ORIGINAL REPORT
Impact of Long-term Stability on Mental Health in Adults with Atopic Dermatitis: A Cohort Study with Unsupervised Cluster Analysis
Lea K. NYMAND1,3  , Mia-Louise NIELSEN1 , Maria Oberländer CHRISTENSEN1 , Simon F. THOMSEN1,3 , Jacob P. THYSSEN1,2 and Alexander EGEBERG1,2
, Mia-Louise NIELSEN1 , Maria Oberländer CHRISTENSEN1 , Simon F. THOMSEN1,3 , Jacob P. THYSSEN1,2 and Alexander EGEBERG1,2
1Department of Dermatology and Venereology, Bispebjerg and Frederiksberg Hospital, University of Copenhagen, Copenhagen NV, 2Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, and 3Department of Biomedical Sciences, University of Copenhagen, Copenhagen, Denmark
Atopic dermatitis (AD) is a heterogeneous disease characterized by unpredictable flares, potentially leading to impaired mental health. Adult patients with a dermatologist-verified AD diagnosis received after their 18th birthday were grouped according to patient-reported flare activity between 2018 and 2023. The k-means clustering algorithm was used in combination with dynamic time warping and barycenter averaging. Clusters were analysed according to current levels of anxiety and depression and severity across the 4 time points. The clustering method divided the 262 patients into 4 groups. Cluster 1 was characterized by a disease course with an average of < 6 annual flares, a median (interquartile range) anxiety and depression score of 3.0 (1.0–6.3), and 1.0 (0.0–4.0), respectively. Clusters 2 and 3 were characterized by annual flares ranging from 4 to 16 and anxiety scores of 6.0 (3.0–8.5) and 4.0 (2.0–7.0) and depression scores of 3.0 (1.0–6.0) and 2.0 (1.0–5.0), respectively. Cluster 4 was characterized by an unstable disease course with an average of ≥ 14 yearly flares, and anxiety and depression scores similar to cluster 2. Patients characterized by an unstable moderate disease course were more burdened compared with patients with a stable disease course (p = 0.03). This emphasizes the importance of long-term flare patterns in clinical decision-making.
SIGNIFICANCE
In this study, adult patients with moderate severe atopic dermatitis and unstable disease progression displayed significantly higher levels of anxiety compared with those with stable progression. Long-term stability of atopic dermatitis and flare patterns should be considered by the physician in the assessment of severity and treatment decisions.
Key words: anxiety; atopic dermatitis; depression; flares; long-term stability; severity.
Citation: Acta Derm Venereol 2025; 105: adv43071. DOI: https://doi.org/10.2340/actadv.v105.43071.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 31, 2025. Accepted after revision: Jun 11, 2025. Published: Jul 1, 2025.
Corr: Lea Krog Nymand, Department of Dermatology, Bispebjerg Hospital, Nielsine Nielsens Vej 17, opgang 9, DK-2400 Copenhagen, Denmark. E-mail: lea.krog.nymand@regionh.dk
Competing interests and funding: LKN has nothing to declare. M-LN has received consultancy honoraria from LEO Pharma. MOC: has been a sub-investigator for LEO Pharma. With no relation to the present manuscript SFT has been a speaker or has served on advisory boards for Sanofi, AbbVie, LEO Pharma, Pfizer, Eli Lilly, Novartis, UCB Pharma, Union Therapeutics, Almirall, and Janssen Pharmaceuticals, and has received research support from Sanofi, AbbVie, LEO Pharma, Novartis, UCB Pharma, and Janssen Pharmaceuticals. Unrelated to the present study, JPT has been an adviser for AbbVie, Almirall, Arena Pharmaceuticals, Coloplast, OM Pharma, Aslan Pharmaceuticals, Union Therapeutics, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, a speaker for AbbVie, Almirall, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, and received research grants from Pfizer, Regeneron, and Sanofi-Genzyme. Dr Thyssen is a full-time employee at LEO Pharma. Unrelated to the present study, AE has received research funding from Pfizer, Eli Lilly, Novartis, Bristol-Myers Squibb, AbbVie, Janssen Pharmaceuticals, Boehringer Ingelheim, the Danish National Psoriasis Foundation, the Simon Spies Foundation, and the Kgl Hofbundtmager Aage Bang Foundation, and honoraria as consultant and/or speaker from Amgen, AbbVie, Almirall, Leo Pharma, Zuellig Pharma Ltd, Galápagos NV, Sun Pharmaceuticals, Samsung Bioepis Co., Ltd, Pfizer, Eli Lilly and Company, Novartis, Union Therapeutics, Galderma, Dermavant, UCB, Mylan, Bristol-Myers Squibb, McNeil Consumer Healthcare, Horizon Therapeutics, Boehringer Ingelheim, and Janssen Pharmaceuticals. He is currently employed by LEO Pharma.
