ORIGINAL REPORT
Photoaging and Cosmetic Result with Artificial Daylight Photodynamic Therapy Using Methyl Aminolevulinate
Rolf-Markus SZEIMIES  1, Matthias BRÜCKNER2, Matthias HOFFMANN3, Melvin BAÉ 4, Jörg FRÄNKEN5, Bernd GROßMANN6, Uwe PAASCH 7, Sven QUIST 8, Berenice M. LANG 9, Rajeev CHAVDA 10 and Wolfgang G. PHILIPP-DORMSTON 11,12
1, Matthias BRÜCKNER2, Matthias HOFFMANN3, Melvin BAÉ 4, Jörg FRÄNKEN5, Bernd GROßMANN6, Uwe PAASCH 7, Sven QUIST 8, Berenice M. LANG 9, Rajeev CHAVDA 10 and Wolfgang G. PHILIPP-DORMSTON 11,12
1Knappschaft Kliniken Recklinghausen, Recklinghausen, Germany, 2Galderma Laboratorium GmbH, Düsseldorf, Germany, 3Hautarztpraxis Dr. Hoffmann, Witten, Germany, 4Privatpraxis Dermatologie am Luisenplatz, Potsdam, Germany, 5Dermatologische Praxis Dr. med. Fränken, Schwelm, Germany, 6MVZ Fokus-Haut Corius Koblenz, Koblenz, Germany, 7Hautarztpraxis Hautaerzte-paasch.de, Jesewitz OT Gotha, Germany, 8BAG Drs. Quist, Mainz, Germany, 9Klinik für Dermatologie, Venerologie und Allergologie, Universitätsmedizin Frankfurt, Frankfurt am Main, Germany, 10Galderma SA, Switzerland, 11Hautzentrum Köln (Cologne Dermatology), Köln, Germany, and 12Faculty of Health, University Witten-Herdecke, Witten, Germany
Artificial daylight photodynamic therapy with methyl aminolevulinate is an effective and almost painless treatment approach for actinic keratoses. The objective of the prospective, non-interventional, multicentre study ArtLight (NCT05725213) was to gain comprehensive insights into the cosmetic effect of methyl aminolevulinate-artificial daylight photodynamic therapy in patients with actinic keratoses using different artificial daylight systems under real-world conditions. The study enrolled patients with Olsen grade 1 or 2 actinic keratoses on the face and scalp in Germany. Patients were treated with methyl aminolevulinate-artificial daylight photodynamic therapy. The cosmetic effect was assessed via photodamage parameters (global score for photoaging, mottled pigmentation, tactile roughness, telangiectasias, fine lines). Each photodamage variable was recorded on a 5-point scale (0–4). In total, 224 patients (median age: 75.0 years [range 50–91], 85.3% male, 62.5% Olsen grade 2, 55.4% treatment-naive) were treated with methyl aminolevulinate-artificial daylight photodynamic therapy. At month 3, all 5 parameters of photoaging were significantly reduced from baseline (p < 0.001). The majority of patients (81.3%) and investigators (83.6%) rated the cosmetic result as good or very good. Beyond effective eradication of actinic keratoses, field-directed methyl aminolevulinate-artificial daylight photodynamic therapy can improve photoaging symptoms, including tactile roughness, mottled pigmentation, telangiectasis, and fine lines. Thus methyl aminolevulinate-artificial daylight photodynamic therapy provides additional benefits, particularly for patients concerned with cosmetic outcomes during or after treatment.
SIGNIFICANCE
Beyond effective eradication of actinic keratoses, field-directed methyl aminolevulinate-artificial daylight photodynamic therapy can improve photodamage symptoms, including tactile roughness, mottled pigmentation, telangiectasis, and fine lines. Methyl aminolevulinate-artificial daylight photodynamic therapy provides additional benefits, particularly for patients who are concerned with cosmetic outcomes during or after treatment. As the treatment is almost pain-free and has visible effects on cosmetic results and actinic keratosis lesion count, this promotes patients’ satisfaction and adherence.
Key words: actinic keratosis; methyl aminolevulinate; photoaging of skin; photodynamic therapy; telangiectasia.
