SHORT COMMUNICATION
Subtotal Scrotectomy and Scrotoplasty: An Effective Treatment for Idiopathic Scrotal Calcinosis
Ricardo MORENO-BORQUE  1, Carmen CARRANZA-ROMERO1, Ana SIRGADO-MARTÍNEZ1, Elena LOZANO-MARTÍNEZ1 and Eduardo LÓPEZ-BRAN2
1, Carmen CARRANZA-ROMERO1, Ana SIRGADO-MARTÍNEZ1, Elena LOZANO-MARTÍNEZ1 and Eduardo LÓPEZ-BRAN2
1Dermatology Department, Hospital Clínico San Carlos, Madrid, Spain, and 2Dermatology Department, Hospital Clínico San Carlos; IdISSC, Madrid, Spain. E-mail: rmorenoborque@gmail.com
Citation: Acta Derm Venereol 2025; 105: adv43100. DOI: https://doi.org/10.2340/actadv.v105.43100.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 4, 2025. Accepted after revision: Apr 16, 2025. Published: May 13, 2025
Competing interests and funding: The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given his consent for his images and clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
INTRODUCTION
First described by Lewinski in 1883 as a subtype of calcinosis cutis (1), idiopathic scrotal calcinosis (ISC) is a rare, benign dermatological condition characterized by multiple intradermal calcified nodules within the scrotum that occur with normal calcium and phosphate metabolism. These nodules tend to affect the anterior scrotum, clustering around the midline raphe (2). The scrotal wall is composed, from superficial to deep, by rugated skin, superficial fascia (Dartos), external spermatic fascia, cremasteric muscle, and the internal spermatic fascia (3).
Various pathogenetic mechanisms have been postulated to explain these nodules. There is evidence that dystrophic calcification of pre-existing epidermal cysts can represent an initiating event in the pathogenesis of the disease in some cases (4), but no consensus has been reached concerning the aetiology of ISC. Histologically, ISC is characterized by the presence of amorphous basophilic calcium deposits, within the dermis, surrounded by a granulomatous inflammatory reaction composed predominantly of macrophages, multinucleated giant cells, and lymphocytes (5).
Although generally asymptomatic, the nodules may cause itching, undergo ulceration, or develop secondary infection. Extensive scrotal involvement has been linked to an excess of anterior scrotal skin, which can manifest as discomfort during activities such as walking, wearing loose clothes, practising sports, or during sexual intercourse. It is related to aesthetic concerns in affected individuals because of the appearance of their genitalia, leading to psychological issues such as embarrassment, anxiety, or low self-esteem. Assessment tools such as the Dermatology Life Quality Index (DLQI) provide a standardized and validated method to quantify the impact of various dermatological conditions on patients’ quality of life. These instruments facilitate the evaluation of the psychosocial benefits associated with different therapeutic interventions (6).
Therapeutic approaches are primarily aimed at alleviating symptoms. If minimal in number, nodules may be treated conservatively, or can be individually excised. Individual nodule excision is not a feasible approach in cases involving multiple lesions, as it is time-consuming and may result in numerous scars with a poor cosmetic outcome. Partial scrotectomy, a surgical technique involving the excision of affected scrotal tissue, has emerged as a promising intervention. In most scrotectomies, primary closure scrotoplasty is sufficient to repair the excised area. However, in more extensive cases, the post-excisional defect might require the use of skin flaps or grafts (7, 8).
We present the diagnostic and therapeutic outcomes of a case of ISC and provide a review of the current literature on surgical options and techniques.
CASE REPORT
We present the case of a 33-year-old male patient with a medical history notable only for segmental vitiligo, for which he was not undergoing any treatment, who consulted for an aesthetic concern regarding his genitalia. Upon scrotal examination we found multiple firm nodules, predominantly affecting the anterior wall, with noticeable scrotal laxity (Fig. 1A and Fig. 2A). Occasional nodules outside of this region were also found. His serum calcium, phosphorus, and PTH levels were within normal limits. The patient was clinically diagnosed with ISC and scheduled for surgical treatment involving subtotal scrotectomy and scrotoplasty.
