
(ii) The existence of total or universal AA (AAT or AAU).
(iii) Affection of special locations (eyebrows, eyelashes, beard, body hair).
(iv) Age of onset, disease duration, previous and current treatments for AA.
(v) Therapeutic burden: score obtained from the sum of the different treatments carried out by the patients up to the time of the consultation. The higher the score, the more lines of treatment performed by the patient, as in other dermatological diseases (27).
Other variables:
Sociodemographic, biometric, and clinical variables (including age, sex, educational level, employment and marital status, tobacco use, and comorbidities) were collected through a multiple-choice section included at the beginning of the self-administered patient questionnaires.
Statistical analysis
Descriptive statistics were used to evaluate the characteristics of the sample. The Shapiro–Wilk test was used to assess the normality of the variables. Continuous variables are expressed as mean and standard deviation (SD). Likert scale scores are expressed as median and interquartile range (IQR). Qualitative variables are expressed as relative and absolute frequency distributions. The χ2 test or Fisher’s exact test, as appropriate, were used to compare nominal variables, and Student’s t-test or the Wilcoxon–Mann–Whitney test were used to compare nominal and continuous data. To explore possible associated factors, simple linear regression was used for continuous variables. The β coefficient and SD were used to predict the log odds of the dependent variable. Statistical significance was considered if p-values were less than 0.05. Statistical analyses were performed using JMP version 14.1.0 (SAS Institute, Cary, NC, USA).
RESULTS
Sociodemographic and clinical features of the sample
One hundred patients were invited to join the study. Finally, a total of 70 patients were included: 71% (50/70) were female and 29% (20/70) were male with a female-to-male ratio of 2.5. All patients had Caucasian skin type. The mean age was 38.7 (SD 14.3) and the mean age of debut was 31.4 (SD 15.2) years old. The majority of participants were non-smokers (71%, 50/70), with university education (63%, 44/70) and active employment (61%, 43/70). Concerning AA, the most frequent form of disease was multiple plaques (55.7%, 39/70), with a mean SALT of 39.3% (SD 39.9) and a mean time of evolution of 7.2 (SD 7.6) years. AA total or universal was present in 25.7% (18/70) of the sample, and 50% (35/70) of the patients presented with alopecia in special locations (eyebrows, eyelashes, beard, or body hair). The most commonly used treatments at the time of consultation were minoxidil 48.6% (34/70), JAK inhibitors 47.1% (33/70), and topical corticosteroids 35.7% (25/70) respectively. Detailed information is given in Table I.
Subjective evaluation of alopecia areata and the impact on Major Life Changing Decisions
Patients were shown to have a median perception that the severity of their AA was moderate (median [IQR] score 3 [2–4]), and that the long-term impact on their lives had been severe (3 [2–4]). Of the 16 participants who answered the open-ended question, 50% (8/16) reported that medical treatment had contributed to lessening the impact of AA; and 25% (4/16) had relied on social relationships.
In terms of MLCDs, it was observed that those most affected in patients with AA were dressing and couple relationships (median score 2 [1–4]). Other MLCDs that were significantly affected were job performance, social and family relationships, changes in lifestyle, sports practice, and the choice of holiday destination (median score 2 [1–3] for all of these). The percentage of patients having moderate or severe impact of disease on most affected MLCDs is shown in Fig. 1.
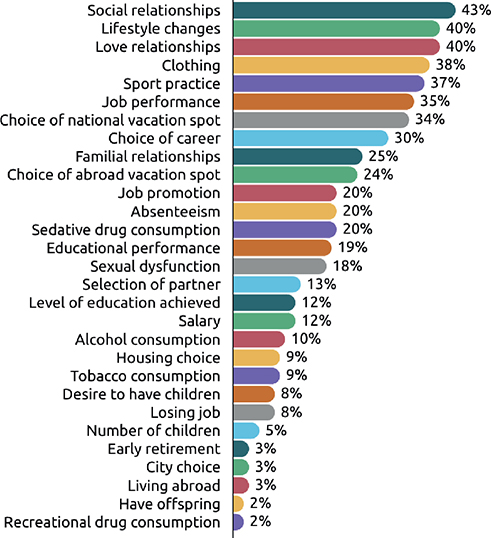
Fig. 1. Percentage of alopecia areata patients with moderate or severe involvement of each of the Major Life Changing Decisions evaluated.
On the other hand, AA seemed to have a negative effect on MLCDs related to leaving work, educational attainment, reproductive desires, housing choice, or having toxic habits, although with a lower intensity than those previously mentioned (mean score 1 [1–1] for all of these). Detailed information is presented in Table II.