Citation: Acta Derm Venereol 2025; 105: adv43245. DOI: https://doi.org/10.2340/actadv.v105.43245.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 24, 2025; Accepted after revision: Mar 28, 2025; Published: Apr 22, 2025
Corr: Prof. Dr. med. Rolf-Markus Szeimies, Knappschaft Kliniken Recklinghausen, Dorstener Str. 151, DE-45657 Recklinghausen, Germany. E-mail: Rolf-Markus.Szeimies@knappschaft-kliniken.de
Competing interests and funding: R-MS has received honoraria for lectures from Almirall, Beiersdorf, Galderma, and Pierre Fabre. He is vice-president of the EURO-PDT Society and a member of the German S3 Guideline committee on Actinic Keratosis and Squamous Cell Carcinoma. MB is an employee of Galderma Laboratorium GmbH, Germany. MH has received consulting fees from Almirall, Galderma, and Dermasence. He has received honoraria for lectures, presentations, speakers’ bureaux, manuscript writing, or educational events from Galderma, Biofrontera, and L’Oréal. He has received support for attending meetings and/or travel from Galderma and Biofrontera. He has received payment for participation on advisory boards from Dermasence, Almirall, Galderma, L’Oréal, and Biofrontera. He has received equipment from Galderma, L’Oréal, Biofrontera, and Dermasence. MB has no conflicts of interests to disclose. JF has received speakers’ honoraria and participated in clinical trials of the following companies: Almirall, Leo Pharma, Abbvie, Galderma, and Janssen. BG has received institutional payment for participation on advisory boards from Galderma. UP has received equipment from Fotona, GME Medical, Alma Lasers, Zimmer, Canfield, FotoFinder, research grants from Zimmer; and consulting fees/speaker honorarium from Alma Lasers, Fotona, Landsberg, Galderma, DDL, DGPRAEC, and Quintessenz publishing. SQ has been an adviser and/or received speakers’ honoraria and/or participated in clinical trials for the following companies: Almirall (adviser, speaker, clinical trials), Galderma (speaker), Leo Pharma (adviser, speaker, clinical trial), Pierre Fabre (clinical trial). BML has been an adviser and/or received speaker’s honoraria from the following companies: Galderma, Biofrontera, Pierre Fabre, Almirall, and L’Oréal. RC is an employee of Galderma SA, Switzerland. WGP-D has been an adviser and/or received speaker’s honoraria and/or received grants and/or participated in clinical trials for the following companies: Almirall, Biofrontera, Galderma, German Medical Engineering, Leo Pharma, Photonamic, Pierre Fabre, and Schulz und Böhm. He is a certified specialist of the Euro-PDT.
The study was financially supported by Galderma Laboratorium GmbH, Düsseldorf, Germany and Galderma SA, Switzerland. Medical writing assistance was provided by Dr Petra Jöstingmeyer (med:unit GmbH, Germany) and was funded by Galderma Laboratorium GmbH, Düsseldorf, Germany and Galderma SA, Switzerland. The authors had full editorial control of the manuscript and provided their final approval.
INTRODUCTION
Actinic keratoses (AK) are keratinocyte neoplasms following long-term exposure to ultraviolet (UV) radiation (1). Whereas UVB plays a major role in skin cancer by exerting its primary effect on the epidermis, causing sunburn and inflammation, UVA contributes significantly to photodamage by deep penetration into the dermis (2–4). As a consequence of these UV effects, AK present as rough scaly patches arising on the skin that can potentially evolve into invasive and metastatic cutaneous squamous cell carcinoma (SCC), if left untreated (5, 6). The cosmetic appearance of photodamaged skin, which includes visible signs of photoaging, such as rough skin texture, fine lines, coarse wrinkles, telangiectasias, and mottled pigmentation, often affects patients’ self-esteem (7). In particular, the presence of telangiectasias has been associated with development of severe AK (8). An ideal treatment should therefore eradicate AK to prevent the progression to skin cancer and simultaneously reverse photodamage. The cosmetic improvement of the skin in AK patients following the alleviation of photodamage symptoms, such as lines, mottled pigmentation, and telangiectasias, is considered an overall indicator of the response to therapy (9). Thus, assessing the cosmetic effect is important, to gain insight into the impact of disease burden and treatment effects in patients with AK, which may not be fully captured by traditional, validated endpoints, such as lesion count.
Among various available treatment options, non-invasive field-directed treatments, including photodynamic therapy (PDT), have proved to be efficient in managing multiple AKs in a contiguous area (10). PDT targets subclinical lesions in chronically UV-damaged skin areas as well, while healthy cells are left largely intact (11). Before PDT was approved for the treatment of AK, its rejuvenating effects were observed in several studies (12, 13). Marked improvement of skin ageing signs following conventional PDT (cPDT) was initially described in 2002 (12). As cPDT was associated with elevated levels of procedural pain during the irradiation, performing PDT in daylight (DL-PDT) turned out to be more tolerable with comparable photo-rejuvenating effects (14–16). In order to enable PDT application all year round and under controlled conditions, artificial daylight PDT (ADL-PDT) using certified light sources has been established in clinical routine. A split-face study demonstrated cosmetic outcomes with ADL-PDT comparable to those achieved with cPDT (17). There is substantial literature supporting the use of PDT with either aminolevulinic acid (ALA) or its methyl ester methyl aminolevulinate (MAL) as photosensitizer in the treatment of AK. During PDT, the photosensitizer is selectively absorbed by photodamaged skin cells, whereby the lipophilic character of MAL enhances its ability to penetrate tissues and increases its target-cell specificity (18, 19). At the time the present study was initiated, MAL was the only photosensitizer approved for ADL-PDT in Germany.