This research received partial funding from AbbVie A/S. The study protocol was designed in collaboration with AbbVie. Once the study protocol was approved, AbbVie had no influence on conduct of the study, data analysis or interpretation of the results, writing of the manuscript, or the decision to submit for publication.
INTRODUCTION
A topic dermatitis (AD) is a common heterogeneous skin disease predominantly debuting in early childhood. Clinically, AD presents as a red and scaly rash and symptoms include pruritus and a burning skin sensation (1). Moreover, the disease course is often unpredictable, with either persistent or relapsing lesions and frequent flaring; however, the underlying mechanisms of AD flares are still not fully understood. In addition to the burden caused by skin-related symptoms, flares may inflict a tremendous negative impact on patients’ quality of life. AD has further been associated with sleep disturbance and mental health problems, including stress, fatigue, anxiety, depression, and suicidal ideation (2–6).
Current diagnostic criteria are based on clinical and historical features, including morphology and distribution of skin lesions. Furthermore, patients are often stratified into mild, moderate, or severe AD based on patient-reported or physician-assessed signs and symptoms (7–10). AD is notable for the chronically relapsing course and flare patterns are essential features that may be considered as part of the AD phenotypes (11).
Studies have demonstrated that only 24% of patients and caregivers feel confident in managing AD flares, and 75% of patients and caregivers feel that being able to effectively control AD would be the single most important improvement to their own or their child’s quality of life (12). This highlights the importance of prioritizing stability of disease and flare patterns in the treatment of AD. However, current treatment guidelines are often based solely on severity subgrouping and do not account for the disease course and impact of flares.
This study used machine-learning and longitudinal data on flares to investigate the impact of stability in disease trajectories on anxiety and depression in patients with AD.
MATERIALS AND METHODS
The study was registered in the Capital Region’s Inventory (Videnscenter for Dataanmeldelser, ref. P-2021-386). All participants gave written informed consent and allowed processing of personal information. This constitutes the necessary legal requirements, and ethical approval is not required for this type of study in Denmark.
Data sources and study population: the Danish Skin Cohort
The Danish Skin Cohort (DSC) was established as an inception cohort in 2018, and is described in detail elsewhere (11, 13). Data on patients with AD were collected from May to July in 2018, in October to November of 2020, and in January to February of 2022 and 2023, respectively. Patients were invited to participate if they had a dermatologist-verified diagnosis of AD occurring at least once after their 18th birthday. Eligible patients were asked to respond to the survey electronically through an invitation in their personal and secure governmentally run mailbox. In the case of nonresponse, patients were either called by phone (in 2018, 2020) or sent 2 reminders after 1 and 2 weeks, respectively (in 2022, 2023).
Patient-reported number of flares within the past 12 months was collected through the survey, with a flare being defined as “an acute, clinically significant worsening of signs and symptoms of AD requiring therapeutic intervention” according to the European Task Force of Atopic Dermatitis (ETFAD) (14). Patients were instructed to consider multiple consecutive days with significant worsening as a single flare and to select a maximum of 20 flares.
Additional information included lifestyle factors (smoking, BMI), skin pain, skin itch, and sleep disturbance (numeric rating scale [NRS]), AD characteristics (disease severity [PO-SCORAD], body surface area (BSA), age at disease onset, Dermatology Life Quality Index [DLQI]), and depression and anxiety score measured by the Hospital Anxiety and Depression Score (HADS). Severity of AD was defined based on PO-SCORAD as mild (0–25), moderate (25–50), and severe (> 50), and DLQI was stratified by no (0–1), small (2–5), moderate (6–10), very large (11–20), and extremely large impact (21–30) on life quality (15). Both HADS anxiety and depression levels were defined as normal (0–7), borderline abnormal (8–10), and abnormal (11–21) (16). Demographic information on age and sex was obtained from the Danish Central Person Register (CPR).
Data were collected and managed with the Research Electronic Data Capture (REDCap; https://project-redcap.org/) tool hosted at the Capital Region of Denmark. REDCap is a secure, web-based software platform designed to support data capture for research studies (17, 18).
