REVIEW ARTICLE
Leukotriene Receptor Antagonists for the Treatment of Atopic Dermatitis: A Systematic Review and Meta-analysis
Safa Fawaza MAHMOOD 1, Wafa Nawafa MAHMOOD2*, Omnia Mohamed ABDALLA2, Afra NAZAR2, Hadeeqah Zayaan RIAZ2 and Soha ELMORSY3
1, Wafa Nawafa MAHMOOD2*, Omnia Mohamed ABDALLA2, Afra NAZAR2, Hadeeqah Zayaan RIAZ2 and Soha ELMORSY3
1David Tvildiani Medical University, Tbilisi, Georgia, 2Kasr Al Ainy, Faculty of Medicine, Cairo University, Cairo, and 3Department of Pharmacology, Kasr Al Ainy, Faculty of Medicine, Cairo University, Cairo, Egypt
Atopic dermatitis is a chronic skin condition with no cure. Current conventional treatments can have many side effects or are expensive. Emerging evidence suggests leukotriene receptor antagonists could serve as a corticosteroid-sparing option. This meta-analysis examined 26 studies on the efficacy of leukotriene receptor antagonists for treating atopic dermatitis across 742 participants. There were non-significant reductions in atopic dermatitis severity overall. However, in subgroup analyses montelukast significantly reduced Severity Scoring of Atopic Dermatitis scores in adult populations (SMD = –0.94, 95% CI –1.35 to –0.54, p < 0.0001) and also when compared with conventional treatment rather than placebo (SMD = –0.84, 95% CI –1.21 to –0.47, p < 0.0001). Studies excluded from the statistical analysis generally showed a positive trend favouring montelukast, even if results were not statistically significant. Montelukast shows potential as an adjunct therapy in atopic dermatitis, particularly in adults, but its efficacy is inconsistent. While it may help with pruritus, it should not replace standard treatments. Future research should focus on standardized assessments and personalized approaches to clarify its role in atopic dermatitis management.
SIGNIFICANCE
Our study found that montelukast (a type of medication used for asthma) can be beneficial for patients with eczema as an additional therapy alongside standard therapy like antihistamines, especially in adult patients who have other allergies along with eczema.
Key words: atopic dermatitis; leukotriene receptor antagonists; montelukast.
Citation: Acta Derm Venereol 2025; 105: adv43140. DOI: https://doi.org/10.2340/actadv.v105.43140.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 11, 2025. Accepted after revision: Apr 28, 2025. Published: May 19, 2025.
Corr: Wafa Nawafa Mahmood, Kasr Al Ainy, Faculty of Medicine, Cairo University, Al-Saray Street, El Manial, Cairo 11956, Egypt. E-mail: wafanawafa@gmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) or eczema is a chronic inflammatory skin disease characterized by intense itching, dry skin, and recurrent eczematous lesions. It commonly occurs during early childhood but can affect individuals of any age group. AD is part of the “atopic triad” along with asthma and allergic rhinitis and is often associated with an overactive immune response to environmental allergens and frequently found present together in the same individual (1). The pathophysiology of AD is multifactorial and may involve a combination of genetic predisposition, immune system dysfunction, environmental triggers, and skin barrier defects (2).
There is currently no cure for atopic dermatitis. However, several treatments are used to control it. Conventional treatments for AD primarily include topical therapies such as corticosteroids and calcineurin inhibitors along with emollients and moisturizers. In severe cases, systemic treatments like oral corticosteroids, cyclosporine, or methotrexate may be used (3).
Conventional treatments, namely topical steroids, can have side effects, including skin thinning and adrenal suppression with prolonged use. Systemic immunosuppressive drugs such as cyclosporine carry risks of kidney toxicity and increased infection rates. Biologics and JAK inhibitors, while effective, are costly and may not be suitable for all patients (3).
Leukotriene receptor antagonists (LTRAs), such as montelukast, inhibit leukotrienes (LTs) – inflammatory mediators derived from arachidonic acid – thereby reducing inflammation and allergic responses in conditions like asthma and allergic rhinitis (4). Elevated levels of LTs and proteinoids in chronic inflammatory diseases such as AD indicate their potential role in its pathogenesis (5). Specifically, LTB4 is involved in recruiting neutrophils and Th2 cells related to acute inflammation, while CysLTs contribute to chronic features such as collagen deposition and skin thickening (4). LTs may also increase vascular permeability and promote eosinophil recruitment, further exacerbating skin inflammation (5). Studies have shown that mean urinary LTE4 levels are abnormally elevated and increase consistently with the severity of AD (8). Montelukast was found to be prescribed for off-label use in allergic diseases such as AD (7). In a prescription event monitoring study, some general practitioners reported improvements with montelukast treatment in patients who had a history of longstanding eczema or urticaria (8). While LTRAs are primarily used for asthma, emerging evidence suggests they may also help alleviate AD symptoms, especially in patients with concurrent atopic conditions, although their specific efficacy for AD is still under evaluation (5).
If proven effective and safe, LTRAs could serve as a corticosteroid-sparing option for eczema. Additionally, they may be more cost-effective and accessible compared with newer treatment modalities.
We performed a systematic review to evaluate the safety and efficacy of LTRAs as a potential therapeutic option for atopic dermatitis. Secondary objectives included exploring changes in biological markers associated with AD in patients taking LTRAs and assessing changes in quality of life.
METHODS AND METHODS
This systematic review and meta-analysis were carried out as per the PRISMA Guidelines 2020 (9). Prior to the stage of data extraction, a protocol was registered on PROSPERO (registration number: CRD42024507184).
Literature search
A systematic search was performed in 5 electronic databases: PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Google Scholar, ScienceDirect, and Scopus. Our search included studies published from database inception till May 2024. A search on ClinicalTrials.gov was done to identify any additional studies. Reference lists of the included studies were also manually searched. A general overview of the studies is given in Table SI.
The search was conducted using specific search strings taken from the review question, which were modified according to the specifics of the search engine of each database. The exact strategies used are given in Table SII.
Study selection
Studies that met the following criteria were included in the review:
Inclusion criteria:
- Studies using montelukast or other LTRAs to treat AD.
- Studies involving patients of any age, ethnicity or gender, and having varying severity of AD.