There is a lack of systematic observations under real-life conditions to assess the effectiveness and safety of the different available light sources approved for MAL-ADL-PDT in Germany. Therefore, the aim of this non-interventional study (NIS), ArtLight, was to generate real-world data on the use of MAL with various approved ADL lamp systems in a large patient cohort in order to gain comprehensive insights into the practicability in daily routine. MAL-ADL-PDT was safe and effective. Three months after treatment, lesion counts were reduced in the focus area by 71% (p < 0.001) and the median AKASI decreased from 6.2 at baseline to 3.4 at month 3 (95% confidence interval 2.4–3.0; p < 0.001). Nearly all patients (93.3%) experienced no or mild pain during PDT (numeric rating scale score 0–3) and no new safety signals were reported (20). Here we focus on the cosmetic effect assessed as improvement of photodamage parameters.
MATERIALS AND METHODS
Study design
Study design, eligibility criteria, and study procedures have been described previously (20). In brief, the effect of ADL-PDT with MAL on photodamage in patients with AK was evaluated in a multicentre, open-label, prospective non-interventional observational cohort study conducted (according to § 4 (23) and § 67 (6) German drug law) in 38 dermatology centres in Germany between November 2022 and October 2023. The study protocol was reviewed by the ethics committee of the Westphalia-Lippe Medical Association and the Westphalian Wilhelms University of Münster (ref no. 2022-488-f-S) prior to the study’s commencement. The data collection was conducted in compliance with the current version of the Declaration of Helsinki, as well as guidelines and recommendations for safeguarding Good Epidemiological Practice, and other applicable regulations and laws. No additional diagnostic measures beyond routine clinical practice were required. MAL-ADL-PDT using 160 mg/g MAL cream was performed at the baseline visit in accordance with the regular treatment routine and the treatment recommendations in the summary of product characteristics (SmPC). To assess outcome parameters, follow-up documentation was scheduled 3 months after treatment.
Study population
Adult patients with a confirmed diagnosis of thin or non-hyperkeratotic and non-pigmented AK (Olsen grade 1 or 2) on the face or scalp were selected from dermatology practices when MAL-ADL-PDT was indicated, and the decision to undergo MAL-ADL-PDT was made independently of this study. Exclusion criteria were skin cancers or precursors other than AK of Olsen type I and II.
Assessments
Detailed effectiveness and safety parameters have been published separately (20). The cosmetic effect was assessed as improvement of photodamage parameters (global score for photoaging, mottled pigmentation, tactile roughness, telangiectasias, fine lines). Each photodamage variable was recorded on a 5-point scale (0–4), where higher points indicate higher damage, according to Karrer et al. (15). For evaluation of the global score for photoaging, the entire face and scalp were taken into account. Mottled pigmentation, tactile roughness, telangiectasias, and fine lines were assessed within a pre-specified focus area, covering 10 x 10 cm of the treated area. Optional photo documentation was performed at baseline and month 3. Both the investigators and patients rated their satisfaction with regard to the cosmetic result on a 5-point Likert scale (very good, good, satisfied, unsatisfied, very unsatisfied) at month 3 and, for patients who received a second treatment, month 6.
Statistical analysis
The sample size of the study population was determined by the number of eligible patients who agreed to participate in the observation. All documented data were analysed descriptively. For continuous variables (size, age, time periods, etc.), the statistical parameters (mean, standard deviation, median, minimum, maximum, interquartile range, total number) were listed. Discrete variables were categorized in the form of frequency distributions and listed as a percentage of the total sample. Exploratory analyses were carried out to investigate the change in skin quality parameters, which was determined using the Wilcoxon test. All tests were two-sided and significance was declared at the 0.05 level. Imputation methods (such as Last Observation Carried Forward) were generally not used for missing data. All statistical analyses were performed with the SPSS program package (version 22.0, IBM Deutschland GmbH, Ehningen, Germany).