Statistical analysis
Current (2023) HADS scores were analysed in relation to PO-SCORAD, DLQI, and long-term stability with data from years 2018, 2020, 2022, and 2023. To identify long-term flare patterns, unsupervised cluster analysis was performed on yearly number of flares. To handle the time-series aspect of the data, the widely used unsupervised k-means clustering was combined with “dynamic time warping” (DTW) (19). DTW is a measure of the distance between data points that accounts for the possible shift in time, as opposed to the Euclidian distance. As the analysis was unsupervised, the “Silhouette score” was used to determine the optimal number of clusters (20). The silhouette score is a measure of the cohesion within each cluster and the separation between clusters. The optimal number of clusters is the point that balances cohesion and separation. Furthermore, a global averaging strategy called DTW barycenter averaging (DBA) was used to estimate the average shapes of the trajectories for the clusters, henceforth referred to as “average” as opposed to the commonly used “mean” (19). To ensure that clusters not only expressed severity differences, patients were divided into severity groups according to PO-SCORAD as a sub-analysis.
Descriptive statistics present the characteristics of patients with AD. Categorical data were presented using frequency with percentages and normally distributed continuous variables were presented with means and standard deviations (SDs), while non-normally distributed continuous variables were presented with median with interquartile range (IQR). Correlations were assessed with Spearman’s or Kendall’s rank test and comparisons between clusters or severity groups were tested using the Wilcoxon rank-sum test and regression analysis.
Statistical analysis was conducted using RProject software, version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) with packages “Tableone” and Python version 3.7.6 (Python Software Foundation, Wilmington, DE, USA), including relevant packages (21).
RESULTS
A total of 262 patients provided complete flare and severity data between 2018 and 2023, and current anxiety and depression score at the last time point (Table I). There was a female predominance (67.9%), and the mean (SD) age was 51.9 (12.1) years. Around half of patients (49.7%) had a smoking history and mean BMI was 26.3 (5.2) kg/m2. Current mean BSA was 13%, while worst-ever was 40%. The overall median (IQR) number of flares reported in 2023 was 6.0 (3.0–12.0), whereas the median (IQR) HADS was 4.0 (1.3–7.0) for anxiety and 2.0 (1.0–5.0) for depression. A weak correlation was observed between number of flares in 2023 and level of anxiety and depression (τ = 0.14, p < 0.005 and τ = 0.17, p < 0.0005).
Patient clusters
A total of 4 patient clusters were identified (Fig. S1), comprising 91, 48, 74, and 49 patients. These had similar baseline characteristics, except for smoking habits and current BSA. A higher percentage of patients were daily/occasional smokers in clusters 2 and 4 (14.6% and 14.3%), compared with clusters 1 and 3 (6.6% and 6.8%). In addition, clusters 2 and 4 reported the highest mean (SD) current BSA (13.6 [20.5] and 23.0 [24.5] compared with 9.5 [14.6] and 9.8 [12.9] for clusters 1 and 3).
Cluster 1 was characterized by a stable disease trajectory with an average of < 6 annual flares, a median (IQR) PO-SCORAD changing from 33.1 (20.0–40.7) to 28.4 (20.7–36.2), and current median DLQI of 2.00 (1.75–5.00). The median (IQR) current anxiety score was 3.0 (1.0–6.3) and the depression score was 1.0 (0.0–4.0) (Fig. 1).
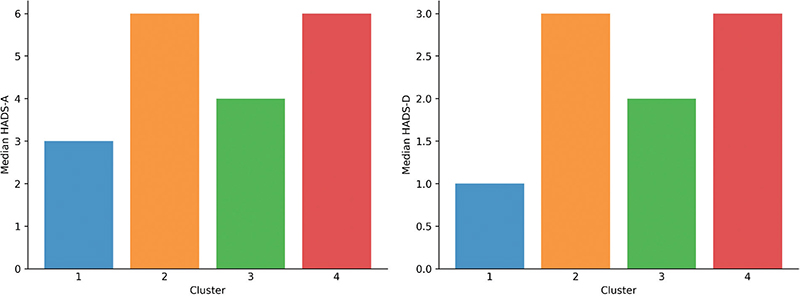
Fig. 1. Anxiety and depression median score for the 4 clusters.