Sociodemographic factors association
Univariate analyses were performed to explore the sociodemographic factors associated with the most commonly affected MLCDs in patients with AA. Only the most frequently affected MLCDs were included in the analysis: couple relationships, choice of clothing and holiday destination, job performance, social and family relationships, changes in lifestyle, and sports practice.
Female gender was statistically significantly related to all of the most affected MLCDs (p < 0.05), with the exception of couple relationships, which were highly affected regardless of gender. Concerning the rest of the sociodemographic variables, a greater impact on couple relationships was observed in patients with AA who were younger, single, and smokers (p < 0.05). No statistically significant association was observed between the rest of the MLCDs and demographic features (p > 0.10).
Clinical factors association
No statistically significant associations were observed between the most commonly affected MLCDs and disease duration, severity measured by SALT index, universal or total types of AA, or involvement of special locations (p > 0.10). Patients with higher therapeutic burden scores and those undergoing treatment with JAK inhibitors exhibited a greater impact on social and couple relationships, clothing, holiday choices, and sports practice (p < 0.05).
Association between measures of quality of life, mental well-being, and mood disturbances with the most commonly affected Major Life Changing Decisions in patients with alopecia areata
Lower scores on the WHO-5 well-being index were associated with greater impact on work performance, family and social relationships, choice of holidays, lifestyle changes, and sports practice (p < 0.05). No association was shown with greater impact on clothing and couple relationships (p > 0.10).
Higher impairment in social and family relationships, choice of holidays, changes in healthy habits, sports practice, and dress were statistically significantly associated with higher scores on the DLQI questionnaire and the presence of depressive symptoms assessed by the HADS-D questionnaire scores (p < 0.05), with no association observed with a deterioration in work performance or couple relationships (p > 0.10). Anxiety symptoms assessed by the HADS-A scores were statistically significantly associated with all the most affected MLCDs in patients with AA (p < 0.05).
Evaluation of potential clinical tools to predict impairment of Major Life Changing Decisions
We evaluated the correlation between the impact on all MLCDs and some variables that could serve as tools in real clinical practice to assess the long-term impact of AA. All the results for this section are available in Fig. 2 and Table III.
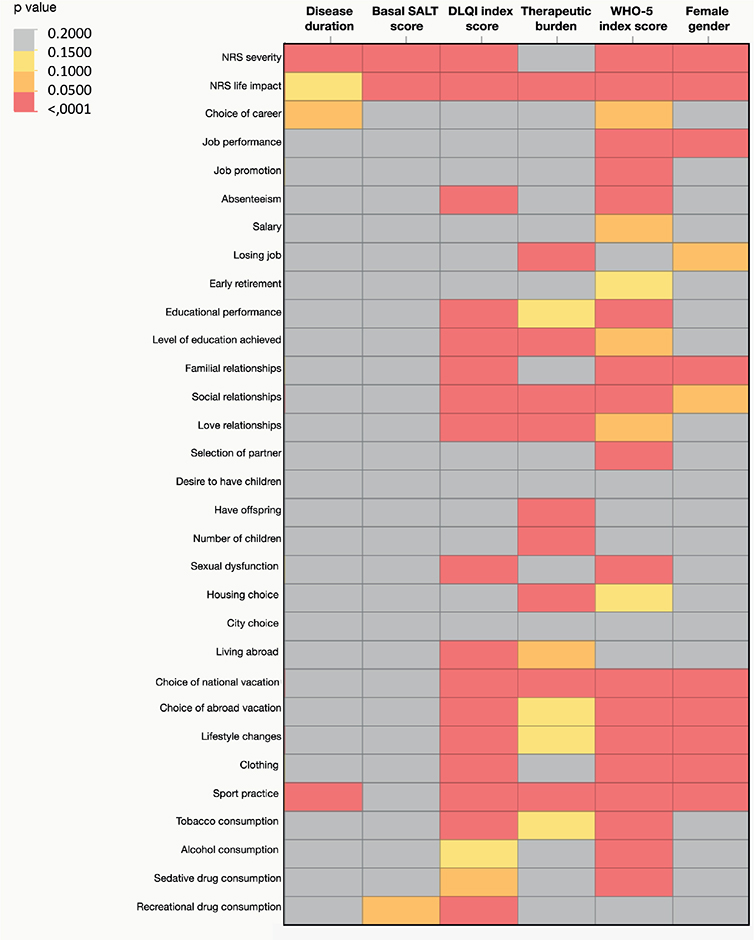
Fig. 2. Evaluation of potential clinical tools to predict impairment of Major Life Changing Decision (MLCD): observed correlations between some sociodemographic, clinical, and quality of life variables with self-perceived severity and long-term impact and with the MLCDs assessed in this study.