RESULTS
In total, 224 patients (median age: 75.0 years [range 50–91], 85.3% male, 62.5% AK Olsen grade 2, 55.4% treatment-naive) were included in the study and treated with MAL-ADL-PDT. At baseline, the median scores for photodamage parameters were 2.0 (range 0–4) for global photoaging score, mottled pigmentation, telangiectasia, and fine lines, respectively, and 3.0 (range 1–4) for tactile roughness. At month 3, 215 patients were available for the efficacy analysis.
Photodamage
At month 3, all 5 parameters of photodamage (global photoaging score, tactile roughness, mottled pigmentation, telangiectasia, fine lines) were significantly reduced from baseline (p < 0.001) as illustrated by the shift in the interquartile range (Fig. 1, Table I). Fig. 2 shows an example of 3 patients from different study sites with improved photoaging parameters at month 3 compared with baseline. In patient A the global photoaging score changed from 2 to 1, tactile roughness from 2 to 1, mottled pigmentation from 3 to 0, telangiectasia from 2 to 1, and fine lines from 3 to 1 (Fig. 2a). In patient B the score for mottled pigmentation changed from 4 to 3, the score for telangiectasia also from 4 to 3, and fine lines from 4 to 2. The global photoaging score and the score for tactile roughness remained stable at 3 (Fig. 2b). In patient C the score for tactile roughness changed from 3 to 2, the scores for mottled pigmentation, fine lines, and the global photoaging score remained stable at 2. The score for telangiectasia remained stable at 3 (Fig. 2c). Additional patient images have been published previously (20).
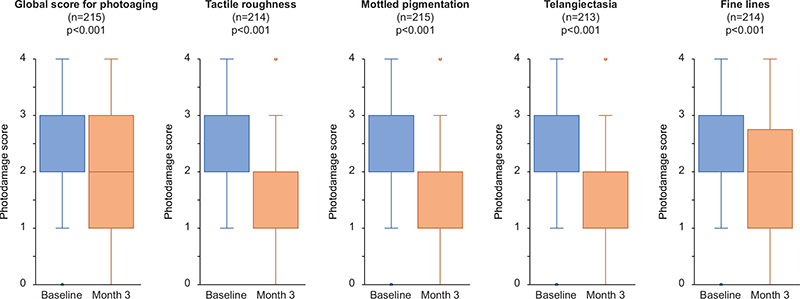
Fig. 1. Changes in photodamage parameters. Boxes indicate first quartile, median, and third quartile. Whiskers indicate minimum and maximum data points within the 1.5 interquartile range. Outliers are plotted as dots. Numbers in boxes indicate the median.
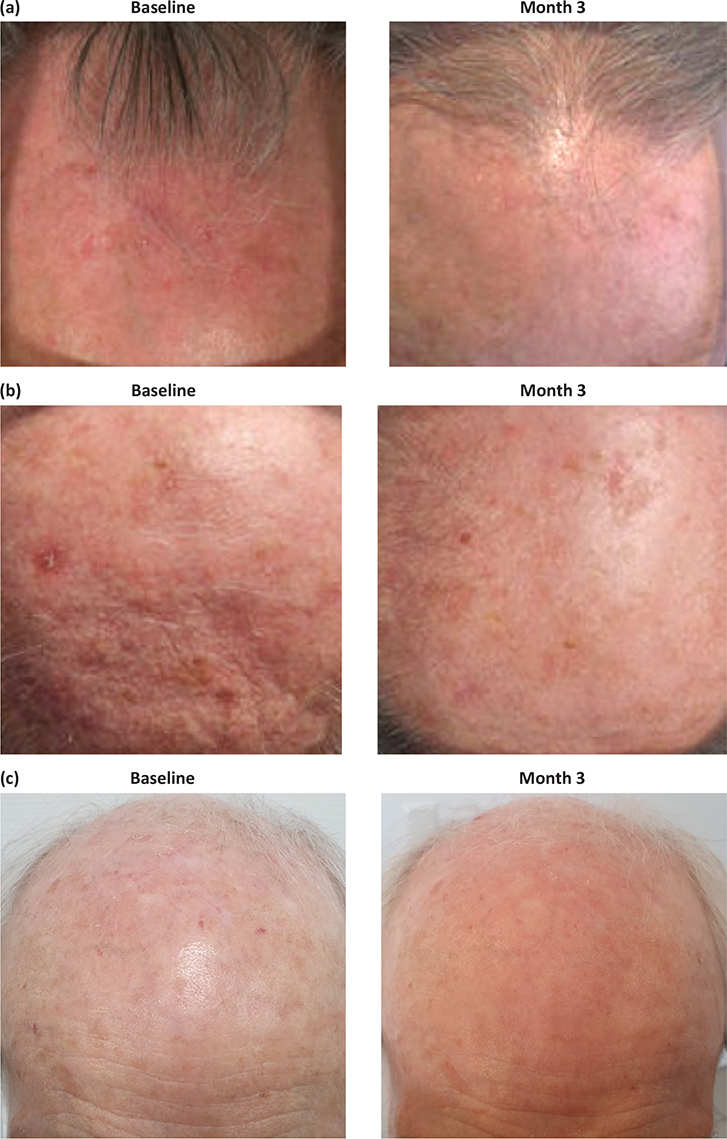
Fig. 2. Photo documentation of three patients with improvements in photoaging parameters from baseline to month 3.