Cluster 2 exhibited an unstable disease course with varying number of flares but an overall improvement from 16 flares initially to 6 flares at last time point. This cluster was characterized by a moderate median (IQR) severity score decreasing from 45.4 (37.0–56.2) to 32.8 (24.4–45.4) across the study period. The DLQI ranged between 5.0 (2.0.9.0) and 7.0 (3.0–11.8) (Fig. 2), while the median current anxiety score was 6.0 (3.0–8.5) and the depression score was 3.0 (1.0–6.0) (see Fig. 1).
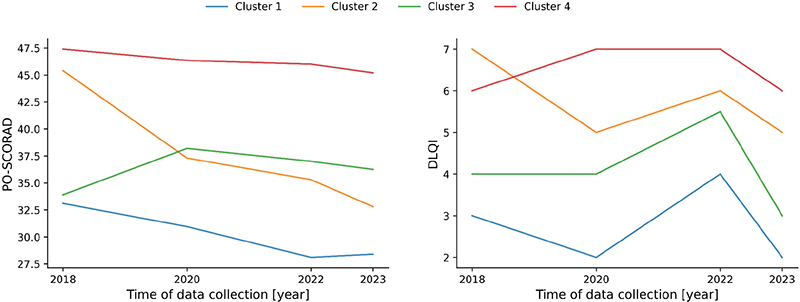
Fig. 2. PO-SCORAD and DLQI score for the 4 time points for the 4 clusters.
Cluster 3 displayed an unstable disease course and a fluctuating number of flares with an overall worsening (from annual 5 flares, increasing to ≥ 8 at later time points). Cluster 3 had a severity score fluctuating between 33.9–38.2, a DLQI of 3.0–5.5 (see Fig. 2), whereas the median current anxiety score was 4.0 (2.0–7.0) and the depression score was 2.0 (1.0–5.0) (see Fig. 1).
Cluster 4 was characterized by a consistently unstable trajectory with a persistently high number of yearly flares ranging between 14 and 20 on average, and a median severity score decreasing slightly from 47.4 (33.4–60.2) to 45.2 (37.8–53.8) across the study period. The DLQI was consistently moderate (Fig. 2 and Fig. 3), and the current anxiety score was 6.0 (2.0–8.0) and the depression score was 3.0 (1.0–6.0) (see Fig. 1).
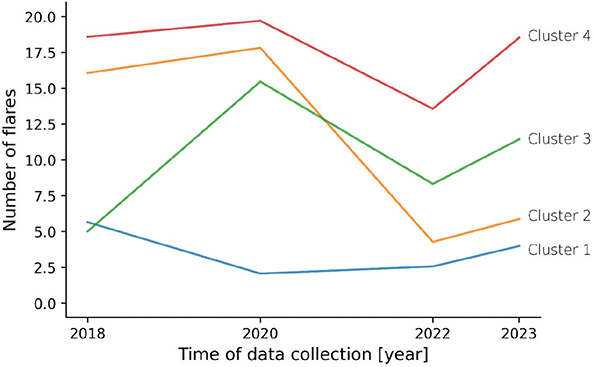
Fig. 3. Average number of flares at the 4 time points for the 4 clusters.
With cluster 1 being the most stable of the 4 clusters, significantly higher anxiety and depression scores were observed for cluster 2 (p = 0.002 and p = 0.002) and cluster 4 (p = 0.003 and p = 0.003), but not for cluster 3 (p = 0.074 and p = 0.235).
A sub-analysis on treatment demonstrated that 16.2–20.8% and 18.9–22.9% of patients in clusters 1, 2, and 3 received immunosuppressive medication “at the moment or within the past 12 months” in 2022 and 2023, respectively, as opposed to only 10.2% and 12.2% in cluster 4.
Sensitivity analysis
Considering cluster 1 as the stable group with consistently few yearly flares, while combining clusters 2, 3, and 4 that all exhibited more annual flares, results in 2 groups with a stable and an unstable disease course, respectively. To counteract the influence of severity, both groups were stratified in mild, moderate, and severe subgroups according to current PO-SCORAD, yielding a total of6 groups (Table SI and Fig. 4). The unstable moderate group was the largest with 97 patients (37.0%). All other groups were smaller (≤ 42 patients each) with the stable severe group including only 12 patients. Except for the stable severe group, all groups had a predominance of women (69.0–73.5%), and skin pain, itch, and sleep disturbance increased with severity and instability (ρ = 0.6, p < 0.001, ρ = 0.7. p < 0.001, and ρ = 0.4, p < 0.001) (Table SI). The anxiety level within the moderate group differed significantly based on stability (p = 0.03). Both the stable/unstable mild group and the stable moderate group had similar anxiety scores. Likewise, the stable/unstable severe group and the unstable moderate group had anxiety scores of ≥ 5. The same pattern was observed for depression (Fig. 4).
