ORIGINAL REPORT
Bidirectional Relationship Between Atopic Dermatitis and Psychiatric Comorbidities in Individuals of European Ancestry: A Mendelian Randomization Study
Zhe WU1–3#, Chenglong WU1–3#, Xuanyi CHEN1–3#, Qiufang QIAN4 and Zhirong YAO1–3
1Dermatology Center, Xinhua Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, 2Department of Dermatology, Xinhua Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, 3Institute of Dermatology, Shanghai Jiaotong University School of Medicine, Shanghai, and 4Department of Dermatology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
#These authors contributed equally to this work.
Atopic dermatitis is a chronic inflammatory skin disorder that significantly impacts quality of life and is often associated with psychiatric comorbidities. How-ever, the causal relationship between atopic dermatitis and psychiatric disorders remains unclear. This study employed bidirectional 2-sample Mendelian randomization to investigate the potential causal relationships between atopic dermatitis and 8 psychiatric conditions: depression, anxiety, autism spectrum disorder, attention deficit hyperactivity disorder, suicidality, bipolar disorder, obsessive-compulsive disorder, and schizophrenia. Genetic instruments were derived from large-scale genome-wide association studies of European ancestry. Forward Mendelian randomization analysis indicated that atopic dermatitis causally increases the risk of anxiety (inverse variance weighting p = 0.016; odds ratio = 1.110, 95% confidence interval: 1.019–1.208). Reverse Mendelian randomization analysis revealed a significant causal effect of bipolar disorder on increasing the risk of atopic dermatitis (inverse variance weighting p = 0.005; odds ratio = 1.062, 95% confidence interval: 1.018–1.107). No significant causal relationships were found for other psychiatric conditions. Sensitivity analyses confirmed the robustness of these findings, with no evidence of horizontal pleiotropy. These results highlight the need for integrated dermatological and psychiatric care, emphasizing early mental health screening for atopic dermatitis patients and dermatological evaluation for individuals with bipolar disorder. Future research should explore underlying biological mechanisms and validate findings across diverse populations.
SIGNIFICANCE
Atopic dermatitis is a common skin condition that significantly affects quality of life. Many people with atopic dermatitis also experience psychiatric disorders, such as anxiety and bipolar disorder, but whether atopic dermatitis causes these conditions or vice versa remains unclear. Using genetic data, our study found that atopic dermatitis increases the risk of anxiety, while bipolar disorder increases the risk of atopic dermatitis. These findings highlight the need for integrated care that addresses both skin and mental health. Understanding these connections may lead to better prevention and treatment strategies, improving overall patient well-being.
Key words: causal relationship; atopic dermatitis; psychiatric comorbidity; Mendelian randomization.
Citation: Acta Derm Venereol 2025; 105: adv43133. DOI: https://doi.org/10.2340/actadv.v105.43133.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
Submitted: Feb 10, 2025; Accepted after revision: Feb 10, 2025. Published: May 15, 2025
Corr: Qiufang Qian, MS, Department of Dermatology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, 355 Luding Road, Putuo District, Shanghai 200062, China, and Zhirong Yao, MD, Dermatology Center, Xinhua Hospital, Shanghai Jiaotong University School of Medicine, 1665 Kongjiang Road, Yangpu District, Shanghai 200092, China. E-mails: qianqf@shchildren.com.cn; yaozhirong@xinhuamed.com.cn
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) is a chronic, inflammatory skin disorder characterized by recurrent eczematous lesions, intense itching, and an impaired skin barrier (1). It is among the most prevalent dermatological conditions globally, significantly affecting the quality of life of individuals. In the United States, AD prevalence is estimated at approximately 10–15% in children and 7–10% in adults (2). Recent research in China indicates that AD is notably prevalent among both adult and paediatric populations, with prevalence rates of 6.13% in adults, 12.94% in children aged 1–7, and a striking 30.48% in infants (3–5), highlighting the substantial burden of AD across age groups.
The burden of AD goes beyond merely addressing its primary symptoms. Significant physical discomfort, sleep disturbances, and social stigma are common among patients, amplifying the disease’s impact. Additionally, the presence of associated comorbidities, including both medical and psychological issues, exacerbates this burden (6). Among these, the co-occurrence of mental health disorders has gained increasing recognition (7). Commonly observed psychiatric conditions in AD patients include depression, anxiety, autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), suicidality, bipolar disorder (BD), obsessive-compulsive disorder (OCD), and schizophrenia (6, 8, 9). These comorbidities not only complicate AD management but also exert a profound impact on the quality of life for both patients and their families.