- Randomized controlled trials (RCTs), case series, cohort, quasi-experimental, and case-control studies.
We excluded studies that did not report an analysable outcome, case reports, and articles for which full texts were unavailable despite contacting the authors.
According to the criteria, articles were screened independently by 3 authors (WNM, HZR, and OMA). Disagreements were resolved through discussion and if continued discourse occurred, a senior researcher (SFM) was involved to reach a consensus on the final decision for inclusion.
Data extraction
Data from eligible studies were extracted independently by 3 authors (WNM, AN, and SFM). A standardized data extraction sheet developed for the study was used. It included the following information: first author, study designs, year of publication, eligibility criteria, participants demographics, interventions, controls used, concomitant therapy, general outcomes, safety outcomes, efficacy results measured either subjectively or by AD severity scoring systems, biological markers measured, effects on quality of life (QoL), and other relevant information. Data from the figure in the study done by Nettis et al. (10) were extracted using WebPlotDigitizer software (Version 5.2; https://automeris.io/). Any disagreement was resolved through discussion among the authors to reach a consensus.
Quality assessment
Quality assessment was conducted independently by 3 authors (WNM, OMA, SFM). Quality of RCTs was assessed using the Cochrane Risk of Bias Tool (RoB-2) (11). The quality of the observational studies was evaluated using JBI critical appraisal checklists (12), with each study design having its own checklist. Each question in the checklist was assigned 1 point and percentages-based scores were calculated based on total points received by the study, scores > 70 indicating high quality, 50–70 indicating medium quality, and < 50 indicating low quality. Any disagreements were resolved through discussion to reach a consensus.
Statistical analysis
We used R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria), along with RStudio as an integrated development environment (Posit Team, 2024, Posit Software, PBC, Boston, MA), to analyse continuous variables for our study (13). The meta-analysis results were presented as standardized mean differences (SMD) with 95% confidence intervals (CI), and we applied a random-effects model using the inverse variance method for this analysis. Statistical heterogeneity was evaluated using the I-square (I²) statistic, with I² values > 60% indicating substantial heterogeneity, between 30% and 60% indicating moderate heterogeneity, and < 30% indicating low heterogeneity (14).
Only RCT studies that were graded as low risk of bias or having some concerns were included due to the greater quality of evidence and larger sample sizes. Non-RCT studies, those with a high risk of bias, or studies with incomplete data were excluded from the statistical analysis. Comparison of studies was performed by pooling together all studies as well as stratifying studies based on the type of severity score used. Subgroup analyses based on scoring systems, age group, and comparator used were conducted to explore variations among studies.
As a form of sensitivity analysis, both random-effects and fixed-effects models were used in the meta-analysis. However, the fixed-effects model was not preferred due to high heterogeneity and methodological differences across studies.
RESULTS
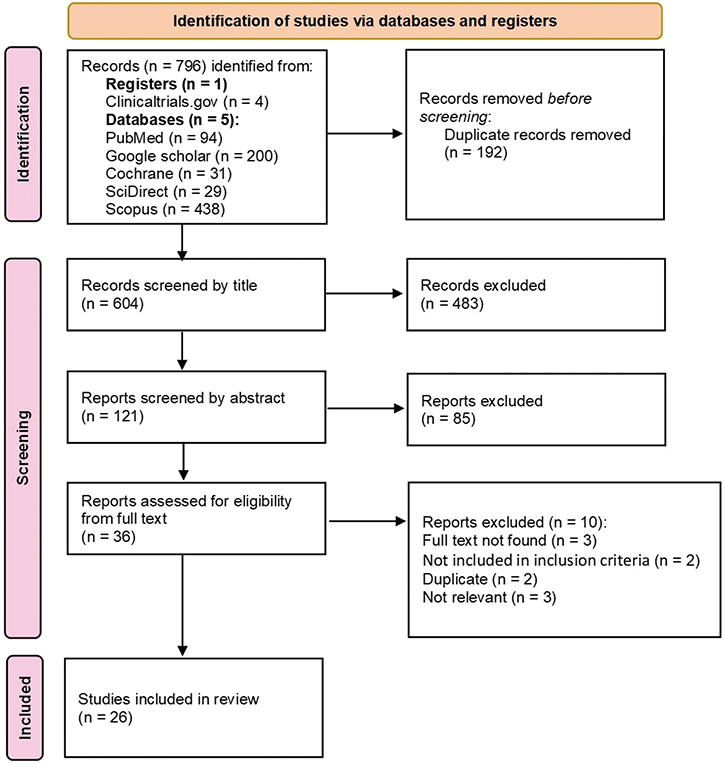
A total of 796 articles were identified during the preliminary search; 26 articles (8, 10, 15–38) of varying study designs were included in the final qualitative analysis (Fig. 1). The studies included a total of 742 participants with sample size ranging from 2 to 91 patients and ages ranging from 1–70 years. Most studies included both male and female participants except 2 studies: 1 that recruited only male subjects (10), and 1 with only female participants (15). The studies were conducted in 16 different countries. The dosages for montelukast used were either 4–5 mg for paediatric subjects or 10 mg for adults, while the dosage for zafirlukast was 20 mg in all subjects.
Outcomes were assessed using various measures across studies. Some utilized official severity scores such as SCORAD (Severity Scoring of Atopic Dermatitis), SASSAD (six area, six sign atopic dermatitis), EASI (Eczema Area and Severity Index), IGA (Investigator’s Global Assessment), ADASI (Atopic Dermatitis Area and Severity Index), or self-made scales while others relied on subjective metrics such as body surface area. Additionally, certain studies measured alternative parameters such as urinary LTE4 levels or flare diameters. Quality of life outcomes were also considered in some studies, using tools such as the CDLQI (Children’s Dermatology Life Quality Index) or DLQI (Dermatology Life Quality Index). Study characteristics are recorded in Table I.