Regarding clinical variables, the SALT index was not statistically significantly correlated with any MLCDs (p > 0.05), and the disease duration was only associated with less sports practice (p < 0.05). The therapeutic burden showed a statistically significant correlation with more than one-third of MLCDs explored (34.5% [10/29]; (p < 0.05).
Female gender had a significantly greater impact on MLCDs related to manner of dressing, losing the job, family relationships, choice of holiday destination, and lifestyle habits including sports practice (p < 0.05). An additional analysis regarding differences between the sexes has also been performed to assess possible sex-adjusted differences in respect of the main predictor variables studied. It was observed that female patients had a longer duration of illness, with significantly lower SALT scores, but still had a significant loss of mental well-being compared with males (p < 0.05). Detailed information is given in Table IV.
On the other hand, higher scores on the DLQI correlated with a significantly greater impact on the MLCDs mentioned above in the gender dimension, in addition to educational performance, all forms of relationships assessed, sexual dysfunction, and tobacco or recreational drug use (p < 0.05). Lower scores on the WHO-5 well-being index showed the strongest correlation with the impact on MLCDs (68.9%, 20/29), particularly in work-related aspects, all types of relationships evaluated, clothing, lifestyle changes, vacation destination choice, and toxic substance consumption (p < 0.05).
Finally, most of the variables studied as potential predictive tools demonstrated a strong correlation with patient-perceived severity and long-term impact (p < 0.05).
DISCUSSION
The results of our study suggest that AA exerts a considerable CLCI, influencing a range of MLCDs that patients must make throughout their lives. Some variables, such as female sex, a greater number of treatments and the lower sense of well-being as measured by the WHO-5 scale, seem to correlate with a greater deterioration of MLCDs in general terms.
The main MLCDs affected in patients with AA were couple relationships and manner of dressing. Recent studies support this impact on relationships, which are largely affected irrespective of gender because of the feelings of shame, anxiety, and loss of self-esteem that are common in patients with AA (28). On the other hand, hair is identified as a symbol of gender, age, beauty, status, and health, among others (29). For all these reasons, hair loss can condition the way in which patients tend to dress, forcing them to use camouflage measures to reduce the negative impact (30).
Job performance, social and family relationships, changes in lifestyle habits, sports practice, and choice of holiday destination were the other MLCDs most affected in the cohort of patients evaluated. This is consistent with other studies showing how patients with AA have a higher risk of absenteeism, unemployment, and loss of work productivity in relation to the presence of physical symptoms, eyebrow/eyelash involvement, and perceived severity of the disease, especially in women (31–33). As with couple relationships, social and family relations are also affected in patients with AA (32). In previous studies, patients reported social isolation, reduced interactions with friends, and withdrawal from leisure activities due to feelings of rejection, intimidation, and embarrassment about their appearance. At the family level, even explaining AA to children was emotionally challenging, as children expressed distress and fear of experiencing the same loss in the future as their parents (34).
In terms of clinical factors associated with greater long-term impairment, the impact of AA on MLCDs appears to be greater in women than in men, despite having less severe forms of the disease in the cohort studied. This is consistent with what has been observed in other pathologies such as atopic dermatitis, psoriasis, or hidradenitis suppurativa, where being female has been found to predispose to certain outcomes such as higher rates of mental illness that accentuate the suffering caused by the disease (35). We will have to pay special attention to this group of patients to try to fight this gender gap.
On the other hand, objective severity as measured by the SALT index or years of evolution will not serve as tools to explore CLCI in patients with AA. However, having a higher therapeutic burden or having required treatment with JAK inhibitors should alert us to ask specifically about this long-term impact, as correlations were observed with up to one-third of the MLCDs assessed. It is possible that cumulative fatigue, frustration, and anxiety due to failure to respond to various lines of treatment may contribute to increased CLCI.
Finally, the WHO-5 well-being questionnaire proved to be a useful, quick and easy tool to explore the impact of most MLCDs. There are no studies to date assessing the impact on quality of life using the WHO-5 in patients with AA. Patients with altered scores on this questionnaire, especially if they have mood disturbances or altered scores on other tests such as the DLQI, should be specifically questioned to try to detect and at least alleviate this long-term impact.
The main limitations of the current study are: its cross-sectional nature, which makes it impossible to assess causality, the probable overrepresentation of patients with more severe disease, and the limited sample size, especially for men, which could have led to limited detection of statistical differences.