The intersection of dermatology and psychiatry is gaining recognition as a critical area of research and clinical focus. Connor provides practitioners’ guidelines on managing the psychological comorbidities of dermatological conditions, highlighting the stigma associated with psychiatric disorders in dermatology and emphasizing their significant impact on both patients and their families (10). Psychiatric comorbidities in AD patients often exacerbate primary dermatological symptoms, creating a vicious circle that aggravates both physical and mental health (11).
Emerging research is shedding light on the potential links between AD and psychiatric comorbidities (PCs). Observational studies indicate associations between AD and various mental health conditions (12–15). However, the causal nature of these relationships remains unclear, primarily due to the limitations of observational studies, including confounding and reverse causation. These methodological challenges necessitate more robust analytical approaches.
Mendelian randomization (MR) represents a robust epidemiological approach that leverages single-nucleotide polymorphisms (SNPs) as instrumental variables to infer causal relationships between exposures and outcomes. By minimizing bias from confounders and addressing reverse causality, MR facilitates the examination of whether AD predisposes individuals to psychiatric comorbidities or vice versa, offering valuable insights into the aetiology of these conditions (16–18)
In this study, we employed a bidirectional 2-sample MR design to investigate the potential causal relationships between AD and PCs. This approach enables an exploration of whether AD contributes to the development of PC or whether PCs, in turn, influence the risk of AD. By elucidating these causal pathways, our findings aim to inform more targeted strategies for the prevention and management of these comorbid conditions.
MATERIALS AND METHODS
Study design description
A bidirectional 2-sample MR analysis was performed using summary statistics from genome-wide association studies (GWAS) to investigate causal associations between AD and PC. In the forward MR analysis, AD was treated as the exposure and PC as the outcome, whereas in the reverse MR analysis, PC served as the exposure and AD as the outcome. The core MR assumptions are as follows: (i) instrumental variables (IVs) are strongly associated with the exposure; (ii) IVs are independent of any confounders; and (iii) IVs affect the outcome only through the exposure and not through any other pathways (Fig. 1). As this study used publicly available summary statistics, ethical approval was not required. The study protocol was not pre-registered in a public repository as the analysis relied entirely on existing GWAS datasets.
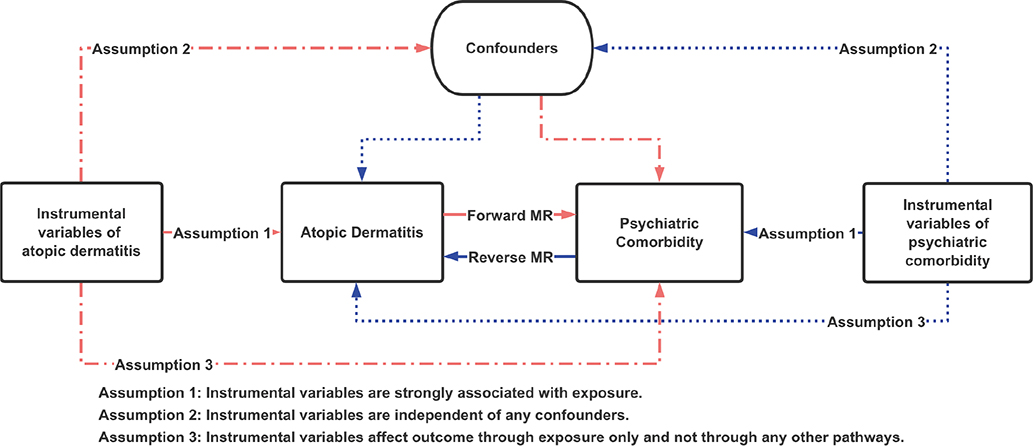
Fig. 1. Bidirectional Mendelian randomization (MR) design. MR analyses require 3 core assumptions. In the forward MR analysis (red arrows), atopic dermatitis (AD) is treated as the exposure and psychiatric comorbidities (PC) as the outcome. In the reverse MR analysis (blue arrows), PC is treated as the exposure and AD as the outcome.
Selection of instrumental variables for MR analyses
For the forward MR analysis, appropriate SNPs for MR were selected from GWAS findings. First, SNPs with genome-wide significance (p < 5 × 10–8) were chosen. Highly correlated variants (r2 > 0.001) within a 10 Mb range were excluded using the clump data approach. SNPs associated with the outcome at p < 5 × 10–8 were then excluded (19).