| Author, country, year, (reference no.) | Study design | Initial Sample Size | Dropout rate (%) | Male/ female (M/F) | Age range | Study duration | Eligibility criteria | Treatment | Comparator | Concomitant therapy | Outcomes assessed |
| Angelova-Fischer et al., Bulgaria, 2005 (15) | Case series | 2 | 0% | 0/2 | 32 and 19 | 24 weeks | Patients diagnosed with AD | 10 mg of montelukast sodium OD | None | Emollient |
|
| Broshtilova et al., Bulgaria, 2010 (16) | Case series | 3 | 0% | 1/2 | 19–32 | 6 months | Patients diagnosed with AD | 10 mg of montelukast OD | none | Emollients |
|
| Capella et al., Italy, 2001 (17) | Randomized, single-blind, parallel-group study | 32 | 0% | 18/14 | 18+ | 6 weeks | Patient with moderate-to-severe eczema with SCORAD ≥ 30 | 10 mg of montelukast OD, oral placebo tablet thrice daily, and topical placebo gel twice daily | Cetirizine and clarithromycin, topical corticosteroids and hydrating preparations | Inhaled or intranasal medications, or eye drops, for cases with coexisting allergic asthma, rhinitis, or keratoconjunctivitis |
|
| Carucci et al., USA, 1998 (18) | Case series | 4 | 0% | 3/1 | 41–61 | Not given | Patients diagnosed with AD | 20 mg of zafirlukast orally twice per day | None | Antihistamines and topical steroids, prednisone, as required | Percentage of body surface area |
| Craig et al., USA, 2002 (19) | Randomized, double-blind, placebo-controlled, parallel study | 60 | Not stated | Not given | Not given | 8 weeks | Patients diagnosed with moderate to severe AD | 10 mg of montelukast OD | Placebo | Daily use of a lubricant and hydroxyzine |
|
| Ehlayel et al., Qatar, 2007 (20) | Randomized, double-blind, placebo-controlled, crossover study | 25 | 0 | 13/12 | 2–16 | 12 weeks | Patients diagnosed with moderate to severe AD according to Hanifin and Rajka’s criteria, who may also have allergic rhinitis and/or asthma, and who have not responded to conventional therapy | 5 mg of montelukast | Placebo | Nasal medications for allergic rhinitis and inhaled asthma medications were allowed if the dosage remained unchanged, as were antihistamines and topical steroids |
|
| Nettis et al, Italy, 2002 (10) | Randomized, double-blind, placebo-controlled, parallel study | 20 | 0% | 20/0 | 18–28 | 6 weeks | Patients with severe AD with a mean SCORAD index of > 40 | 10 mg of montelukast OD | Placebo | Emollients |
|
| Friedmann et al., UK 2007 (21) | Randomized, double-blind, placebo-controlled, parallel study | 60 | 10% | 20/40 | 16–60 | 10 weeks | Patients with moderate AD diagnosed according to Hanifin and Rajka criteria, having a SASSAD score between 12 and 50 at visits 1 and 2 | 10 mg of montelukast OD | Placebo | Emollients, antihistamines and corticosteroids provided that the use of these had been stable over the preceding month |
|
| Friedmann et al., UK, 2001 (22) | Quasi-experimental study | 11 | 0% | Not given | Not given | 2 weeks | Patients diagnosed with AD | 10 mg of montelukast OD | none | None |
|
| Goh et al., Australia, 2016 (23) | Randomized, parallel group, open label trial | 62 | Not stated | Not given | 6–16 | 8 weeks | Children diagnosed with AD | Montelukast with topical therapy | Topical therapy | not mentioned |
|
| Hon et al., Hong Kong, 2005 (8) | Case series | 7 | 0% | 4/3 | 3–16 | 3 months | Patients diagnosed with AD according to Hanifin and Rajka’s criteria with SCORAD greater than 15 | Ages < 12 years: 5 mg montelukast Ages > 12 years: 10 mg montelukast |
None | Each subject remained on same type of oral antihistamine or topical corticosteroid throughout the study | SCORAD scores |
| Ibrahim et al., Egypt, 2014 (24) | Case-controlled study | 32 | 0% | 16/16 | 8 adults 24 children | 2 weeks | Patients with AD diagnosed according to Hanifin and Rajka criteria | 4 mg of montelukast OD | none | none |
|
| Jamalyan et al., Armenia, 2024 (25) | Randomized, double-blind, placebo-controlled, parallel study | 91 | 0% | Not given | 21–37 | 12 weeks | Patients with a chronic AD diagnosis (at least 3 years) and a minimum of: an EASI score of 16, AD involving 10% of body surface area (BSA), an IGA score of 3 at, an average pruritus NRS score of 3, and an inadequate response to antihistamine therapy | 5 mg of desloratadine and 10 mg of montelukast OD | Desloratadine | Topical corticosteroid (Elocon) twice daily, emollient, a probiotic, thrice per day |
|
| Jeon et al., South Korea, 2016 (26) | Randomized, double-blind, placebo-controlled, crossover study | 54 | 20.40% | 21/22 | 2–6 | 20 weeks | Children with moderate to severe atopic dermatitis diagnosed according to Hanifin and Rajka’s criteria with a SCORAD greater than 15 | Ages < 6 years: 4 mg montelukast Ages ≥ 6 years: 5 mg montelukast |
Placebo | 0.1% hydrocortisone lotion twice daily) and emollients (3-4 times a day) |
|
| Kägi et al., Switzerland, 2001 (27) | Case series | 4 | 0% | Not given | Not given | 2 weeks | Patients with facial AD refractory to conventional treatment with topical steroids | 10 mg of montelukast OD | none | Emollients | Subjective opinion |
| Lee et al., South Korea, 2007 (28) | Quasi-experimental study | 10 | Not stated | 8/2 | 8–36 | 8 Weeks | Patients with severe AD diagnosed according to Hanifin and Rajka criteria | 10 mg of montelukast OD | None | Not mentioned |
|