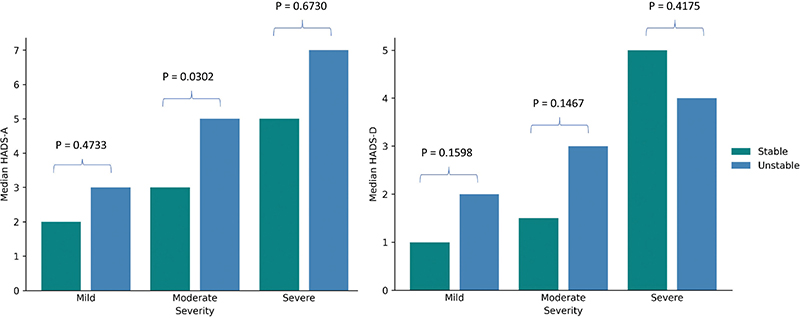
Fig. 4. Differences in anxiety and depression scores for the stable and unstable severity groups.
DISCUSSION
The cluster analysis identified 4 clusters with different disease courses defined by AD flare patterns. We found that those who exhibited more unstable disease courses had significantly higher anxiety and depression scores compared with patients with stable disease. Notably, patients with moderately severe AD but unstable disease displayed significantly higher levels of anxiety, compared with stable moderate AD, emphasizing the need for long-term stability in this population. In addition, the less frequent use of immunosuppressive treatment in cluster 4 may help explain why these patients experience a more severe AD trajectory and frequent flares over time. However, while they may be using topicals, these appear to be ineffective. This may also have negatively influenced patients’ HADS score.
A previous large-scale study reported that 55% of the included patients were either always or sometimes worried about the next AD flare – a pattern that was especially prominent among patients with severe AD (65%) (12). This emphasizes the burden of flares in AD patients, despite the lack of research into the direct link between the stability of the disease course and mental health. Besides the impact of sleep deprivation caused by symptoms such as itching, studies suggest a neuroimmune link between AD and mental health. The believed profile of pro-inflammatory cytokines in AD varies depending on whether the disease is in an acute or chronic phase. The acute phase is dominated by a T helper 2 (Th2)-skewed immune response involving interleukin-4 (IL-4), IL-13, and IL-5, whereas the chronic phase is characterized by a broader immune activation, including elevated levels of IL-6, IL-1β, tumour necrosis factor alpha (TNF-α), and interferon gamma (IFN-γ) (22, 23). Although findings are mixed, studies report increased levels of IL-6, IL-1β, and TNF-α in individuals with psychiatric diseases such as depression (24). In cases of moderate-to-severe AD with frequent or intense flares, levels of these pro-inflammatory cytokines are even further elevated (25). Moreover, the risk of psychological stress, worries, and insomnia increases. Therefore, the link between AD and mental health appears to be multifaceted, involving both physiological and psychological mechanisms.
HADS is a widely used instrument to quantify anxiety and depression in patients with skin disease (26–28). It was originally developed for hospitalized physically ill outpatients but a recent updated literature study found that HADS performed well for somatic, psychiatric, and primary care patients, and in the general population (16, 29). One study compared AD patients with controls, and found mean anxiety scores of 7.7 vs 5.6 and depression scores of 6.0 vs 4.3 for the AD patients and controls, respectively (30). In comparison, most patients in this study scored within the normal range of both anxiety and depression, with the unstable severe group having a median (IQR) anxiety score of 7 (4–10).
Flares and relapses were considered when AD features were first described and diagnostic criteria were developed (7), but have never been used in a standardized measure of stability in the disease course. “Time to first flare” is the most common end-point related to flaring in randomized controlled trials, but lacks information on long-term control (31). Previously, several definitions have been used for flares and disease stability in research and these often favour healthcare providers’ clinical perspective (32–34). Recent studies suggest that existing published definitions of AD flares do not fully reflect patients’ lived experiences (35, 36). Focus-group discussions have highlighted key elements for a patient-centred definition of a flare, notably changes from a patient’s usual baseline; mental, emotional, and social impacts; physical alterations in the skin; perceived control or loss of control; and overall quality of life (35). Furthermore, a larger survey found the highest level of agreement among patients in defining a flare as “when my symptoms take significantly more of my attention than normal” and “a worsening of physical symptoms associated with AD”, with “acute worsening of symptoms of AD” rated as the most important (36). In the current study, we rather chose a concrete definition of a flare to enable quantification of the number of flares, and to avoid overestimation. However, some degree of underestimation is plausible, as more interpretive definitions might have captured a broader range of patient experiences. In future studies, the purpose of flare-related questions should be carefully considered: is the aim to identify the most severely affected patients, or to capture a more comprehensive picture of how many patients experience some level of worsening in their eczema? Incorporating the patient’s subjective experience may offer a more reality-based understanding of flares and their impact in everyday life.