F-statistics were used to evaluate instrument strength, with weak IVs (defined as F ≤ 10) excluded. The F-value was calculated as follows: F = [(N – k – 1)/k] × [R2/ (1 – R2)] (where “N” is the sample size, “k” is the number of SNPs in IVs, and R2 explains the extent to which IVs correspond to disease) (20). R2 can be calculated as follows: R2 = 2 × (1 – MAF) × MAF × (β/SD) 2 (where “MAF” is the minor allele frequency for each SNP, “β” and “SD” are the coefficient and stand deviation of exposure respectively) (21, 22). The LDtrait Tool (https://ldlink.nih.gov/?tab=ldtrait#ldtrait-tab) was used to exclude SNPs associated with confounding factors (p < 5 × 10–8). During harmonization, palindromic and incompatible SNPs were removed.
For the reverse MR analysis, we assessed reverse causality by performing analyses for ADHD and BD using the same method and parameters (p < 5 × 10–8, linkage disequilibrium r2 < 0.001, clumping distance = 10,000 kb). For other PC, we applied relaxed screening thresholds as follows: depression, anxiety, and ASD (p < 1 × 10–6) or suicidality, OCD, and schizophrenia (p < 5 × 10–6), with linkage disequilibrium r2 < 0.001 and clumping distance = 10,000 kb. The LDtrait Tool was also used to exclude SNPs associated with confounding factors (p < 5 × 10–8), and palindromic and incompatible SNPs were removed during harmonization. The application of relaxed thresholds for these specific psychiatric outcomes aimed to retain a sufficient number of instrumental variables, thereby optimizing the balance between genetic instrument strength and statistical power in the Mendelian randomization framework.
Data sources and instrumental variables selection for AD
The largest AD GWAS data from a European meta-analysis of 40 cohorts was used, consisting of 60,653 cases and 804,329 controls (23) (Table I). A total of 62 SNPs associated with AD were initially identified. (Table SI). Among these, 14 SNPs with F < 10 were excluded, along with 21 SNPs associated with confounders (e.g., body mass index, asthma, 25-hydroxyvitamin D levels; Table SII). Thus, 27 variants were finally included as IVs in the forward MR analysis (Table SIII).
Data sources and instrumental variables selection for PC
Eight kinds of PC were selected for MR analysis: depression (finn-b-F5_DEPRESSIO), anxiety (finn-b-KRA_PSY_ANXIETY), ASD (ieu-a-1185), ADHD (ieu-a-1183), suicidality (finn-b-VWXY20_SUICI_OTHER_INTENTI_SELF_H), BD (ieu-b-5110), OCD (ieu-a-1189), and schizophrenia (finn-b-F5_SCHZPHR). Data for PC were obtained from the IEU OpenGWAS project (https://gwas.mrcieu.ac.uk/), originating from the FinnGen and PGC Consortium databases. Sample sizes for these disorders ranged from 33,925 to 352,006 individuals of European ancestry (Table I). There was no participant overlap between AD and PC cohorts. The number of IVs selected for reverse MR analyses ranged from 8 to 37.
Statistical analysis
Inverse variance weighting (IVW) was used as the primary approach for MR analysis, with MR-Egger, weighted median, simple mode, and weighted mode used as sensitivity analyses. Cochran’s Q test was employed to assess SNP heterogeneity. MR-Egger regression was utilized to detect and correct for directional pleiotropy, interpreting the intercept as an estimate of the average pleiotropic effect across genetic variants (24). The Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO) test was conducted to identify horizontal pleiotropic outliers in multi-instrument summary-level MR analysis (25). Stability of results was verified using the “Leave-one-out” method. SNPs showing heterogeneity or pleiotropy or affecting stability were removed prior to the MR analysis. The MR analysis workflow is illustrated in Fig. 2.