| Lehtimäki et al., Finland, 2009 (29) | Randomized, double-blind, placebo-controlled, crossover study | 49 | 26.20% | 12/33 | 18–40 | 6 weeks | Patients with a wheal diameter ≥ 4 mm on skin-prick tests for both birch and timothy pollen, experiencing allergic symptoms in both upper and lower airways during pollen season, and with at least one other type of allergy | 10 mg of montelukast OD | Placebo | Short-acting antihistamine capsules and a short-acting inhaled beta 2 agonist were allowed as needed |
|
| Melamed et al., USA, 2017 (30) | Randomized, double-blind, placebo controlled, parallel study | 20 | Not stated | 11/.9 | 1–8 | 9 weeks | Patients with a positive reactivity to food (indicated by skin or RAST test) with 10–25% body area affected by AD | Ages 2-5 years: 4 mg montelukast Ages 6-8 years: 5 mg montelukast |
Placebo | A 1% hydrocortisone cream, and cetirizine HCl (Zyrtec) liquid was used when symptoms became severe |
|
| Pei et al., Hong Kong, 2001 (31) | Randomized, double-blind, placebo-controlled, crossover study | 15 | 26.66% | 4/7 | 6–16 | 12 weeks | Patients diagnosed with chronic moderate-to-severe AD according to Hanifin and Rajka’s criteria and resistant to conventional treatment | Montelukast | Placebo | 70% light liquid paraffin as soap substitute, emollient, and 0.05% clobetasone butyrate cream |
|
| Rahman et al., Bangladesh, 2006 (32) | Randomized, parallel group, open label trial | 31 | 0% | 17/14 | ≥ 6 | 4 weeks | Patients diagnosed with AD according to Hanifin and Rajka’s criteria, with at least 1 year of intermittent or persistent symptoms of AD and a SCORAD ≥ 30 | Ages 6–14 years: 5 mg montelukast once daily Ages > 14 years: 10 mg montelukast once daily |
Antihistamines and topical hydrocortisone | None | SCORAD (subjective and objective observations) |
| Sekerel et al., Turkey, 2003 (33) | Randomized, double-blind, placebo-controlled, crossover study | 31 | 3.20% | 20/10 | 6–15 | 3 weeks | Patients with ECARs and LCARs to Dermatophagoides pteronyssinus, and a value of pre-bronchodilator FEV1 greater than 70% of the predicted value | Montelukast 5mg/day for 2 days | Placebo | Not mentioned | Mean of longest diameter and longest perpendicular of the induration response |
| Silverberg et al., USA, 2004 (34) | Case series | 7 | 0% | Not given | 4–65 | 4 weeks | Patients with severe AD affecting more than 90% of body surface area | 5 mg of montelukast OD 15-year-olds received 10 mg of montelukast OD Adults received 20 mg of zafirlukast twice daily |
None | One 8-year-old girl hydroxyzine nightly. All patients continued their use of topical steroid with a potency class of 2–3 | Observation of dermatitis on body surface area |
| Veien et al. Denmark, 2005 (35) | Randomized, double-blind, placebo-controlled, crossover study | 59 | 20.30% | 16/43 | 16–70 | 6 weeks | Moderate to severe AD diagnosed according to Hanifin and Rajka’s criteria with involvement of 5–35% of the body surface and a minimum score of 4.5 based on Rajka and Langeland’s grading system | 10 mg montelukast | Placebo | Emollient | Modified EASI score as well as a pruritus score |
| Xabibullayevna et al., Uzbekistan, 2021 (36) | Randomized, parallel group, open label trial | 40 | Not stated | 20/20 | 2–12 | 4 weeks | Patients diagnosed with AD | Ages 2–5 years: 4 mg montelukast Ages 6–12 years: 5 mg montelukast |
Montelucast vs Singulon | None |
|
| Yanase et al., USA, 2001 (37) | Randomized, double-blind, placebo-controlled, crossover study | 8 | 0% | Not given | ≥ 18 | 5 weeks | Patients with persistent AD diagnosed according to Hanifin and Rajka criteria | 10 mg of montelukast OD | Placebo | Emollients, antihistamines, and weak topical steroids when necessary | ADASI score assessing erythema, papulation, excoriation, lichenification, scaling/dryness, and erosion/oozing |
| Zabawski et al., USA, 1999 (38) | Case series | 5 | 0% | 1/4 | 8–45 | 10 days–4 weeks | Patients diagnosed with AD | 10 mg zafirlukast twice daily for 8 year olds, 20 mg twice daily for other patients | None | Corticosteroids or emollients were used as needed | Objective and subjective observations for improvement of disease |
| AD: atopic dermatitis; OD: once daily; SCORAD: Severity Scoring of Atopic Dermatitis 1; IgE: immunoglobulin E; SASSAD: six area, six sign atopic dermatitis; CDLQI: Children’s Dermatology Life Quality Index; FLG: filaggrin; EASI: Eczema Area and Severity Index; IGA: Investigator’s Global Assessment; LTE4: leukotriene E4; EDN: eaosinophil-derived neurotoxin; QoL: quality of life; ECAR: early cutaneous allergic response; LCAR: late cutaneous allergic response; FEV1: forced expiratory volume; PEFR1: peak expiratory flow rate; ADASI: Atopic Dermatitis Area and Severity Index. | |||||||||||
Quality assessment
Sixteen studies were evaluated using RoB-2 (https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials): 9 parallel and 7 crossover RCTs. Among these, 3 showed low concern, 8 had some concern, and 5 were rated high concern (Fig. 2).

Fig. 2. Risk of bias summary. Review of authors’ judgements on the level of risk of bias across each bias domain for parallel randomized controlled trials (RCTs) on right and crossover RCTs on the left. D = domain.
Ten studies were assessed using the JBI critical appraisal checklists (12). Among these studies, 5 were rated high quality, 1 medium, and 3 low (Fig. 3).
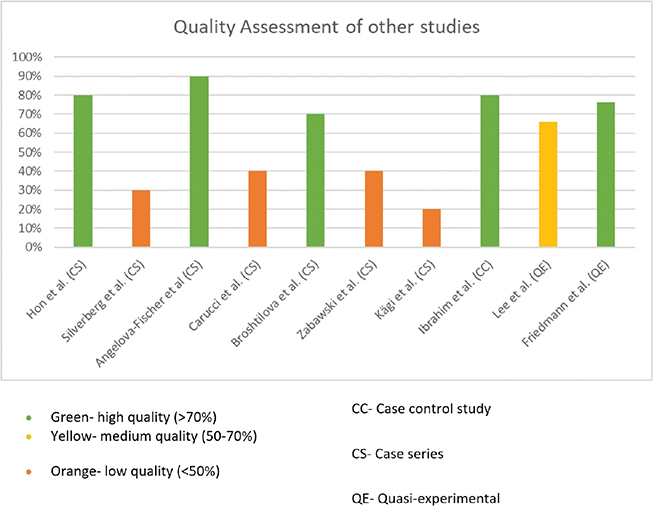
Fig. 3. Quality assessment graph showing authors’ assessments, presented as percentages for all studies except randomized controlled trials (RCTs).