Twenty-two patients (10.2%) received a second treatment. In the 16 patients evaluable 3 months after the second treatment, further improvement was observed in all 5 parameters of photodamage (Table II).
Satisfaction with cosmetic result
Three months after the initial treatment, the majority of patients (81.3%) and investigators (83.6%) rated the cosmetic result as good or very good. Among those receiving a second treatment, 68.8% of patients and more investigators (80.0%) rated the cosmetic results 3 months after the second treatment as good or very good (Fig. 3).
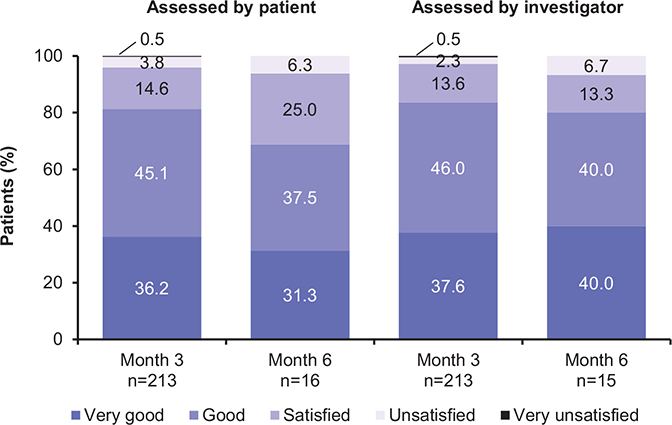
Fig. 3. Satisfaction with cosmetic result rated by patients and investigators.
DISCUSSION
The non-interventional study ArtLight currently represents the largest study that focuses on skin rejuvenation with MAL-ADL-PDT applied under real-world conditions for the treatment of AK. Significant improvement was observed in all 5 assessed photodamage parameters. To date, clinical studies have provided only little evidence that ADL-PDT may also reduce facial photodamage. The beneficial effect of cPDT on photodamaged skin has been observed previously in studies on skin rejuvenation (12, 21–24). However, in a population treated for AK, studies investigating the use of cPDT, DL-PDT, or ADL-PDT achieved varying results for photodamage parameters, depending on protocol, pretreatment, and lamp systems (14, 15). In a randomized split-face trial investigating MAL-ADL-PDT vs cPDT in 40 patients, effects on photoaging were observed with both applications, but, contrary to presented results, they were limited to erythema and tactile roughness (17). A significant reduction in signs of photoaging including fine lines, pigmentation, roughness, erythema, and sebaceous gland hyperplasia was observed after MAL-DL-PDT (15). In a small trial with 18 patients, the use of ALA-PDT with blue light led to significant improvement in skin quality, fine lines, and skin complexion; however, deep wrinkles and mottled pigmentation did not improve (25). To the best of our knowledge, ArtLight is the first study on MAL-ADL-PDT for AK showing significant reductions in telangiectasias, the presence of which has been associated with development of severe AK (8).
The cosmetic effect noticeable as reversal of photodamage results from improvement in the density and arrangement of collagen and elastic fibres in photodamaged skin (26). Collagen is upregulated as a consequence of the PDT-induced synthesis of keratinocyte-derived cytokines, which penetrate the basal layer of the epidermis and enhance dermal collagen metabolism (27, 28). In addition, increased epidermal proliferation along with a reduction of abnormal elastin in the dermis has been observed (29, 30). Examined underlying genetic changes included decreased expression of Ki-67, a marker of proliferation and of p53, a marker of early skin carcinogenesis (31). Thus, the observed improved tactile roughness and mottled pigmentation results from a direct effect of PDT on epidermal reorganization, while a secondary indirect cytokine-mediated dermal effect on fibroblast stimulation, elastolysis, and neocollagenesis resulting in collagen remodelling is responsible for the improvement seen in fine lines (28, 32). Neocollagenesis in the subepidermal layer leads to a compression of the telangiectatic vessels towards the deep dermis, thus resulting in the observed improvement of telangiectasias on the skin surface (28).