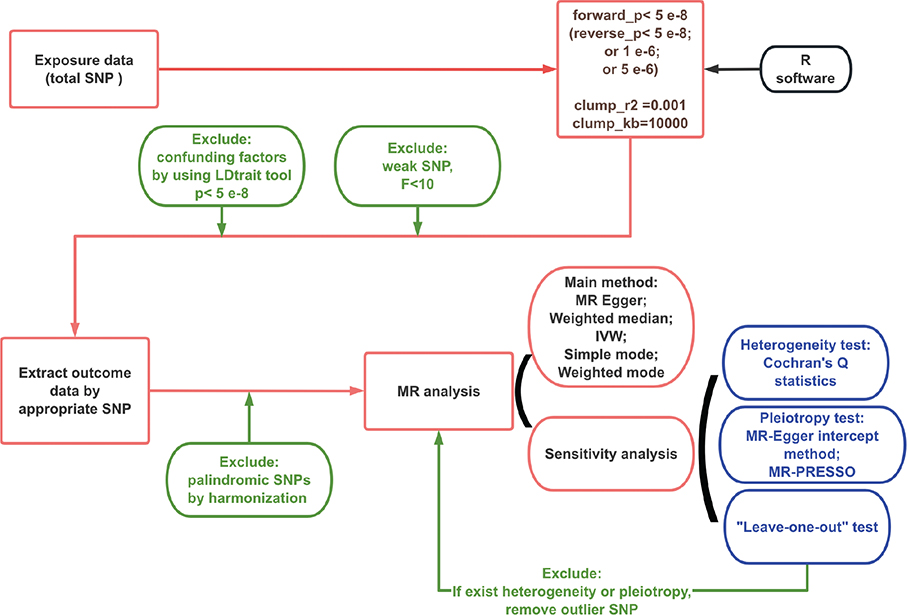
Fig. 2. Mendelian randomization (MR) flowchart. The flowchart outlines the analytical pipeline used in the Mendelian randomization (MR) study. The process begins with selecting exposure data, represented by total SNPs, and follows with quality control measures to exclude confounding factors using the LDtrait tool and SNPs with weak instrumental strength (F < 10). Subsequently, SNPs linked to outcome data are extracted, with harmonization procedures employed to exclude palindromic SNPs. The MR analysis is performed using robust statistical methods, including MR-Egger, weighted median, inverse-variance weighting (IVW), simple mode, and weighted mode. Sensitivity analyses are incorporated to evaluate heterogeneity (Cochran’s Q statistics), pleiotropy (MR-Egger intercept method, MR-PRESSO), and robustness (leave-one-out test). SNPs identified as outliers during these tests are excluded to ensure valid causal inference. The thresholds for forward and reverse analyses are specified, and all analyses are executed using R software.
For binary outcomes, odds ratios (ORs) and 95% confidence intervals (CIs) were used to estimate causal relationships. Causal estimates for both binary and continuous outcomes, including p-values, β coefficients, and standard errors, were reported. All p-values were two-tailed. Analyses were performed using the TwoSampleMR package (version 0.6.8) in R (version 4.4.1) (R Foundation for Statistical Computing, Vienna, Ausutria).
RESULTS
Causal effect of AD on PC
A total of 27 valid single nucleotide polymorphisms (SNPs) were initially included in the forward Mendelian randomization (MR) analysis. Upon extracting ADHD data from the 27 SNPs, data for rs62193132 were missing. For ASD, ADHD, BP, and OCD data from the PGC consortium, the same palindromic SNPs (rs11811788, rs5005507, rs7857407, and rs952558) were excluded.
The p-values of the Cochran’s Q test and the MR-PRESSO global test in the MR analysis of AD on ASD (Q_P = 0.049, MR_PRESSO_P = 0.048) indicated heterogeneity and horizontal pleiotropy among SNPs. After removing the outlier SNP rs10822037, the adjusted Q_P was 0.222, and the adjusted MR_PRESSO_P was 0.252. Furthermore, heterogeneity and pleiotropy tests for the remaining MR analyses showed no significant evidence of heterogeneity among the genetic instruments, reinforcing the reliability of the results.
A forest plot, scatterplot, and “Leave-one-out” test for the causal relationship of AD on PC are provided in Figs S1–3.
A statistically significant association was observed between AD and anxiety (IVW_P = 0.016; OR = 1.110, 95% CI: 1.019–1.208), suggesting that AD may increase the risk of anxiety. No significant associations were found between AD and other psychiatric outcomes, including depression (IVW_P = 0.534; OR = 1.027, 95% CI: 0.945–1.115), ASD (IVW_P = 0.695; OR = 0.855, 95% CI: 0.392–1.867), ADHD (IVW_P = 0.351; OR = 1.227, 95% CI: 0.799–1.884), suicidality (IVW_P = 0.197; OR = 1.042, 95% CI: 0.979–1.109), BD (IVW_P = 0.458; OR = 1.032, 95% CI: 0.950–1.120), OCD (IVW_P = 0.921; OR = 0.984, 95% CI: 0.722–1.342), and schizophrenia (IVW_P = 0.505; OR = 1.101, 95% CI: 0.830–1.459) (Table II).