Meta analysis
Analysis was done only for studies using EASI and SCORAD due to insufficient data present for other severity scores or lack of appropriate comparability. A total of 7 groups using both scoring systems were analysed. In comparison with the control group (n = 191), our meta-analysis showed a non-significant effect of montelukast in reducing severity scores in the intervention group (n = 183; SMD = –0.99 at 95% CI –2.11 to 0.13, p = 0.0828, I2 = 94.4%) (Fig. 4).
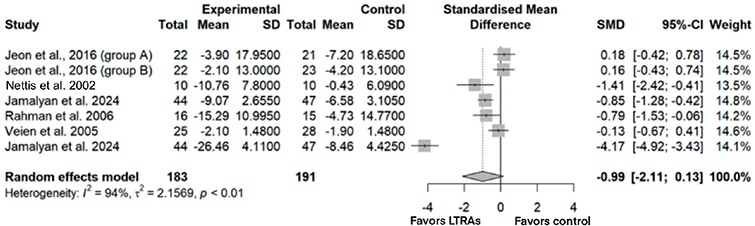
Fig. 4. Forest plot for meta-analysis of all studies. LTRAs = leukotriene receptor antagonists.
Subgroup analyses
Subgroup analyses stratified studies by severity scoring (EASI or SCORAD), population (paediatric or adult), and control type (placebo or conventional treatment). Forest plots and details of each analysis are available in Figs S1–S6. While montelukast reduced severity scores in both EASI and SCORAD analyses, the results were not statistically significant. In the SCORAD paediatric vs adult analysis, reductions were observed in both groups, but significance was reached only in adults (intervention n = 54; SMD = –0.94, 95% CI–1.35 to –0.54, p < 0.0001, I² = 1.8%). Similarly, in the SCORAD analysis comparing placebo and conventional treatment controls (antihistamines and/or corticosteroids), reductions occurred in both subgroups, but significance was achieved only with conventional treatment (intervention n = 60; SMD = –0.84, 95% CI –1.21 to –0.47, p < 0.0001, I² = 0%).
NARRATIVE SYNTHESIS
Severity and improvement of AD
A total of 26 studies were utilized in narrative synthesis across adult, paediatric, and mixed populations. The relevant findings of each study are presented in Table II. SCORAD, used in 13 studies (5 paediatric), was the most common tool for assessing pruritus, erythema, and other symptoms. SCORAD assessments included both objective measures, such as extent and intensity of lesions, and subjective measures such as patient discomfort.
| Author, country, year, (reference no.) | Results |
| Angelova-Fischer et al., Bulgaria, 2005 (15) |
|
| Broshtilova et al., Bulgaria, 2010 (16) |
|
| Capella et al., Italy, 2001 (17) |
|
| Carucci et al., USA, 1998 (18) |
|
| Craig et al., USA, 2002 (19) |
|
| Ehlayel et al., Qatar, 2007 (20) |
|
| Nettis et al., Italy, 2002 (10) |
|
| Friedmann et al., UK, 2007 (21) |
|
| Friedmann et al., UK, 2001 (22) |
|
| Goh et al., Australia, 2016 (23) |
|
| Hon et al., Hong Kong, 2005 (8) |
|
| Ibrahim et al., Egypt, 2014 (24) |
|
| Jamalyan et al., Armenia, 2024 (25) |
|
| Jeon et al., South Korea, 2016 (26) |
|
| Kägi et al., Switzerland, 2001 (27) |
|
| Lee et al., South Korea, 2007 (28) |
|
| Lehtimäki et al., Finland, 2009 (29) |
|
| Melamed et al., USA, 2017 (30) |
|
| Pei et al., Hong Kong, 2001 (31) |
|
| Rahman et al., Bangladesh, 2006 (32) |
|
| Sekerel et al., Turkey, 2003 (33) |
|
| Silverberg et al., USA, 2004 (34) |
|
| Veien et al. Denmark, 2005 (35) |
|
| Xabibullayevna et al., Uzbekistan, 2021 (36) |
|
| Yanase et al., USA, 2001 (37) |
|
| Zabawski et al., USA, 1999 (38) |
|
| SCORAD: Severity Scoring of Atopic Dermatitis; AD: atopic dermatitis; SASSAD: six area, six sign atopic dermatitis; CDLQI: Children’s Dermatology Life Quality Index; GISS: Global Individual Signs Score; EASI: Eczema Area and Severity Index; PPNRS: Peak Pruritus Numerical Rating Scale; DLQI: Dermatology Life Quality Index; LTRAs: leukotriene receptor antagonists; QoL: quality of life; IgE: immunoglobulin E. | |
A total of 18 studies favoured the use of LTRAs, while 8 studies did not show significant benefits. Even among the studies that did not find statistically significant results, most still reported some positive effects, such as reductions in AD severity. Of 20 longer duration studies (≥ 4 weeks), 8 studies (7 RCTs and 1 case series) did not find LTRAs to be significantly beneficial. Notably, the case series by Silverberg and Paller (34) found an initial temporary improvement in AD, after which symptoms reappeared. Most studies using zafirlukast showed improvement, while montelukast had inconsistent outcomes. Studies favouring montelukast were generally smaller, whereas those showing no significant benefit often had larger sample sizes. Six adult and 7 paediatric studies supported montelukast, while 2 in each group did not.
Overall, montelukast helped alleviate pruritus but had little effect on skin dryness, and showed a generally positive but mixed response across studies.
LTRAs vs placebo
Among 11 placebo-controlled RCTs, montelukast showed mixed effectiveness in reducing AD severity. Four studies reported significant improvements, particularly in pruritus, while the others found no significant differences compared with placebo. For example, Goh et al. (23) reported a 32% reduction in SCORAD scores with montelukast vs 10% with placebo (p = 0.047), indicating moderate benefit. Other studies noted no significant changes in secondary outcomes such as skin dryness, rescue medication use, or disease extent.