In addition, new methods are being developed to obtain robust and accurate measures of disease control. A relatively new instrument, the Recap of Atopic Eczema (RECAP), is a 7-item questionnaire designed to capture the experience of eczema control in all ages and eczema severities, and provides a standardized measure of eczema control perceived by the patient. RECAP has the potential to improve reporting of eczema control in research and could be considered in future studies within this area (37).
Within guidelines, the moderate and severe groups of AD patients are often combined into a “moderate-to-severe” group. It has been demonstrated that only a minority of moderate-to-severe AD patients who are eligible for a systemic treatment receive such therapy (38). Patients with moderate-to-severe AD often report a substantial disease burden, particularly with regard to underuse of systemic treatments despite the fact that AD is a systemic disease (39). Knowledge of a stable and unstable disease course within the moderate severity group could emphasize the contribution of flaring in treatment decisions. In this study, the median PO-SCORAD for cluster 4 with persistent flaring was consistent with moderate disease. Consequently, patients with moderate disease but severe flaring may be at risk of undertreatment, especially with systemic therapies, unless the flaring is prioritized in treatment decisions. Conversely, moderate-to-severe disease was most often accompanied by a large number of annual flares, thereby implying that persistent flaring may be considered a common feature of severe AD.
Interestingly, an increase was observed in DLQI for most clusters from 2020 to 2022. It can be speculated whether this is related to factors beyond AD, for instance a remnant of COVID-19 in 2020/2021.
Strengths and limitations
An important strength of the DSC is that all patients included had a dermatologist-verified AD diagnosis and patients across the entire country were invited to participate, thereby minimizing the risk of selection bias. Another strength of the machine-learning models was that no assumption was made regarding the number of clusters or the distributions and characteristics of these clusters.
Recall bias of flares was reduced by requiring the patients to remember only 12 months back. However, patient-reported outcomes (PROs) should generally be used with caution, as we have previously demonstrated that patients with AD had a poor recollection even of having had AD (40). Furthermore, only patients with complete data on number of flares and PO-SCORAD were included, leading to a smaller total number of AD patients, especially in subgroups, thereby resulting in less statistical power to identify differences. Moreover, the definition of flares could be elaborated, as the current study is limited by defining flares solely in terms of skin symptoms, while patient perception also includes significant emotional and quality-of-life impacts.
It may be interesting to consider flare severity and duration in future analyses, but we found it to be out of scope for this study.
Conclusion
Stability in AD disease courses is crucial due to its association with better mental health, measured by lower levels of anxiety compared with an unstable disease course. An unstable disease trajectory was common among patients with moderate-to-severe disease, implying the need for an increased focus on this large group. Long-term stability of AD and flare patterns should be considered by the physician in the assessment of severity and treatment decisions.
ACKNOWLEDGEMENTS
IRB approval status: All participants gave written informed consent and allowed processing of personal information. This constitutes the necessary legal requirements, and ethical approval is not required for this type of study in Denmark.