Causal effect of PC on AD
In the reverse MR analysis, we investigated the potential causal impact of various psychiatric comorbidities on the risk of developing AD. After removing confounder-associated, palindromic, and outlier SNPs, the final SNPs for each disease were used in the reverse MR analysis. Heterogeneity and pleiotropy tests for all reverse MR analyses showed no significant evidence of heterogeneity among the genetic instruments, supporting the robustness and reliability of the results across most outcomes.
A forest plot, scatterplot, and “Leave-one-out” test for the causal relationship of PC on AD are provided in Figs S4–S6.
A statistically significant association was observed between BD and an increased risk of AD (IVW_P = 0.005; OR = 1.062, 95% CI: 1.018–1.107), suggesting that BD may increase the risk of AD. No significant associations were found between other psychiatric outcomes and AD, including depression (IVW_P = 0.649; OR = 1.029, 95% CI: 0.909–1.165), anxiety (IVW_P = 0.460; OR = 1.021, 95% CI: 0.966–1.080), ASD (IVW_P = 0.687; OR = 0.984, 95% CI: 0.912–1.062), ADHD (IVW_P = 0.439; OR = 1.027, 95% CI: 0.959–1.100), suicidality (IVW_P = 0.587; OR = 0.984, 95% CI: 0.928–1.043), OCD (IVW_P = 0.875; OR = 1.002, 95% CI: 0.987–1.026), and schizophrenia (IVW_P = 0.892; OR = 1.002, 95% CI: 0.980–1.024). (Table III).
DISCUSSION
Recent years have seen an increasing number of Mendelian randomization (MR) analyses exploring the relationship between atopic dermatitis (AD) and psychiatric comorbidities (PC). However, significant limitations in these studies warrant attention. Baurecht et al. (26) utilized an earlier AD GWAS dataset (n = 10,788 cases) from 2015, whereas our analysis incorporated updated summary statistics (n = 60,653 cases) with broader population coverage. Differences in sample size and variant selection may influence the precision of causal estimates. Similarly, Cao et al. (27) calculated F-statistics using a formula (F = β²/SE²) that does not account for sample size and allele frequency, whereas we applied the recommended approach (F = [(N – k – 1)/k] × [R²/(1 – R²)]) to ensure accurate assessment of instrument strength. Additionally, their analysis included SNP rs2227491, which is strongly associated with 25-hydroxyvitamin D levels (p = 9 × 10–9) – a potential confounder linked to psychiatric outcomes (28–30). While their findings remain valuable, this SNP’s inclusion raises concerns about horizontal pleiotropy, a key challenge in MR design. To address these limitations, we conducted a bidirectional 2-sample MR analysis, strictly adhering to the 3 core assumptions of MR, to investigate the causal relationships between AD and PC.
The forward MR analysis revealed a statistically significant association between AD and an increased risk of anxiety (IVW_P = 0.016; OR = 1.110, 95% CI: 1.019–1.208), but no significant causal relationships were identified between AD and other psychiatric comorbidities. In the reverse MR analysis, bipolar disorder (BD) was found to causally increase the risk of AD (IVW_P = 0.005; OR = 1.062, 95% CI: 1.018–1.107), while no significant associations were observed for other psychiatric comorbidities. The bidirectional associations observed between AD and anxiety, as well as BD and AD, align with a causal interpretation under MR assumptions. While these findings require replication, they highlight the potential need for multidisciplinary approaches to manage patients with overlapping dermatological and psychiatric conditions.
The central nervous system (CNS) and epidermis both originate from the embryonic neuroectoderm, which may explain the association between skin diseases and neuropsychiatric conditions. However, the mechanisms underlying the relationship between AD and PC remain unclear. Sleep disturbances accompanying AD may predispose children to concurrent mental health conditions, potentially serving as 1 mechanism for this relationship (31). Epidemiological studies indicate that sleep disturbances, particularly insomnia, affect approximately 50% of individuals with anxiety and can exacerbate the condition (32). Similarly, sleep and circadian rhythm disturbances are common and persistent in individuals with bipolar disorder, often occurring between and during episodes of illness (33).