LTRAs vs conventional treatment
In 5 RCTs, montelukast significantly reduced AD severity, showing efficacy comparable to conventional treatments such as antihistamines and/or corticosteroids. Rahman et al. (32) found it as effective as topical steroids and antihistamines, especially for pruritus and erythema, while Capella et al. (17) reported significant improvements and score reductions that were similar to but had no advantage over conventional therapy. Notably, 2 studies found montelukast combined with antihistamines to be more effective than conventional treatment alone.
Biological markers associated with AD
Markers such as eosinophilic cationic protein (ECP), eosinophil protein X (EPX), immunoglobulin E (IgE), and urinary leukotriene E4 (LTE4) were evaluated. Montelukast significantly reduced serum ECP and EPX, and urinary LTE4s levels in some studies, suggesting modulation of eosinophil activity and inflammation, though others found no significant changes. Ibrahim et al. (24) detected the FLG mutation 2282del4 in all 20 AD patients, who showed significant reductions in eosinophil levels and improvements in SCORAD and IgE levels (p < 0.05) after montelukast treatment. Several studies also found a decrease in cys-LT levels. These findings underscore the complexity of AD and the need for further research to clarify how montelukast influences specific biomarkers associated with the disease.
Quality of life (QoL)
QoL of patients with AD was reported only in some studies using patient-reported outcomes. In a paediatric study by Goh et al. (23), CDLQI was used to assess QoL, and reported a 50% improvement in the montelukast group compared with a 23% improvement in the control group. However, in the study performed by Pei et al. (31), no significant difference in QoL scores was noted between montelukast and placebo.
Rescue medication
Most studies did not provide detailed information on rescue medication. Friedmann et al. (21) assessed the frequency of corticosteroid use but found no significant steroid-sparing effect, with similar use in both the montelukast and placebo groups. Lehtimäki et al. (29) and Ehlayel et al. (20) also reported no difference, while Melamed (30) noted a trend towards reduced rescue medication use.
Emollient usage
Emollient use was not a primary focus in the studies reviewed but was included as part of treatment regimens alongside other therapies. While trials mentioned emollients, their impact on montelukast’s efficacy or on reducing the need for treatments like corticosteroids was not directly assessed.
Adverse effects
Montelukast’s adverse effects in AD treatment were generally mild and infrequent. Three studies reported notable effects: Friedmann et al. (21) observed septicaemia and dizziness, Sekerel and Akpinarli (33) found no difference between groups, and Jamalayan and Azaryan (25) noted mild effects (in 13.6% of patients) such as conjunctivitis and nasopharyngitis without discontinuation. Its safety profile was comparable to conventional treatments, with no significant long-term toxicity, though monitoring patients for potential reactions during treatment remains important.
DISCUSSION
This review synthesized data from 26 studies examining montelukast’s efficacy in AD across adult, paediatric, and mixed populations. We observed that LTRAs show some improvement in AD, but the clinical significance is variable.
Our findings align with prior reviews by Chin et al. and Ferguson et al., showing montelukast’s superiority to conventional treatments and a non-significant trend favouring it over placebo (39, 40). Unlike these reviews, our broader scope – 26 studies, compared with Ferguson et al.’s 5 and Chin et al.’s 11 studies – allowed for subgroup analyses by population and scoring systems, addressing heterogeneity. Our inclusion of all LTRAs, not just montelukast, further expanded the review.
Our subgroup analyses also reached statistical significance in 2 subgroups, providing additional insights beyond previous reviews. Overall, our results tend to be more favourable towards LTRAs than those reported by Chin et al. and Ferguson et al. (39, 40), likely due to our inclusion of a larger and more diverse set of studies.
Our meta-analysis yielded mixed results. Montelukast demonstrated no significant improvement in AD severity, whether evaluated using both EASI and SCORAD indices or each score separately. Our overall analysis showed a non-significant trend favouring montelukast, likely due to high heterogeneity (I² = 94%) from variations in patient and control populations, scores used, and study quality. Subgroup analyses were conducted to address this and better understand montelukast’s impact on AD.
The EASI subgroup showed a trend favouring montelukast, though it was not statistically significant. This was likely due to the presence of only 2 studies and high heterogeneity (I² = 99%), reducing statistical power. The lower-quality study by Veien et al. (35) showed minimal effect, while Jamalyan and Azaryan’s more recent, higher-quality study (25), with a longer duration and larger sample size, showed stronger results. However, this may be due to the fact that montelukast was used in combination with antihistamines. Results were significant under the fixed-effects model but not the random-effects model, reflecting substantial study variability.
In the SCORAD subgroup, montelukast showed some benefits but lacked statistical significance. The placebo-controlled, high-quality, long-duration paediatric study by Jeon et al. (26) found no benefit, possibly due to greater power and crossover effects. In contrast, the lower-quality paediatric study by Rahman et al. (32) and Jamalyan and Azaryan’s high-quality study (25) favoured montelukast but used conventional treatment as a comparator. Results were significant under the fixed-effects model but not the random-effects model, similar to the EASI group analysis. The observed heterogeneity across populations, study designs, comparators, and quality likely contributed to the lack of statistical significance.
In both the pediatric and placebo subgroups of studies using SCORAD, no statistical significance was found under either the fixed or random-effects model, likely due to the same reasons as the overall SCORAD subgroup.
In the adult subgroup of studies using SCORAD, montelukast significantly improved SCORAD scores, supported by Jamalyan and Azaryan’s high-quality study (25) using adjunct therapy and Nettis et al. 2002’s standalone treatment study. Low heterogeneity (I² = 2%) strengthens these results. These findings suggest montelukast may be effective for adults, particularly with combination therapy, though further studies are needed.
In the conventional treatment subgroup using SCORAD, statistically significant results favouring montelukast were observed, with low heterogeneity (I² = 0%) reinforcing the findings. The high-quality study by Jamalayan and Azaryan (25) focused on adults, while the study by Rahman et al. (32) of moderate quality examined paediatric patients, suggesting montelukast may have comparable efficacy across age groups as opposed to the findings in the paediatric subgroup.
The disparity between the placebo and conventional treatment subgroups could be explained by the difference in population size, as the conventional subgroup has a higher sample size (n = 122) compared with placebo (n = 108). There was no difference in the number of high-quality studies or between the number of paediatric studies between the 2 groups. Another possible confounding factor could be that Jamalayan and Azaryan’s study (25) utilized montelukast along with antihistamines vs antihistamines, and the use of montelukast as an adjunct treatment could have tipped the results in favour of montelukast.