For the indication of AK, a single application of PDT achieved a satisfactory response in terms of lesion reduction. For cosmetic indications, studies found that a single treatment is not always sufficient (13). Whereas 1 application of PDT already resulted in significant photodamage reversal, conducting a second PDT confirmed further improvement of photodamage parameters compared with baseline. In terms of satisfaction with cosmetic result, there is a gap between patients and investigators’ rating for the repeated treatment at month 6. Patients may expect faster or more dramatic results, while investigators assess progress more clinically. A small retrospective study analysing ALA-PDT for AK indicated effective alleviation of photodamage over a 2-year follow-up period (33). Whether the improvement in photodamage by MAL-ADL-PDT is a long-term effect remains to be investigated in future studies with longer follow-up periods.
Overall, assessing cosmetic outcomes in the treatment of AK is important, particularly for facial or visible lesions, as poor cosmetic results may impact patient satisfaction and adherence to follow-up care. However, given that some patients with AK may generally prioritize efficacy over aesthetics, the significance of cosmetic outcomes should not be underestimated.
In addition to the beneficial effect on photodamage, MAL-ADL-PDT using different artificial illumination systems resulted in significantly reduced lesion counts and AKASI scores as well as high patient satisfaction with treatment, effectiveness, time investment, and aesthetics. The procedure was almost pain-free with the majority of patients reporting no or mild procedural pain. No new safety signals were reported. Detailed effectiveness and safety results have been published previously (20).
The study is limited by its non-controlled real-world setting, which may be obscured by unknown confounders in patient cohorts. The strength of the study is the use of an objective score to assess parameters of photodamage, with a distinctive description assigned to each score point in order to minimize error (15). As only a few patients were lost to follow-up, 3-month assessments were based on a solid sample size, contributing to the robustness of the reported results. To mitigate limitations such as enrolment bias, where participant differences may skew results, and information bias, arising from data inaccuracies, strategies such as standardized data collection and rigorous quality checks were employed. Although the demographic makeup of the ArtLight population is similar to common AK populations (17, 34, 35), its setting in Germany may limit generalizability to other regions.
In conclusion, beyond effective eradication of AK, field-directed MAL-ADL-PDT can improve photodamage symptoms, including tactile roughness, mottled pigmentation, telangiectasis, and fine lines. Thus, MAL-ADL-PDT provides additional benefits, particularly for patients who are concerned with cosmetic outcomes during or after treatment. As the treatment is almost pain-free and has visible effects on cosmetic results and AK lesion count, this promotes patients’ satisfaction and adherence. Consequently, about 90% of participants would consider using MAL-ADL-PDT again if needed (20).
ACKNOWLEDGEMENTS
IRB approval status: The study protocol was reviewed by the ethics committee of the Westphalia-Lippe Medical Association and the Westphalian Wilhelms University of Münster, Germany (ref no. 2022-488-f-S) prior to the study’s commencement.
REFERENCES
- Eisen DB, Asgari MM, Bennett DD, Connolly SM, Dellavalle RP, Freeman EE, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol 2021; 85: e209–e233. https://doi.org/10.1016/j.jaad.2021.02.082
- Yaar M, Gilchrest BA. Photoageing: mechanism, prevention and therapy. Br J Dermatol 2007; 157: 874–887. https://doi.org/10.1111/j.1365-2133.2007.08108.x
- Benjamin CL, Ullrich SE, Kripke ML, Ananthaswamy HN. p53 tumor suppressor gene: a critical molecular target for UV induction and prevention of skin cancer. Photochem Photobiol 2008; 84: 55–62. https://doi.org/10.1111/j.1751-1097.2007.00213.x