In conclusion, there are some MLCDs that appear to be significantly affected in patients with AA such as social relationships, clothing, job performance, changes in lifestyle, or sports practice. The identification of factors associated with a greater impact on MLCDs like female gender, therapeutic burden, or alterations in mental well-being is crucial to explore and limit the long-term negative effects of the disease. Further studies are needed to understand the multidimensionality and CLCI of the disease in order to provide holistic care for patients with AA.
ACKNOWLEDGEMENTS
This article will be part of the doctoral thesis of Daniel Muñoz-Barba.
REFERENCES
- Sibbald C. Alopecia areata: an updated review for 2023. J Cutan Med Surg 2023; 27: 241–259. https://doi.org/10.1177/12034754231168839
- Alhanshali L, Buontempo MG, Lo Sicco KI, Shapiro J. Alopecia areata: burden of disease, approach to treatment, and current unmet needs. Clin Cosmet Investig Dermatol 2023; 16: 803–820. https://doi.org/10.2147/CCID.S376096
- Wei D, Chen Y, Shen Y, Xie B, Song X. Efficacy and safety of different JAK inhibitors in the treatment of alopecia areata: a network meta-analysis. Front Immunol 2023; 14: 1152513. https://doi.org/10.3389/fimmu.2023.1152513
- Vañó-Galván S, Blume-Peytavi U, Farrant P, Reygagne P, Johansson E, Reed C, et al. Physician- and patient-reported severity and quality of life impact of alopecia areata: results from a real-world survey in five European countries. Dermatol Ther 2023; 13: 3121–3135. https://doi.org/10.1007/s13555-023-01057-0
- Lauron S, Plasse C, Vaysset M, D’Incan M, Rondepierre F, Jalenques I. Prevalence and odds of depressive and anxiety disorders and symptoms in children and adults with alopecia areata: a systematic review and meta-analysis. JAMA Dermatol 2023; 159: 281–288. https://doi.org/10.1001/jamadermatol.2022.6085
- Sánchez-Díaz M, Díaz-Calvillo P, Ureña-Paniego CA, Molina-Leyva A, Arias-Santiago S. Quality of life and mood status disturbances in cohabitants of patients with alopecia areata: a cross-sectional study in a Spanish population. Int J Environ Res Public Health 2022; 19: 16323. https://doi.org/10.3390/ijerph192316323
- Sánchez-Díaz M, Montero-Vílchez T, Cuenca-Barrales C, Molina-Leyva A, Arias-Santiago S . Prevalence and implications of type D personality in patients with alopecia areata: a marker of quality-of-life impairment and mood status disturbances, a comparative study. J Eur Acad Dermatol Venereol 2023; 37: 1064–1070. https://doi.org/10.1111/jdv.18733
- Mayer KU. New directions in life course research. Annu Rev Sociol 2009; 35: 413–433. https://doi.org/10.1146/annurev.soc.34.040507.134619
- Lynch J, Smith GD. A life course approach to chronic disease epidemiology. Annu Rev Public Health 2005; 26: 1–35. https://doi.org/10.1146/annurev.publhealth.26.021304.144505
- Ben-Shlomo Y, Kuh D. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol 2002; 31: 285–293. https://doi.org/10.1093/ije/31.2.285
- Kimball A, Gieler U, Linder D, Sampogna F, Warren R, Augustin M. Psoriasis: is the impairment to a patient’s life cumulative? J Eur Acad Dermatol Venereol 2010; 24: 989–1004. https://doi.org/10.1111/j.1468-3083.2010.03705.x
- Bhatti Z, Salek M, Finlay A. Major life changing decisions and cumulative life course impairment. J Eur Acad Dermatol Venereol 2011; 25: 245–246. https://doi.org/10.1111/j.1468-3083.2010.03930.x
- Krüger C, Schallreuter KU. Cumulative life course impairment in vitiligo. Curr Probl Dermatol 2013; 44: 102–117. https://doi.org/10.1159/000350010
- Augustin M. Cumulative life course impairment in chronic wounds. Curr Probl Dermatol 2013; 44: 125–129. https://doi.org/10.1159/000350789
- Fine JD. Cumulative life course impairment by epidermolysis bullosa. Curr Probl Dermatol 2013; 44: 91–101. https://doi.org/10.1159/000350009
- Piaserico S. Cumulative life course impairment in melanoma and nonmelanoma skin cancer. Curr Probl Dermatol 2013; 44: 118–124. https://doi.org/10.1159/000350055
- Burns LJ, Mesinkovska N, Kranz D, Ellison A, Senna MM. Cumulative life course impairment of alopecia areata. Int J Trichology 2020; 12: 197–204. https://doi.org/10.4103/ijt.ijt_99_20
- Jebb AT, Ng V, Tay L. A review of key Likert scale development advances: 1995–2019. Front Psycho 2021; 12: 637547. https://doi.org/10.3389/fpsyg.2021.637547
- Bhatti ZU, Salek SS, Bolton CE, George L, Halcox JP, Jones S, et al. The development and validation of the major life changing decision profile (MLCDP). Health Qual Life Outcomes 2013; 11: 78. https://doi.org/10.1186/1477-7525-11-78
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- de Tiedra AG, Mercadal J, Badía X, Mascaró JM, Herdman M, Lozano R. Adaptación transcultural al español del cuestionario Dermatology Life Quality Index (DLQI): El Índice de Calidad de Vida en Dermatología. Actas Dermo-Sifiliográficas 1998; 89: 692–700.