Montelukast was generally well tolerated, with mild side effects reported and no neuropsychiatric events noted in the reviewed studies. The 2007 study by Friedmann et al. (21) noted septicaemia, but it is unlikely to be related to montelukast. Its safety profile is comparable to conventional AD treatments, making it a potential option for patients who cannot use standard therapies. Most studies lacked details on coexisting atopic conditions; however, Lehtimäki et al. (29) evaluated its effectiveness in individuals with comorbid allergic disorders and found it to be ineffective in managing non-airway-related allergies in patients with atopic syndrome.
While montelukast may benefit select adult populations, particularly as an adjunct treatment, its efficacy remains inconsistent, and more effective treatments are available. Genetic factors such as the FLG mutation were linked to improved SCORAD and IgE levels, suggesting that biomarker-driven approaches could identify patients who may benefit most from montelukast. Montelukast is not recommended for AD in current guidelines, its use for this condition remains primarily off-label, and further research is needed to clarify its role.
Limitations
A key limitation was the lack of standardized scoring systems for assessing AD severity, complicating comparisons and hindering unified data analysis. High heterogeneity further challenged meta-analyses. Additionally, some studies lacked numerical data, with Nettis et al. 2002’s study requiring estimations via tools like WebPlotDigitizer, introducing potential error.
Most studies were underpowered with small sample sizes, risking type II errors or overestimating benefits due to statistical bias. Furthermore, the focus was primarily on montelukast, with limited data on other LTRAs like zafirlukast. Disease severity also varied, with most studies involving moderate cases and fewer examining severe or mild AD. Diagnostic criteria for AD differed across studies, with some studies lacking detail. However, all studies used for statistical analysis employed valid diagnostic methods such as Hanifin and Rajka criteria or severity scores above particular cut-off values.
Concomitant therapies, including antihistamines, topical corticosteroids, and antibiotics, were common. For instance, the study by Capella et al. (21) included antibiotics, which are not standard AD treatments. Additionally, the lack of clarity on rescue medication use complicated the evaluation of montelukast’s standalone efficacy in the narrative synthesis. However, in all studies included in the statistical analysis, concomitant therapies were either prohibited or administered at standardized doses uniformly across both experimental and control groups. Despite limitations, our analysis yielded some statistically significant results, providing valuable insights into montelukast’s effects in patients with AD.
Future directions
Future research should prioritize larger, long-term, multicentre trials with standardized assessment tools to enhance comparability and consistency. Exploring biomarker-driven approaches could identify subgroups likely to benefit, while studies on combination therapies may reveal montelukast’s potential to enhance conventional treatments. Paediatric-focused research is especially important, given montelukast’s suitability as an oral treatment for children and its demonstrated efficacy in adults, suggesting potential benefits in younger populations.
CONCLUSION
Montelukast shows promise, particularly in adult populations and as an adjunct to conventional treatments, but its effectiveness in AD is variable. While it offers modest benefits, especially in relieving pruritus, its overall efficacy remains inconsistent. Given its favourable safety profile, montelukast may be a useful adjunct therapy, particularly for patients with comorbid asthma. However, it should not replace standard treatments in comprehensive AD management. Future research should focus on standardizing assessments and developing patient-specific approaches to better define montelukast’s role in AD treatment.
REFERENCES
- Weidinger S, Novak N. Atopic dermatitis. Lancet 2016; 387: 1109–1122. https://doi.org/10.1016/S0140-6736(15)00149-X
- Boguniewicz M, Leung DY. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunol Rev 2011; 242: 233–246. https://doi.org/10.1111/j.1600-065X.2011.01027.x
- Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol 2014; 71: 116–132. https://doi.org/10.1016/j.jaad.2014.03.023
- Jo-Watanabe A, Okuno T, Yokomizo T. The role of leukotrienes as potential therapeutic targets in allergic disorders. Int J Mol Sci 2019; 20: 3580. https://doi.org/10.3390/ijms20143580
- Honda T, Kabashima K. Prostanoids and leukotrienes in the pathophysiology of atopic dermatitis and psoriasis. Int Immunol 2019; 31: 589–595. https://doi.org/10.1093/intimm/dxy087
- Pratamasari MA, Hoetomo MM, Hidayati AN. Urinary leukotriene e4 level profile in various degrees of severity in atopic dermatitis patients in dermatovenereology outpatient clinic Dr. Soetomo General Hospital, Surabaya: a descriptive study. Dermatol Reports 2019;11: s1.
- Morais-Almeida M, Cabral AJ. Off-label prescribing for allergic diseases in pre-school children. Allergol Immunopathol (Madr) 2014;42: 342–347. https://doi.org/10.1016/j.aller.2013.02.011
- Biswas P, Wilton LV, Shakir SA. Montelukast and improvement of eczema: observations from a prescription event monitoring study in England. Int J Clin Pharmacol Ther 2001; 39: 529–533. https://doi.org/10.5414/cpp39529
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. https://doi.org/10.1136/bmj.n71
- Nettis E, Pannofino A, Fanelli M, Ferrannini A, Tursi A. Efficacy and tolerability of montelukast as a therapeutic agent for severe atopic dermatitis in adults. Acta Derm Venereol 2002; 82: 297–298. https://doi.org/10.1080/000155502320323298
- Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011; 343: d5928. https://doi.org/10.1136/bmj.d5928
- Munn Z, Barker TH, Moola S, Tufanaru C, Stern C, McArthur A, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth 2020; 18: 2127–2133.
- R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing, 2024. https://www.R-project.org/
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Chapter 10: Analysing data and undertaking meta-analyses. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. Available from: www.training.cochrane.org/handbook.
- Angelova-Fischer I, Tsankov N. Successful treatment of severe atopic dermatitis with cysteinyl leukotriene receptor antagonist montelukast. Acta Derm Venereol Alp Panonn Adriat 2005; 14: 115–119.