- Schwarz T. 25 years of UV-induced immunosuppression mediated by T cells-from disregarded T suppressor cells to highly respected regulatory T cells. Photochem Photobiol 2008; 84: 10–18. https://doi.org/10.1111/j.1751-1097.2007.00223.x
- Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg 2007; 33: 1099–1101. https://doi.org/10.1097/00042728-200709000-00010
- Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet 1988; 1: 795–797. https://doi.org/10.1016/S0140-6736(88)91658-3
- Abrouk M, Gianatasio C, Li Y, Waibel JS. Prospective study of intense pulsed light versus pulsed dye laser with or without blue light in the activation of PDT for the treatment of actinic keratosis and photodamage. Lasers Surg Med 2022; 54: 66–73. https://doi.org/10.1002/lsm.23492
- George CD, Tokez S, Hollestein L, Pardo LM, Keurentjes AJ, Wakkee M, et al. Longitudinal assessment of the prevalence of actinic keratosis and extensive risk factor evaluation: an update from the Rotterdam Study. J Invest Dermatol 2023; 143: 2193–2203.e2112. https://doi.org/10.1016/j.jid.2023.02.042
- Szeimies RM, Gerritsen MJ, Gupta G, Ortonne JP, Serresi S, Bichel J, et al. Imiquimod 5% cream for the treatment of actinic keratosis: results from a phase III, randomized, double-blind, vehicle-controlled, clinical trial with histology. J Am Acad Dermatol 2004; 51: 547–555. https://doi.org/10.1016/j.jaad.2004.02.022
- Stockfleth E. The importance of treating the field in actinic keratosis. J Eur Acad Dermatol Venereol 2017; 31: 8–11. https://doi.org/10.1111/jdv.14092
- Philipp-Dormston WG, Aschoff R, von Braunmühl T, Eigentler T, Haalck T, Thoms KM. [Decision criteria and patient characteristics for patient-oriented treatment of field cancerization: standardized algorithm for personalized treatment concepts]. Hautarzt 2021; 72: 314–320. https://doi.org/10.1007/s00105-020-04731-y
- Ruiz-Rodriguez R, Sanz-Sánchez T, Córdoba S. Photodynamic photorejuvenation. Dermatol Surg 2002; 28: 742–744; discussion 744. https://doi.org/10.1046/j.1524-4725.2002.02018.x
- Szeimies RM, Lischner S, Philipp-Dormston W, Walker T, Hiepe-Wegener D, Feise K, et al. Photodynamic therapy for skin rejuvenation: treatment options – results of a consensus conference of an expert group for aesthetic photodynamic therapy. J Dtsch Dermatol Ges 2013; 11: 632–636. https://doi.org/10.1111/ddg.12119
- Bento CO, Pantaleão L, de Souza MB, Vilar EAG, Luiz RR, Filho PJS, et al. Comparison of clinical and histologic findings in daylight photodynamic therapy for skin field cancerization: a randomized controlled four-arm study on physical methods-assisted delivery of methyl aminolevulinate. Photodiagnosis Photodyn Ther 2021; 35: 102404. https://doi.org/10.1016/j.pdpdt.2021.102404
- Karrer S, Szeimies RM, Philipp-Dormston WG, Gerber PA, Prager W, Datz E, et al. Repetitive daylight photodynamic therapy versus cryosurgery for prevention of actinic keratoses in photodamaged facial skin: a prospective, randomized controlled multicentre two-armed study. Acta Derm Venereol 2021; 101: adv00355. https://doi.org/10.2340/00015555-3717
- Trave I, Salvi I, Serazzi FA, Schiavetti I, Luca L, Parodi A, et al. The impact of occlusive vs non-occlusive application of methyl aminolevulinate on the efficacy and tolerability of daylight photodynamic therapy for actinic keratosis. Photodiagnosis Photodyn Ther 2024; 46: 104049. https://doi.org/10.1016/j.pdpdt.2024.104049
- Arisi M, Rossi MT, Spiazzi L, Guasco Pisani E, Venturuzzo A, Rovati C, et al. A randomized split-face clinical trial of conventional vs indoor-daylight photodynamic therapy for the treatment of multiple actinic keratosis of the face and scalp and photoaging. J Dermatolog Treat 2022; 33: 2250–2256. https://doi.org/10.1080/09546634.2021.1944594
- Gold MH. Therapeutic and aesthetic uses of photodynamic therapy part five of a five-part series: ALA-PDT and MAL-PDT what makes them different. J Clin Aesthet Dermatol 2009; 2: 44–47.