- Carrozzino D, Christensen KS, Patierno C, Woźniewicz A, Møller SB, Arendt ITP, et al. Cross-cultural validity of the WHO-5 Well-Being Index and Euthymia Scale: a clinimetric analysis. J Affect Disord 2022; 311: 276–283. https://doi.org/10.1016/j.jad.2022.05.111
- Psykiatric Center North Zealand. WHO‑5 Questionnaires [Internet]. Hillerød (Denmark): Region Hovedstadens Psykiatri. Available from: https://www.psykiatri-regionh.dk/who-5/who-5-questionnaires/Pages/default.aspx
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983; 67: 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
- Vilela-Estrada AL, Villarreal-Zegarra D, Copez-Lonzoy A, Esenarro-Valencia L, Sánchez-Ramírez JC, Lamas-Delgado F, et al. Psychometric properties of the Spanish version of the hospital anxiety and depression scale in cancer patients. Front Psychol. 2024; 15: 1497946. https://doi.org/10.3389/fpsyg.2024.1497946
- Olsen EA, Canfield D. SALT II: a new take on the Severity of Alopecia Tool (SALT) for determining percentage scalp hair loss. J Am Acad Dermatol 2016; 75: 1268–1270. https://doi.org/10.1016/j.jaad.2016.08.042
- Haselgruber S, Muñoz-Barba D, Leon-Pérez FJ, Cuenca-Barrales C, Arias-Santiago S, Molina-Leyva A. Therapeutic burden in hidradenitis suppurativa: a cross-sectional study of 557 patients. Int J Dermatol 2025; 64: 539–545. https://doi.org/10.1111/ijd.17517
- Li SJ, Huang KP, Joyce C, Mostaghimi A. The impact of alopecia areata on sexual quality of life. Int J Trichology 2018; 10: 271–274. https://doi.org/10.4103/ijt.ijt_93_18
- Cash TF. The psychology of hair loss and its implications for patient care. Clin Dermatol 2001; 19(2): 161–166. https://doi.org/10.1016/s0738-081x(00)00127-9
- Kacar SD, Soyucok E, Bagcioglu E, Ozuguz P, Coskun KS, Asık AH, et al. The perceived stigma in patients with alopecia and mental disorder: a comparative study. Int J Trichology 2016; 8: 135–140. https://doi.org/10.4103/0974-7753.189005
- Macbeth AE, Holmes S, Harries M, Chiu WS, Tziotzios C, de Lusignan S, et al. The associated burden of mental health conditions in alopecia areata: a population-based study in UK primary care. Br J Dermatol 2022; 187: 73–81. https://doi.org/10.1111/bjd.21055
- Aldhouse NVJ, Kitchen H, Knight S, Macey J, Nunes FP, Dutronc Y, et al. “‘You lose your hair, what’s the big deal?’ I was so embarrassed, I was so self-conscious, I was so depressed:” a qualitative interview study to understand the psychosocial burden of alopecia areata. J Patient-Rep Outcomes 2020; 4: 76. https://doi.org/10.1186/s41687-020-00240-7
- Senna M, Ko J, Glashofer M, Walker C, Ball S, Edson-Heredia E, et al. Predictors of QOL in patients with alopecia areata. J Invest Dermatol 2022; 142: 2646–2650.e3. https://doi.org/10.1016/j.jid.2022.02.019
- Mesinkovska N, King B, Mirmirani P, Ko J, Cassella J. Burden of illness in alopecia areata: a cross-sectional online survey study. J Investig Dermatol Symp Proc 2020; 20: S62–S68. https://doi.org/10.1016/j.jisp.2020.05.007
- von Stülpnagel CC, Augustin M, Düpmann L, da Silva N, Sommer R. Mapping risk factors for cumulative life course impairment in patients with chronic skin diseases: a systematic review. J Eur Acad Dermatol Venereol 2021; 35: 2166–2184. https://doi.org/10.1111/jdv.17348