Another potential mechanism linking mental health and AD is the systemic impact of inflammation (31). Keratinocytes play a central role in regulating skin pathology in AD, contributing to skin repair and immune function. Barrier disruption and microbial invasion trigger keratinocytes to produce various cytokines, including IL-6, IL-23, TARC/CCL17, and TNF-α, which promote inflammation by recruiting and activating immune cells (34). Studies have demonstrated that elevated levels of IL-6 and TNF-α in the plasma and central nervous system are associated with anxiety and may exacerbate mental health disorders (35–37).
The significant bidirectional relationships identified in this study have important clinical implications. Given the increased anxiety risk associated with AD, clinicians should consider routine mental health screening, particularly in adults and patients with severe or persistent AD symptoms, balancing clinical utility and resource constraints. Similarly, the causal effect of BD on AD suggests that effective management of psychiatric conditions may play a role in reducing dermatological burden. These insights advocate for a multidisciplinary approach to the care of patients with comorbid AD and psychiatric comorbidities, involving dermatologists, psychiatrists, and primary care providers.
This study has several limitations that merit careful consideration. First, the reliance on GWAS datasets predominantly comprising individuals of European ancestry restricts the generalizability of our findings to other populations, underscoring the need for validation in ethnically diverse cohorts. Second, although we rigorously excluded SNPs associated with known confounders, residual horizontal pleiotropy may persist due to unmeasured biological pathways, potentially biasing our causal estimates. Third, the use of relaxed significance thresholds (e.g., p < 1 × 10–6) in reverse MR analyses for psychiatric comorbidities such as OCD and schizophrenia may have weakened instrument validity, introducing uncertainty into causal interpretations. Fourth, the reliance on summary-level data precluded subgroup analyses (e.g., by age, sex, or treatment history) and limited our exploration of potential effect modifiers. Moreover, the absence of formal a priori power calculations further undermines confidence in null findings, particularly for outcomes with limited sample sizes like OCD, where true effects might have been missed.
Additionally, the clumping procedure (r² < 0.001, clumping distance = 10,000 kb) employed to select independent genetic instruments may have removed variants in linkage disequilibrium that independently predict the exposure. While this step was necessary to satisfy MR’s assumption of instrument independence, it could exclude SNPs with unique causal contributions to atopic dermatitis or psychiatric traits, potentially underestimating true associations. For example, secondary causal variants in LD regions (e.g., within the FLG gene locus) might have been excluded despite their biological relevance.
Furthermore, bidirectional associations could be confounded by shared pathophysiological mechanisms, such as systemic inflammation or immune dysregulation, which may simultaneously drive both AD and psychiatric comorbidities. The lack of assessment of gene–environment interactions (e.g., stress, pollution) leaves unresolved whether environmental factors modulate these relationships – a critical gap that future studies integrating multi-omics and environmental exposure data should address. Finally, the absence of stratification by AD severity represents a key limitation, as severe AD cases may disproportionately influence mental health risks; consequently, our findings may not extend to individuals with milder phenotypes.
To address these limitations, replication in multi-ethnic cohorts is imperative to enhance generalizability. Longitudinal studies incorporating genetic, environmental, and clinical data (e.g., disease severity, treatment trajectories) are needed to disentangle complex interactions and refine causal inferences. Such efforts would advance translational applications, enabling personalized strategies for managing comorbid AD and psychiatric conditions.
ACKNOWLEDGEMENTS
The authors would like to thank the UK Biobank, PGC, FinnGEN Consortium, GWAS catalogue and OpenGWAS Consortium for providing statistical data.
