RESEARCH LETTER
Fibrinogen-like Protein 1 can be a Meaningful Marker Implying Well-differentiated in Cutaneous Squamous Cell Carcinoma
Shin TAEK OH1, Jung MIN BAE2, Hae EUN PARK3, Dong SOO YOO1 and Young MIN PARK1*
1Department of Dermatology, College of Medicine, The Catholic University of Korea, Seoul, 2Heal House Skin Clinic, Suwon, and 3Doctors Dermatology Clinic, Jamsil-Songpa Branch, Seoul, Korea. *E-mail: 96015367@cmcnu.or.kr
Citation: Acta Derm Venereol 2025; 105: adv43248. DOI: https://doi.org/10.2340/actadv.v105.43248.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 25, 2025. Accepted: Apr 29, 2025. Published: Jun 12, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
To the Editor,
Fibrinogen-like protein 1 (FGL1), also known as liver fibrinogen-related gene-1 (LFIRE-1)/hepassocin (HPS) or hepatocyte-derived fibrinogen-related protein-1 (HFREP-1), is a proliferation- and metabolism-related factor secreted by the liver. Recently, FGL1 has become regarded as an emerging checkpoint ligand of lymphocyte activation gene 3 (LAG3), emphasizing the potential of targeting FGL1/LAG3 as the next generation of immune checkpoint therapy (1).
The role of FGL1 in cancer is not clear. It is of interest that FGL1 has both pro- and anti-tumour functions (2). Traditionally, FGL1 has been known to promote tumour progression and metastasis, suggesting its potential as a poor prognostic biomarker (3, 4). It also is known that disruption of FGL1 accelerates hepatocellular carcinoma development, suggesting that FGL1 serves as a tumour suppressor. In addition, high FGL1 expression was reported to be associated with better overall survival in hepatocellular carcinoma (3).
FGL1 has been reported to be abnormally expressed in various tumours (2). However, we could not find a report regarding the expression of FGL1 in cutaneous squamous cell carcinoma (cSCC). In the present study, we aimed to investigate the expression of FGL1 according to cSCC differentiation using immunohistochemical staining.
The ethics committee of the Catholic University of Korea approved this study (XC19SEDI0033). Patients provided written informed consent. A total of 86 biopsy specimens collected from the 3 branch hospitals of the Catholic University of Korea were included. Conventional cSCC cases were divided into 3 histological grades according to differentiation: well differentiated, moderately differentiated, and poorly differentiated. Paraffin sections of normal skin (n = 11), actinic keratosis (n = 16), Bowen’s disease (n = 10), and cSCCs (n = 49) (well-differentiated [n = 22], moderately differentiated [n = 14], and poorly differentiated [n = 13]) were analysed for FGL1 expression. Following deparaffinization and hydration, sections were subjected to the VECTASTAIN Elite ABC System and ImmPACT NovaRED (Vector Lab, Burlingame, CA, USA) according to the manufacturer’s recommended procedure. Briefly, sections were incubated for 20 min with normal blocking serum, 1 h with anti-FGL1 antibody (mouse monoclonal FGL1 antibody, 1:50 dilution; R&D Systems, Minneapolis, MN, USA), 30 min with biotinylated secondary antibody, and 30 min with ABC reagent and then developed for 3 min. Microscopic analysis was performed by 2o independent observers (STO and YMP). Statistical analyses were performed using Python (version 3.12; https://www.python.org/downloads/release/python-3120/) with scipy and statsmodels packages.
FGL1 immunoreactivity was detected in the cytoplasm of cSCCs, normal skin, actinic keratosis, and Bowen’s disease (Fig. 1 A–L). Moderate to strong FGL1 immunoreactivity was observed in 31 of 49 specimens (63%) with cSCC (Fig. 1 A–H). In contrast, this immunoreactivity was observed in 0 of 11 specimens (0%) with normal epidermis (Fig.1 I), 1 of 16 specimens (6%) with actinic keratosis (Fig. 1J), and 3 of 10 specimens (30%) with Bowen’s disease (Fig. 1 K, L). According to cSCC differentiation, moderate to strong FGL1 immunoreactivity was observed in 21 of 22 specimens (96%) of well-differentiated cSCC (Fig. 1 A–D). Moderate to strong FGL1 immunoreactivity was observed in 7 of 14 specimens (50%) of moderately differentiated cSCC (Fig. 1 E, F) and in 3 of 13 specimens (23%) of poorly differentiated cSCC (Fig. 1 G, H and Table I). Thus, there was a significant difference in the proportion of FGL1 immunoreactivity according to the degree of cSCC differentiation (p < 0.001) (Table I).