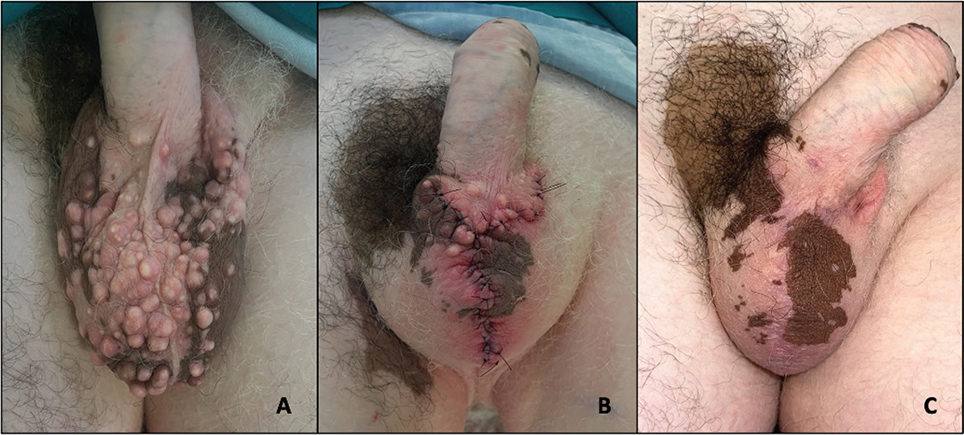
Fig. 1. (A) Preoperative appearance of a 33-year-old male with scrotal calcinosis and increased scrotal laxity. (B) Postoperative result after wound closure. (C) Scrotal appearance at 12-month postoperative follow-up.

Fig. 2. (A) Excess and lax anterior scrotal skin containing multiple calcified nodules. (B) Post-excisional scrotal calcinosis specimen. (C) Immediate postoperative appearance after anterior scrotectomy.
The procedure was performed under local anaesthesia using bupivacaine without adrenaline, which was administered via a spermatic cord block and along the median raphe. Bupivacaine was chosen instead of more conventional options, such as lidocaine or mepivacaine, due to its longer half-life. As scrotectomy and scrotoplasty are lengthy procedures, the use of bupivacaine helped provide a prolonged effect, reducing the need for repeated administrations of local anaesthesia during the intervention. The objective of employing local anaesthesia was to significantly reduce the duration of both the surgical procedure and the recovery period, thereby improving overall surgical efficiency and accessibility (9).
We undertook a triangular resection of the excess scrotal skin along the ventral median raphe (Fig. 2B). The amount of skin and Dartos fascia excised was determined by the degree of scrotal involvement, leaving an extensive defect of the scrotum (Fig. 2C). An A–T flap was conducted for an anatomic reconstruction of the defect, using posterolateral skin of the scrotum to cover the testes. Closure was performed using 4/0 polyglactin (Vicryl plus) resorbable sutures for the Dartos fascia and 4/0 Ethilon non-absorbable sutures for the scrotal skin (Fig. 1B). The patient’s tolerance was good, and there were no intraoperative complications. The histopathological findings of the specimen were compatible with ISC.
The patient was discharged the same day and recovered uneventfully. He was scheduled for a postoperative evaluation 4 weeks after surgery, at which time complete healing was observed without complications. Three months after the initial surgical procedure, a secondary operation was undertaken to excise the residual nodules that were located beyond the boundaries of the initial resection. On follow-up at 12 months, the patient expressed significant satisfaction with the aesthetic outcome of his genitalia and reported normal sensitivity of the scrotum, with no evidence of ISC recurrence (Fig. 1C).
A DLQI assessment was conducted both preoperatively and postoperatively to evaluate the impact of the surgical intervention on the patient’s quality of life. The preoperative DLQI score was 19, reflecting a significant impact on the patient’s quality of life. Postoperatively, the DLQI score decreased to 2, reflecting only a minor effect on the patient’s daily life, primarily due to residual itching.
DISCUSSION
ISC is a rare and benign disease that presents with multiple, brownish-yellow calcified nodules on the scrotum, which appears mainly in childhood or early adulthood. This disorder usually has an indolent course, developing over years. The diagnosis is clinical and may be confirmed through histopathological analysis.
Surgery is indicated when the disease interferes with activities of daily living or when certain conditions, such as recurrent infection, ulceration, or questionable malignancy, are present (10).
Scrotoplasty involves the surgical removal of calcified nodules in the scrotum, addressing both aesthetic and symptomatic concerns. The rationale behind scrotoplasty lies in providing a definitive treatment option for ISC, aiming to improve patient outcomes and quality of life (4). Scrotoplasty incisions typically close primarily, but in large scrotal skin defects the reconstructive choices include the use of skin grafts, skin flaps, musculocutaneous flaps, and tissue expansion (11).
Although scrotectomy and scrotoplasty are generally regarded as safe and technically straightforward procedures, they are not without potential risks and complications. Documented adverse outcomes include infections, seromas, haematomas, sensory disturbances (loss of sensation, hypersensitivity, and chronic pain), and scar-related symptoms (hypertrophic scarring, “dog-ear” skin tags, contractures, wound dehiscence, and asymmetry) (2–4).
Limited studies and case reports exist, suggesting favourable outcomes following scrotoplasty for ISC. Reduction in symptomatology, resolution of cosmetic concerns, and low recurrence rates have been reported, supporting the efficacy of this surgical intervention (12). In our case, the surgical treatment yielded satisfactory results and no postoperative complications were observed. The DLQI was employed both preoperatively and postoperatively to assess the impact of the surgery on the patient’s quality of life objectively, demonstrating a significant improvement in the overall score. This approach underscores the importance of evaluating not only the clinical outcomes but also the psychosocial benefits afforded by the treatment (4).