- Broshtilova V, Gantcheva M. Therapeutic Hotline: Cysteinyl leukotriene receptor antagonist montelukast in the treatment of atopic dermatitis. Dermatol Ther 2010; 23: 90–93. https://doi.org/10.1111/j.1529-8019.2009.01295.x
- Capella GL, Grigerio E, Altomare G. A randomized trial of leukotriene receptor antagonist montelukast in moderate-to-severe atopic dermatitis of adults. Eur J Dermatol 2001; 11: 209–213.
- Carucci JA, Washenik K, Weinstein A, Shupack J, Cohen DE. The leukotriene antagonist zafirlukast as a therapeutic agent for atopic dermatitis. Arch Dermatol 1998; 134: 785–786. https://doi.org/10.1001/archderm.134.7.785
- Craig T, Correale C, Chinchilli V, Lehman E, Mende C, Longernecker A, et al. The effects of montelukast on atopic dermatitis (AD): a placebo-controlled, double-blind, parallel study. J Allergy Clin Immunol 2002; 109: 10. https://doi.org/10.1016/S0091-6749(02)81608-6
- Ehlayel MS, Bener A, Sabbah A. Montelukast treatment in children with moderately severe atopic dermatitis. Eur Ann Allergy Clin Immunol 2007; 39: 232–236.
- Friedmann PS, Palmer R, Tan E, Ogboli M, Barclay G, Hotchkiss K, et al. A double-blind, placebo-controlled trial of montelukast in adult atopic eczema. Clin Exp Allergy 2007; 37: 1536–1540. https://doi.org/10.1111/j.1365-2222.2007.02811.x
- Friedmann PS, Perzanowska M, McGuire C, Nayak N, Clough GF, Sampson AP, et al. New therapeutic indications for Cys-LT1 antagonists: atopic dermatitis and urticaria. Clin Exp Allergy Rev 2001; 1: 156–159. https://doi.org/10.1046/j.1472-9725.2001.00030.x
- Goh A, Lowe A, Zallmann S, Su J. The effectiveness of montelukast as adjunct treatment among children with atopic dermatitis: an open-label, randomized controlled trial. Australas J Dermatol 2016; 57: 52.
- Ibrahim HM, Mohamed AH, Atalla RB, Ahmed AM, Hamada HYI. Effectiveness of montelukast in modulation of filaggrin mutation 2282del4 in atopic dermatitis Egyptian patients. J App Pharm Sci 2014; 4: 014–020. https://doi.org/10.7324/JAPS.2014.40103
- Jamalyan KR, Azaryan HG. Comparative efficacy of combined antihistamine and montelukast therapy in adult patients with atopic dermatitis. Postepy Dermatol Alergol 2024; 41: 32–40. https://doi.org/10.5114/ada.2023.135759
- Jeon YH, Min TK, Yang HJ, Pyun BY. A double-blind, randomized, crossover study to compare the effectiveness of montelukast on atopic dermatitis in Korean children. Allergy Asthma Immunol Res 2016; 8: 305–311. https://doi.org/10.4168/aair.2016.8.4.305
- Kägi MK. Leukotriene receptor antagonists: a novel therapeutic approach in atopic dermatitis? Dermatology 2001; 203: 280–283. https://doi.org/10.1159/000051772
- Lee CK, Ku BS, Kim KH, Young KL. The effect of montelukast in the treatment of atopic dermatitis through the SCORAD index. J Am Acad Dermatol 2007; 56: AB68. https://doi.org/10.1016/j.jaad.2006.10.335
- Lehtimäki L, Petäys T, Haahtela T. Montelukast is not effective in controlling allergic symptoms outside the airways: a randomised double-blind placebo-controlled crossover study. Int Arch Allergy Immunol 2009; 149: 150–153. https://doi.org/10.1159/000189198
- Melamed IR. The benefit of montelukast in atopic dermatitis induced by food allergies. J Allergy Clin Immunol 2010; 125: AB93. https://doi.org/10.1016/j.jaci.2009.12.366
- Pei AY, Chan HH, Leung TF. Montelukast in the treatment of children with moderate-to-severe atopic dermatitis: a pilot study. Pediatr Allergy Immunol 2001; 12: 154–158. https://doi.org/10.1034/j.1399-3038.2001.012003154.x
- Rahman ML, Choudhury AM, Islam MM. Effectiveness of montelukast in the treatment of atopic dermatitis. Mymensingh Med J 2006; 15: 85–88. https://doi.org/10.3329/mmj.v15i1.8
- Sekerel BE, Akpinarli A. The effect of montelukast on allergen-induced cutaneous responses in house dust mite allergic children. Pediatr Allergy Immunol 2003; 14: 212–215. https://doi.org/10.1034/j.1399-3038.2003.00038.x
- Silverberg NB, Paller AS. Leukotriene receptor antagonists are ineffective for severe atopic dermatitis. J Am Acad Dermatol 2004; 50: 485–486. https://doi.org/10.1016/s0190-9622(03)00758-8
- Veien NK, Busch-Sørensen M, Stausbøl-Grøn B. Montelukast treatment of moderate to severe atopic dermatitis in adults: a randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol 2005; 53: 147–149. https://doi.org/10.1016/j.jaad.2004.12.011
- Xabibullayevna MM, Telmanovna AD, Gayratovna AD, Abdukarimovna SM, Masrurovna AM. Antileukotriene drugs in the treatment of atopic dermatitis in children. Int J Pharm Res 2021; 13: 2117.
- Yanase DJ, David-Bajar K. The leukotriene antagonist montelukast as a therapeutic agent for atopic dermatitis. J Am Acad Dermatol 2001; 44: 89–93. https://doi.org/10.1067/mjd.2001.111352
- Zabawski EJ Jr, Kahn MA, Gregg LJ. Treatment of atopic dermatitis with zafirlukast. Dermatol Online J 1999; 5: 10. https://doi.org/10.5070/D3589055T9
- Chin WK, Lee SWH. A systematic review on the off-label use of montelukast in atopic dermatitis treatment. Int J Clin Pharm 2018; 40: 963–976. https://doi.org/10.1007/s11096-018-0655-3
- Ferguson L, Futamura M, Vakirlis E, Kojima R, Sasaki H, Roberts A, et al. Leukotriene receptor antagonists for eczema. Cochrane Database Syst Rev 2018; 10: CD011224. https://doi.org/10.1002/14651858.CD011224.pub2