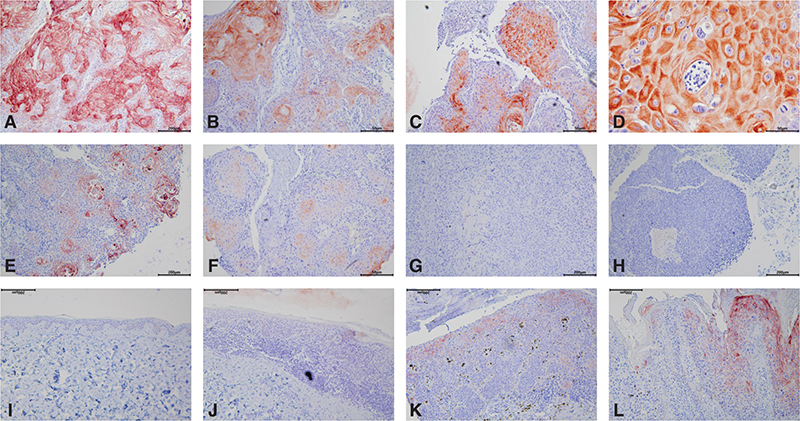
Fig. 1. Fibrinogen-like protein 1 (FGL1) expression in cutaneous squamous cell carcinoma (cSCC) according to histological differentiation. (A–D) Well-differentiated cSCC (×100); strong cytoplasmic expression of FGL1. (D) Magnified view of arrow in C (×400), (E, F) Moderately differentiated cSCC (×100); focal cytoplasmic FGL1 expression. (G, H) Poorly differentiated cSCC (×100); negative FGL1 expression I. Normal epidermis (×100); negative expression of FGL1. (J) Actinic keratosis (×100); negative expression of FGL1. (K, L) Bowen’s disease (×100); focal cytoplasmic expression of FGL1.
| Factor | Expression of FGL1 | p-value | ||||
| 0 | + | ++ | +++ | |||
| Normal skin (n = 11) | 7 | 4 | 0 | 0 | Reference | |
| Actinic keratosis (n = 16) | 8 | 7 | 1 | 0 | 0.034* | |
| Bowen’s disease (n = 10) | 4 | 3 | 2 | 1 | 0.003* | |
| Total cSCC (n = 49) | 11 | 7 | 11 | 20 | < 0.001* | |
| Subtype | Well differentiated cSCC (n = 22) | 0 | 1 | 2 | 19 | < 0.001** |
| Moderately differentiated cSCC (n = 14) | 3 | 4 | 6 | 1 | ||
| Poorly differentiated cSCC (n = 13) | 8 | 2 | 3 | 0 | ||
| The degree of staining intensity was graded semi-quantitatively as follows: 0: no staining; +: weak staining intensity; ++: moderate staining intensity; +++: strong staining intensity. *Mann–Whitney U tests were conducted to compare normal epidermis, actinic keratosis, Bowen’s disease, and total cSCC. **Kruskal–Wallis test was performed to compare FGL1 expression among cSCC differentiation groups. |
||||||
In a pilot study, we tried to measure the expression of LAG3 in cSCC by immunohistochemistry, but we could not find any significant expression or any significant difference according to differentiation (data not shown; LAG3 Rabbit mAb #15372 [Cell Signaling Technology, Danvers, MA, USA], 1:50 titration and LAG3 Rabbit mAb #180187 [Abcam, Cambridge, UK], 1:50 titration).
To our knowledge, no report has examined the expression of FGL1 in cSCC. Based on our results, we could find a significant difference in the proportion of FGL1 immunoreactivity according to the degree of cSCC differentiation: the proportion of FGL1 immunoreactivity was much greater in well-differentiated cSCC. Therefore, FGL1 may participate in the formation of well-differentiated cSCC. Further functional research on the role of FGL1 in well-differentiated cSCC is needed.
ACKNOWLEDGEMENTS
IRB approval status: The ethics committee of The Catholic University of Korea approved this study (XC19SEDI0033).
REFERENCES
- Qian W, Zhao M, Wang R, Li H. Fibrinogen-like protein 1 (FGL1): the next immune checkpoint target. J Hematol Oncol 2021: 14: 147. https://doi.org/10.1186/s13045-021-01161-8
- Yu J, Li J, Shen J, Du F, Wu X, Li M, et al. The role of fibrinogen-like proteins in cancer. Int J Biol Sci 2021; 17: 1079–1087. https://doi.org/10.7150/ijbs.56748
- Zhang Y, Qiao HX, Zhou YT, Hong L, Chen JH. Fibrinogen-like-protein 1 promotes the invasion and metastasis of gastric cancer and is associated with poor prognosis. Mol Med Rep 2018; 18: 1465–1472. https://doi.org/10.3892/mmr.2018.9097
- Liu TY, Yan JS, Li X, Xu L, Hao JL, Zhao SY, et al. FGL1: a novel biomarker and target for non-small cell lung cancer, promoting tumor progression and metastasis through KDM4A/STAT3 transcription mechanism. J Exp Clin Cancer Res 2024; 43: 213. https://doi.org/10.1186/s13046-024-03140-6