REFERENCES
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet 2020; 396: 345–360. https://doi.org/10.1016/S0140-6736(20)31286-1
- De Benedetto A, Boguniewicz M, Ong PY, Chu DK, Schneider LC. Atopic dermatitis (eczema) guidelines 2023: Highlights. J Allergy Clin Immunol Pract 2024; 12: 2955–2965. https://doi.org/10.1016/j.jaip.2024.08.052
- Mao D, Li J, Liu S, Liu P, Tian J, Liu X, et al. Prevalence and risk factors of atopic dermatitis in Chinese adults: a nationwide population-based cross-sectional study. Chin Med J (Engl) 2023; 136: 604–606. https://doi.org/10.1097/CM9.0000000000002560
- Guo Y, Li P, Tang J, Han X, Zou X, Xu G, et al. Prevalence of atopic dermatitis in Chinese children aged 1–7 ys. Sci Rep 2016; 6: 29751. https://doi.org/10.1038/srep29751
- Guo Y, Zhang H, Liu Q, Wei F, Tang J, Li P, et al. Phenotypic analysis of atopic dermatitis in children aged 1–12 months: elaboration of novel diagnostic criteria for infants in China and estimation of prevalence. J Eur Acad Dermatol Venereol 2019; 33: 1569–1576. https://doi.org/10.1111/jdv.15618
- Davis DMR, Drucker AM, Alikhan A, Bercovitch L, Cohen DE, Darr JM, et al. American Academy of Dermatology Guidelines: Awareness of comorbidities associated with atopic dermatitis in adults. J Am Acad Dermatol 2022; 86: 1335–1336.e18. https://doi.org/10.1016/j.jaad.2022.01.009
- Cai XC, Wang SH, Wang CX, Liu L, Wang J, Shen YH, et al. Epidemiology of mental health comorbidity in patients with atopic dermatitis: an analysis of global trends from 1998 to 2022. J Eur Acad Dermatol Venereol 2024; 38: 496–512. https://doi.org/10.1111/jdv.19686
- Adesanya EI, Matthewman J, Schonmann Y, Hayes JF, Henderson A, Mathur R, et al. Factors associated with depression, anxiety and severe mental illness among adults with atopic eczema or psoriasis: a systematic review and meta-analysis. Br J Dermatol 2023; 188: 460–470. https://doi.org/10.1093/bjd/ljac132
- Wan J, Wang S, Shin DB, Syed MN, Abuabara K, Lemeshow AR, et al. Neuropsychiatric disorders in adults with atopic dermatitis: a population-based cohort study. J Eur Acad Dermatol Venereol 2024; 38: 543–548. https://doi.org/10.1111/jdv.19518
- Connor CJ. Management of the psychological comorbidities of dermatological conditions: practitioners’ guidelines. Clin Cosmet Investig Dermatol 2017; 10: 117–132. https://doi.org/10.2147/CCID.S111041
- Rahman SM, Abduelmula A, Jafferany M. Psychopathological symptoms in dermatology: a basic approach toward psychocutaneous disorders. Int J Dermatol 2023; 62: 346–356. https://doi.org/10.1111/ijd.16344
- Tsai SY, Gaffin JM, Hawryluk EB, Ruran HB, Bartnikas LM, Oyoshi MK, et al. Evaluation of dupilumab on the disease burden in children and adolescents with atopic dermatitis: a population-based cohort study. Allergy 2024; 79: 2748–2758. https://doi.org/10.1111/all.16265
- Conway AE, Verdi M, Kartha N, Maddukuri C, Anagnostou A, Abrams EM, et al. Allergic diseases and mental health. J Allergy Clin Immunol Pract 2024; 12: 2298–2309. https://doi.org/10.1016/j.jaip.2024.05.049
- Paller AS, Rangel SM, Chamlin SL, Hajek A, Phan S, Hogeling M, et al. Stigmatization and mental health impact of chronic pediatric skin disorders. JAMA Dermatol 2024; 160: 621–630. https://doi.org/10.1001/jamadermatol.2024.0594
- Johnson JK, Loiselle A, Chatrath S, Smith Begolka W. Patient and caregiver perspectives on the relationship between atopic dermatitis symptoms and mental health. Dermatitis 2024; 35: 386–391. https://doi.org/10.1089/derm.2023.0365
- Davey Smith G, Holmes MV, Davies NM, Ebrahim S. Mendel’s laws, Mendelian randomization and causal inference in observational data: substantive and nomenclatural issues. Eur J Epidemiol 2020; 35: 99–111. https://doi.org/10.1007/s10654-020-00622-7
- Emdin CA, Khera AV, Kathiresan S. Mendelian randomization. JAMA 2017; 318: 1925–1926. https://doi.org/10.1001/jama.2017.17219
- Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ 2018; 362: k601. https://doi.org/10.1136/bmj.k601