REFERENCES
- Garmhausen D, Hagemann T, Bieber T, Dimitriou I, Fimmers R, Diepgen T, et al. Characterization of different courses of atopic dermatitis in adolescent and adult patients. Allergy Eur J Allergy Clin Immunol 2013; 68: 498–506. https://doi.org/10.1111/all.12112
- Bao Q, Chen L, Lu Z, Ma Y, Guo L, Zhang S, et al. Association between eczema and risk of depression: A systematic review and meta-analysis of 188,495 participants. J Affect Disord 2018; 238: 458–464. https://doi.org/10.1016/j.jad.2018.05.007
- Yaghmaie P, Koudelka CW, Simpson EL. Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol 2013; 131: 428–433. https://doi.org/10.1016/j.jaci.2012.10.041
- Thyssen JP, Hamann CR, Linneberg A, Dantoft TM, Skov L, Gislason GH, et al. Atopic dermatitis is associated with anxiety, depression, and suicidal ideation, but not with psychiatric hospitalization or suicide. Allergy Eur J Allergy Clin Immunol 2018; 73: 214–220. https://doi.org/10.1111/all.13231
- Vittrup I, Andersen YMF, Droitcourt C, Skov L, Egeberg A, Fenton MC, et al. Association between hospital-diagnosed atopic dermatitis and psychiatric disorders and medication use in childhood. Br J Dermatol 2021; 185: 91–100. https://doi.org/10.1111/bjd.19817
- Rønnstad ATM, Halling-Overgaard AS, Hamann CR, Skov L, Egeberg A, Thyssen JP. Association of atopic dermatitis with depression, anxiety, and suicidal ideation in children and adults: a systematic review and meta-analysis. J Am Acad Dermatol 2018; 79: 448-456.e30. https://doi.org/10.1016/j.jaad.2018.03.017
- Hanifin JM, Rajka G. Diagnostic features of AD. Acta Derm Venereol 1980; Suppl 92: 44–47.
- Williams HC, Burney PG, Pembroke AC, Hay RJ. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol 1994; 131: 406–416. https://doi.org/10.1111/j.1365-2133.1994.tb08532.x
- Larsen FS, Diepgen T, Svensson Å. The occurrence of atopic dermatitis in North Europe: an international questionnaire study. J Am Acad Dermatol 1996; 34: 760–764. https://doi.org/10.1016/S0190-9622(96)90009-2
- Williams H, Robertson C, Stewart A, Aït-Khaled N, Anabwani G, Anderson R, et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the international study of asthma and allergies in childhood. J Allergy Clin Immunol 1999; 103: 125–138. https://doi.org/10.1016/S0091-6749(99)70536-1
- Nymand L, Nielsen M-L, Vittrup I, Halling A-S, Francis Thomsen S, Egeberg A, et al. Atopic dermatitis phenotypes based on cluster analysis of the Danish Skin Cohort. Br J Dermatol 2024; 190: 207–215. https://doi.org/10.1093/bjd/ljad401
- Zuberbier T, Orlow SJ, Paller AS, Taïeb A, Allen R, Hernanz-Hermosa JM, et al. Patient perspectives on the management of atopic dermatitis. J Allergy Clin Immunol 2006; 118: 226–232. https://doi.org/10.1016/j.jaci.2006.02.031
- Egeberg A, Andersen YMF, Thyssen JP. Prevalence and characteristics of psoriasis in Denmark: findings from the Danish skin cohort. BMJ Open 2019; 9: 1–7. https://doi.org/10.1136/bmjopen-2018-028116
- Wollenberg A, Christen-Zäch S, Taieb A, Paul C, Thyssen JP, de Bruin-Weller M, et al. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol 2020; 34: 2717–2744. https://doi.org/10.1111/jdv.16892
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67: 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform 2019; 95: 103208. https://doi.org/10.1016/j.jbi.2019.103208
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap): a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42: 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
- Petitjean F, Ketterlin A, Gançarski P. A global averaging method for dynamic time warping, with applications to clustering. Pattern Recognit 2011; 44: 678–693. https://doi.org/https://doi.org/10.1016/j.patcog.2010.09.013
- Rousseeuw PJ. Silhouettes: a graphical aid to the interpretation and validation of cluster analysis. J Comput Appl Math 1987; 20: 53–65. https://doi.org/10.1016/0377-0427(87)90125-7
- Tavenard R, Faouzi J, Vandewiele G, Divo F, Androz G, Holtz C, et al. Tslearn, a machine learning toolkit for time series data. J Mach Learn Res 2020; 21: 1–6.