- Henderson BW, Dougherty TJ. How does photodynamic therapy work? Photochem Photobiol 1992; 55: 145–157. https://doi.org/10.1111/j.1751-1097.1992.tb04222.x
- Philipp-Dormston WG, Brückner M, Hoffmann M, Baé M, Fränken J, Großmann B, et al. Artificial daylight photodynamic therapy using methyl aminolaevulinate in a real-world setting in Germany: results from the noninterventional study ArtLight. Br J Dermatol 2025; 192: 510–519. https://doi.org/10.1093/bjd/ljae437
- Piccioni A, Fargnoli MC, Schoinas S, Suppa M, Frascione P, Ginebri A, et al. Efficacy and tolerability of 5-aminolevulinic acid 0.5% liposomal spray and intense pulsed light in wrinkle reduction of photodamaged skin. J Dermatolog Treat 2011; 22: 247–253. https://doi.org/10.3109/09546634.2011.590791
- Sanclemente G, Medina L, Villa JF, Barrera LM, Garcia HI. A prospective split-face double-blind randomized placebo-controlled trial to assess the efficacy of methyl aminolevulinate + red-light in patients with facial photodamage. J Eur Acad Dermatol Venereol 2011; 25: 49–58. https://doi.org/10.1111/j.1468-3083.2010.03687.x
- Karrer S, Kohl E, Feise K, Hiepe-Wegener D, Lischner S, Philipp-Dormston W, et al. Photodynamic therapy for skin rejuvenation: review and summary of the literature – results of a consensus conference of an expert group for aesthetic photodynamic therapy. J Dtsch Dermatol Ges 2013; 11: 137–148. https://doi.org/10.1111/j.1610-0387.2012.08046.x
- Philipp-Dormston WG. Photodynamic therapy for aesthetic-cosmetic indications. G Ital Dermatol Venereol 2018; 153: 817–826. https://doi.org/10.23736/S0392-0488.18.05982-5
- Touma D, Yaar M, Whitehead S, Konnikov N, Gilchrest BA. A trial of short incubation, broad-area photodynamic therapy for facial actinic keratoses and diffuse photodamage. Arch Dermatol 2004; 140: 33–40. https://doi.org/10.1001/archderm.140.1.33
- Ji J, Zhang LL, Ding HL, Wang HW, Huang Z, Wang XX, et al. Comparison of 5-aminolevulinic acid photodynamic therapy and red light for treatment of photoaging. Photodiagnosis Photodyn Ther 2014; 11: 118–121. https://doi.org/10.1016/j.pdpdt.2014.02.007
- Park MY, Sohn S, Lee ES, Kim YC. Photorejuvenation induced by 5-aminolevulinic acid photodynamic therapy in patients with actinic keratosis: a histologic analysis. J Am Acad Dermatol 2010; 62: 85–95. https://doi.org/10.1016/j.jaad.2009.06.025
- Szeimies RM, Torezan L, Niwa A, Valente N, Unger P, Kohl E, et al. Clinical, histopathological and immunohistochemical assessment of human skin field cancerization before and after photodynamic therapy. Br J Dermatol 2012; 167: 150–159. https://doi.org/10.1111/j.1365-2133.2012.10887.x
- Issa MC, Piñeiro-Maceira J, Vieira MT, Olej B, Mandarim-de-Lacerda CA, Luiz RR, et al. Photorejuvenation with topical methyl aminolevulinate and red light: a randomized, prospective, clinical, histopathologic, and morphometric study. Dermatol Surg 2010; 36: 39–48. https://doi.org/10.1111/j.1524-4725.2009.01385.x
- Orringer JS, Hammerberg C, Hamilton T, Johnson TM, Kang S, Sachs DL, et al. Molecular effects of photodynamic therapy for photoaging. Arch Dermatol 2008; 144: 1296–1302. https://doi.org/10.1001/archderm.144.10.1296
- Bagazgoitia L, Cuevas Santos J, Juarranz A, Jaén P. Photodynamic therapy reduces the histological features of actinic damage and the expression of early oncogenic markers. Br J Dermatol 2011; 165: 144–151. https://doi.org/10.1111/j.1365-2133.2011.10270.x
- Zane C, Capezzera R, Sala R, Venturini M, Calzavara-Pinton P. Clinical and echographic analysis of photodynamic therapy using methylaminolevulinate as sensitizer in the treatment of photodamaged facial skin. Lasers Surg Med 2007; 39: 203–209. https://doi.org/10.1002/lsm.20470
- Zhang L, Zhao Z, Wang P, Zhang G, Wang B, Shi L, et al. Long-term improvement on photoaging after ALA photodynamic therapy for actinic keratosis: a retrospective study. Photodiagnosis Photodyn Ther 2021; 33: 102181. https://doi.org/10.1016/j.pdpdt.2021.102181
- Fargnoli MC, Ibbotson SH, Hunger RE, Rostain G, Gaastra MTW, Eibenschutz L, et al. Patient and physician satisfaction in an observational study with methyl aminolevulinate daylight photodynamic therapy in the treatment of multiple actinic keratoses of the face and scalp in six European countries. J Eur Acad Dermatol Venereol 2018; 32: 757–762. https://doi.org/10.1111/jdv.14691
- Philipp-Dormston WG, Müller K, Novak B, Strömer K, Termeer C, Hammann U, et al. Patient-reported health outcomes in patients with non-melanoma skin cancer and actinic keratosis: results from a large-scale observational study analysing effects of diagnoses and disease progression. J Eur Acad Dermatol Venereol 2018; 32: 1138–1146. https://doi.org/10.1111/jdv.14703