- Wang Y, Wang X, Gu X, Pan J, Ouyang Z, Lin W, et al. Evidence for a causal association between psoriasis and psychiatric disorders using a bidirectional Mendelian randomization analysis in up to 902,341 individuals. J Affect Disord 2023; 337: 27–36. https://doi.org/10.1016/j.jad.2023.05.059
- Burgess S, Thompson SG, Collaboration CCG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol 2011; 40: 755–764. https://doi.org/10.1093/ije/dyr036
- Yuan S, Xiong Y, Larsson SC. An atlas on risk factors for multiple sclerosis: a Mendelian randomization study. J Neurol 2021; 268: 114–124. https://doi.org/10.1007/s00415-020-10119-8
- Wu PF, Zhang W, Zhang X, Zhang R. Application and interpretation of Mendelian randomization approaches in exploring the causality between folate and coronary artery disease. Am J Clin Nutr 2020; 111: 1299–1300. https://doi.org/10.1093/ajcn/nqaa069
- Budu-Aggrey A, Kilanowski A, Sobczyk MK, andMe Research T, Shringarpure SS, Mitchell R, et al. European and multi-ancestry genome-wide association meta-analysis of atopic dermatitis highlights importance of systemic immune regulation. Nat Commun 2023; 14: 6172. https://doi.org/10.1038/s41467-023-41180-2
- Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol 2015; 44: 512–525. https://doi.org/10.1093/ije/dyv080
- Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet 2018; 50: 693–698. https://doi.org/10.1038/s41588-018-0099-7
- Baurecht H, Welker C, Baumeister SE, Weidnger S, Meisinger C, Leitzmann MF, et al. Relationship between atopic dermatitis, depression and anxiety: a two-sample Mendelian randomization study. Br J Dermatol 2021; 185: 781–786. https://doi.org/10.1111/bjd.20092
- Cao S, Zhang Z, Liu L, Li Y, Li W, Li Y, et al. Causal relationships between atopic dermatitis and psychiatric disorders: a bidirectional two-sample Mendelian randomization study. BMC Psychiatry 2024; 24: 16. https://doi.org/10.1186/s12888-023-05478-1
- Chen L, Zhu H, Harshfield GA, Treiber FA, Pollock JS, Pollock D, et al. Serum 25-hydroxyvitamin D concentrations are associated with mental health and psychosocial stress in young adults. Nutrients 2020; 12: 1938. https://doi.org/10.3390/nu12071938
- Chu F, Ohinmaa A, Klarenbach S, Wong ZW, Veugelers P. Serum 25-hydroxyvitamin D concentrations and indicators of mental health: an analysis of the Canadian Health Measures Survey. Nutrients 2017; 9: 1116. https://doi.org/10.3390/nu9101116
- Hinata A, Kitamura K, Watanabe Y, Kabasawa K, Saito T, Takahashi A, et al. Low plasma 25-hydroxyvitamin D levels are associated with an increased risk of depressive symptoms in community-dwelling Japanese people aged between 40 and 74 years: the Murakami cohort study. J Affect Disord 2023; 325: 48–54. https://doi.org/10.1016/j.jad.2022.12.104
- Yaghmaie P, Koudelka CW, Simpson EL. Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol 2013; 131: 428–433. https://doi.org/10.1016/j.jaci.2012.10.041
- Chellappa SL, Aeschbach D. Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev 2022; 61: 101583. https://doi.org/10.1016/j.smrv.2021.101583
- Kaplan KA. Sleep and sleep treatments in bipolar disorder. Curr Opin Psychol 2020; 34: 117–122. https://doi.org/10.1016/j.copsyc.2020.02.001
- Yin T, Feng S, Zhu H, Bai R, Gan X, He K, et al. Therapeutic potential of plasma-treated solutions in atopic dermatitis. Free Radic Biol Med 2024; 225: 482–493. https://doi.org/10.1016/j.freeradbiomed.2024.10.290
- Pitsavos C, Panagiotakos DB, Papageorgiou C, Tsetsekou E, Soldatos C, Stefanadis C. Anxiety in relation to inflammation and coagulation markers, among healthy adults: the ATTICA study. Atherosclerosis 2006; 185: 320–326. https://doi.org/10.1016/j.atherosclerosis.2005.06.001
- Maes M, Song C, Lin A, De Jongh R, Van Gastel A, Kenis G, et al. The effects of psychological stress on humans: increased production of pro-inflammatory cytokines and a Th1-like response in stress-induced anxiety. Cytokine 1998; 10: 313–318. https://doi.org/10.1006/cyto.1997.0290
- Arranz L, Guayerbas N, De la Fuente M. Impairment of several immune functions in anxious women. J Psychosom Res 2007; 62: 1–8. https://doi.org/10.1016/j.jpsychores.2006.07.030