QUIZ SECTION
Multiple Papules and Nodules in a Dermatomal Distribution: A Quiz
Roberto RUSSO1,2, Ilaria SALVI1,2, Antonio GUADAGNO3, Aurora PARODI1,2 and Emanuele COZZANI1,2*
1Department of Dermatology, Dipartimento di scienze della salute – DISSAL, University of Genoa, Genoa, 2IRCCS Ospedale Policlinico San Martino, Genoa, and 3Pathology Unit, IRCCS Ospedale Policlinico San Martino, Genoa, Italy. *E-mail: emanuele.cozzani@unige.it
Citation: Acta Derm Venereol 2025; 105: adv43203. DOI: https://doi.org/10.2340/actadv.v105.43203.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Sep 29, 2025
An otherwise healthy 37-year-old male presented to a dermatology appointment for asymptomatic cutaneous lesions that had gradually appeared on the right lumbar region over the course of a few years. On examination, numerous flesh-coloured, soft papules and nodules with a smooth surface were arranged in a dermatomal distribution in the right lumbar region (Fig. 1). Dermoscopy (DermLite DL4, 10X; DermLite, Aliso Viejo, CA, USA) revealed featureless flesh-coloured papules and nodules (Fig. 2). No other clinically relevant skin lesions were present.

Fig. 1. Multiple flesh-coloured, soft papules and nodules with a smooth surface arranged in a dermatomal distribution in the right lumbar region.
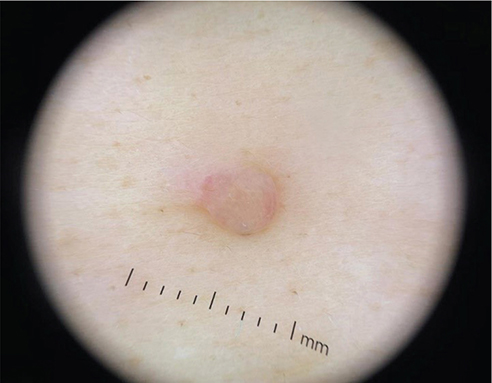
Fig. 2. Featureless flesh-coloured papules and nodules at dermoscopy (DermLite DL4, 10X).
A deep shave biopsy of 1 of the lesions was obtained.
What is your diagnosis?
1: Cutaneous piloleiomyomas
2: Segmental neurofibromatosis
3: Zosteriform cutaneous metastasis
4: Agminated Spitz nevi
See next page for answer.
ANSWERS TO QUIZ
Multiple Papules and Nodules in a Dermatomal Distribution: A Commentary
Diagnosis: Segmental neurofibromatosis
The histopathological examination of the skin biopsy revealed a dermal proliferation composed of spindle cells with scanty pale cytoplasm and wavy nuclei set in a collagenous stroma (Fig. 3A, B). The neoplastic cells were positive for pS100 staining (Fig. 3C) and negative for Melan-A, EMA ed CD57 (not shown). The sampled lesion was identified as a cutaneous neurofibroma.
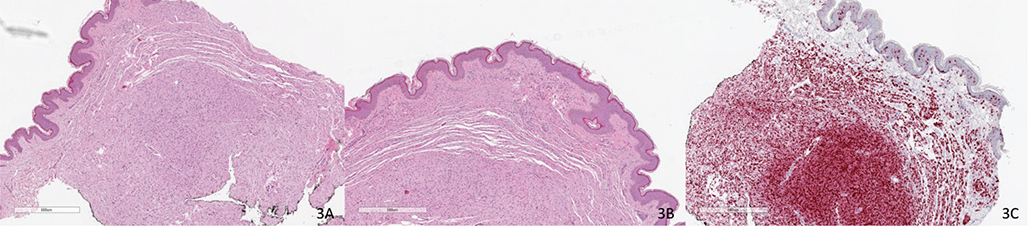
Fig. 3. Haematoxylin-eosin staining of the skin biopsy revealed (A–B) a dermal proliferation composed of spindle cells with scanty pale cytoplasm and wavy nuclei set in a collagenous stroma. (C). The neoplastic cells were positive for pS100 staining.
Due to the typical arrangement of the lesions and the lack of other features typical of neurofibromatosis, a diagnosis of segmental neurofibromatosis was made.
Segmental neurofibromatosis (also known as type V neurofibromatosis) is an atypical presentation of type I neurofibromatosis (von Recklinghausen syndrome). It is a rare disorder, with a prevalence between 0.0014% and 0.002%, although its actual prevalence could be higher due to possible underdiagnosis (1). In a review of the literature, the reported median age of onset was 28 years (2).
Neurofibromas are the most common cutaneous manifestation of segmental neurofibromatosis, but café-au-lait spots and axillary freckling can also occur. Clinically, patients may be divided into 4 groups: with only pigmentary lesions, with only neurofibromas, with both pigmentary lesions and neurofibromas, and with isolated plexiform neurofibromas. Segmental neurofibromatosis is generally unilateral with involvement of a single dermatome, although bilateral cases have been reported (3).
Segmental neurofibromatosis is associated with a postzygotic mutation in the NF1 gene, resulting in a somatic mosaicism. The time of mutation and the affected cell type determine the clinical phenotype, which can be extremely variable. If the mosaicism involves the gonadal cells, offspring of affected individuals can inherit the classical form of neurofibromatosis type I (4). After a thorough physical examination to exclude the presence of other cutaneous or ocular signs of neurofibromatosis, patients with segmental type I neurofibromatosis should be reassured that they are not affected by the generalized form of the disease. They should also be counselled about the small risk of having children with classical type I neurofibromatosis in the case of a mosaicism involving the gonadal cells (1). While there is no definitive treatment for segmental neurofibromatosis, large disfiguring and painful lesions, when present, can be treated by surgical excision (5).
REFERENCES
- Adigun CG, Stein J. Segmental neurofibromatosis. Dermatol Online J 2011; 17: 25. https://doi.org/10.5070/D38M71W0WH
- Hager CM, Cohen PR, Tschen JA. Segmental neurofibromatosis: case reports and review. J Am Acad Dermatol 1997; 37: 864–869. https://doi.org/10.1016/S0190-9622(97)80013-8
- Sobjanek M, Dobosz-Kawałko M, Michajłowski I, Pęksa R, Nowicki R. Segmental neurofibromatosis. Postepy Dermatol Alergol 2014; 31: 410–412. https://doi.org/10.5114/pdia.2014.40942
- Schultz ES, Kaufmann D, Tinschert S, Schell H, von den Driesch P, Schuler G. Segmental neurofibromatosis. Dermatology 2002; 204: 296–297. https://doi.org/10.1159/000063363
- Raju D, Ghosh N, Das S, Krishnan P. Segmental neurofibromatosis. J Neurosci Rural Pract 2021; 12: 441–442. https://doi.org/10.1055/s-0040-1721197