Multiple scrotal resection patterns have been proposed in the context of scrotal calcinosis, the election of which is determined by the area of skin affected (12). We believe that a vertical skin resection pattern should be the preferred surgical option, because it restores the scrotum in a more anatomical way, by placing the scar in the median raphe. This also allows better preservation of scrotal sensitivity, as the genital branch of the genitofemoral nerve and the ilioinguinal nerves run from lateral to medial (13).
Following the excision of the affected scrotum, recurrence of lesions is rare. This surgical approach thus represents a potentially curative intervention, with excellent cosmetic outcomes (14). The A–T flap was the preferred surgical option in our patient, but the choice of scrotoplasty technique should be determined based on the surgeon’s expertise and familiarity with the procedure.
As it is a dermatological condition, we believe it is essential for dermatologists to be well acquainted with the surgical options available for the treatment of ISC. Scrotoplasty surgical techniques still remain poorly addressed entities in the current scientific literature, with no comparative studies currently available. Further research and more reported experiences are needed in order to develop therapeutical guidelines.
The authors have no conflicts of interest to declare.
REFERENCES
- Akosa AB, Gilliland EA, Ali MH, Khoo CT. Idiopathic scrotal calcinosis: a possible aetiology reaffirmed. Br J Plast Surg 1989; 42: 324–327. https://doi.org/10.1016/0007-1226(89)90155-0
- King DT, Brosman S, Hirose FM, Gillespie LM. Idiopathic calcinosis of scrotum. Urology 1979; 14: 92–94. https://doi.org/10.1016/0090-4295(79)90225-5
- Shishido S, Natsume O. [Scrotoplasty]. Geka Chiryo 1967; 16: 347–352 (in Japanese).
- Solanki A, Narang S, Kathpalia R, Goel A. Scrotal calcinosis: pathogenetic link with epidermal cyst. BMJ Case Rep 2015; 2015: bcr2015211163. https://doi.org/10.1136/bcr-2015-211163
- Song DH, Lee KH, Kang WH. Idiopathic calcinosis of the scrotum: histopathologic observations of fifty-one nodules. J Am Acad Dermatol 1988; 19: 1095–1101. https://doi.org/10.1016/S0190-9622(88)70278-9
- da Silva N, Augustin M, Langenbruch A, Mrowietz U, Reich K, Thaçi D, et al. Disease burden and treatment needs of patients with psoriasis in sexually-sensitive and visible body areas: results from a large-scale survey in routine care. Eur J Dermatol 2020; 30: 267–278. https://doi.org/10.1684/ejd.2020.3768
- Karaca M, Taylan G, Akan M, Eker G, Gideroglu K, Gul AE. Idiopathic scrotal calcinosis: surgical treatment and histopathologic evaluation of etiology. Urology 2010; 76: 1493–1495. https://doi.org/10.1016/j.urology.2010.02.001
- Thomas C, Navia A. Aesthetic scrotoplasty: systematic review and a proposed treatment algorithm for the management of bothersome scrotum in adults. Aesthetic Plast Surg 2021; 45: 769–776. https://doi.org/10.1007/s00266-020-01998-3
- Bal DS, Chung D, Urichuk M, Shah J, Fidel MG, Panchendrabose K, et al. Utilizing local anesthesia only for penile and scrotal urologic surgery: a prospective study on patient tolerability and surgical outcomes for a sedation-free option. Urology 2024; 194: 7–13. https://doi.org/10.1016/j.urology.2024.08.051
- Khallouk A, Yazami OE, Mellas S, Tazi MF, El Fassi J, Farih MH. Idiopathic scrotal calcinosis: a non-elucidated pathogenesis and its surgical treatment. Rev Urol 2011; 13: 95–97.
- Morey AF, Meng MV, McAninch JW. Skin graft reconstruction of chronic genital lymphedema. Urology 1997; 50: 423–426. https://doi.org/10.1016/S0090-4295(97)00259-8
- Hofer MD, Dumanian GA, Felício J, Martins FE. Updates in the management of benign and malignant scrotal conditions: issues on surgical ablation and reconstruction. AME Med J 2020; 5: 27–27. https://doi.org/10.21037/amj.2020.03.08
- Liguori G, Ollandini G, Napoli R. Anatomy of the scrotum. In: Bertolotto M, Trombetta C, editors. Scrotal pathology. Heidelberg: Springer, 2012: p. 27–34. https://doi.org/10.1007/174_2011_170
- Deverill SJ, Menzies-Wilson R, Rees RW. Point of technique: Limited anterior scrotectomy and scrotoplasty for multiple epidermoid cysts of the scrotum. J Clin Urol 2020; 14: 306–309. https://doi.org/10.1177/2051415820927820