- Santamaria-Babí LF. Atopic dermatitis pathogenesis: lessons from immunology. Dermatol Pract Concept 2022; 12: e2022152. https://doi.org/10.5826/dpc.1201a152
- Fania L, Moretta G, Antonelli F, Scala E, Abeni D, Albanesi C, et al. Multiple roles for cytokines in atopic dermatitis: from pathogenic mediators to endotype-specific biomarkers to therapeutic targets. Int J Mol Sci 2022; 23. https://doi.org/10.3390/ijms23052684
- Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry 2010; 67: 446–457. https://doi.org/10.1016/j.biopsych.2009.09.033
- Savva M, Papadopoulos NG, Gregoriou S, Katsarou S, Papapostolou N, Makris M, et al. Recent advancements in the atopic dermatitis mechanism. Front Biosci (Landmark Ed) 2024; 29: 84. https://doi.org/10.31083/j.fbl2902084
- Dalgard FJ, Gieler U, Tomas-Aragones L, Lien L, Poot F, Jemec GBE, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol 2015; 135: 984–991. https://doi.org/10.1038/jid.2014.530
- Marron SE, Tomas-Aragones L, Navarro-Lopez J, Gieler U, Kupfer J, Dalgard FJ, et al. The psychosocial burden of hand eczema: data from a European dermatological multicentre study. Contact Dermatitis 2018; 78: 406–412. https://doi.org/10.1111/cod.12973
- Brenaut E, Halvorsen JA, Dalgard FJ, Lien L, Balieva F, Sampogna F, et al. The self-assessed psychological comorbidities of prurigo in European patients: a multicentre study in 13 countries. J Eur Acad Dermatol Venereol 2019; 33: 157–162. https://doi.org/10.1111/jdv.15145
- Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale: an updated literature review. J Psychosom Res 2002; 52: 69–77. https://doi.org/10.1016/s0022-3999(01)00296-3
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Symptoms and diagnosis of anxiety and depression in atopic dermatitis in U.S. adults. Br J Dermatol 2019; 181: 554–565. https://doi.org/10.1111/bjd.17683
- Barbarot S, Rogers NK, Abuabara K, Aubert H, Chalmers J, Flohr C, et al. Strategies used for measuring long-term control in atopic dermatitis trials: a systematic review. J Am Acad Dermatol 2016; 75: 1038–1044. https://doi.org/10.1016/j.jaad.2016.05.043
- Langan SM, Thomas KS, Williams HC. What is meant by a “flare” in atopic dermatitis? Arch Dermatol 2006; 142: 1190–1196. https://doi.org/10.1001/archderm.142.9.1190
- Langan SM, Schmitt J, Williams HC, Smith S, Thomas KS. How are eczema ‘flares’ defined? A systematic review and recommendation for future studies. Br J Dermatol 2014; 170: 548–556. https://doi.org/10.1111/bjd.12747
- Nielsen M-L, Nymand LK, Domenech Pena A, Du Jardin KG, Kasujee I, Thomsen SF, et al. Characterization of patients with atopic dermatitis based on flare patterns and severity of disease: a Danish population-based study. J Eur Acad Dermatol Venereol 2025; 39: 301–307. https://doi.org/10.1111/jdv.20160
- Dainty KN, Thibau IJC, Amog K, Drucker AM, Wyke M, Begolka WS. Towards a patient-centred definition for atopic dermatitis flare: a qualitative study of adults with atopic dermatitis. Br J Dermatol 2024; 191: 82–91. https://doi.org/10.1093/bjd/ljae037
- Drucker AM, Thibau IJC, Mantell B, Dainty KN, Wyke M, Smith Begolka W. Consensus on a patient-centered definition of atopic dermatitis flare. JAMA Dermatol 2024; 160: 1099–1106. https://doi.org/10.1001/jamadermatol.2024.054
- Howells LM, Chalmers JR, Gran S, Ahmed A, Apfelbacher C, Burton T, et al. Development and initial testing of a new instrument to measure the experience of eczema control in adults and children: Recap of atopic eczema (RECAP). Br J Dermatol 2020; 183: 524–536. https://doi.org/10.1111/bjd.18780
- Pascal C, Maucort-Boulch D, Gilibert S, Bottigioli D, Verdu V, Jaulent C, et al. Therapeutic management of adults with atopic dermatitis: comparison with psoriasis and chronic urticaria. J Eur Acad Dermatol Venereol 2020; 34: 2339–2345. https://doi.org/10.1111/jdv.16329
- Kleyn CE, Barbarot S, Reed C, Losi S, von Arx LB, Robert C, et al. Burden of moderate to severe atopic dermatitis in adults from France, Italy, and the UK: patient-reported outcomes and treatment patterns. Dermatol Ther (Heidelb) 2022; 12: 1947–1965. https://doi.org/10.1007/s13555-022-00777-z
- Nymand LK, Andersen YMF, Thyssen JP, Egeberg A. Limitations of using questionnaires for assessing the prevalence of psoriasis and atopic dermatitis among adults. JAMA Dermatol 2021; 157: 971–977. https://doi.org/10.1001/jamadermatol.2021.2307