Lichen sclerosus (LS) is a chronic inflammatory skin disease affecting mainly female and male genital skin, and, in women, the perianal area also. LS causes intense itching and scarring, and may lead to malignant transformation (1). The prevalence of LS has been estimated to be up to 3.1% in elderly women (2). In women, especially, LS has been linked to several autoimmune conditions (1).
In this study, the prevalence of diseases in female patients diagnosed with LS was compared with that in a female patient cohort without LS, in order to study possible co-morbidities. Gynaecological, urological, and gastrointestinal diseases, and malignant co-morbidities, are to be discussed in a separate publication (no data available).
MATERIALS AND METHODS
Patients
Female patients with a diagnosis of LS were identified by searching for International Classification of Diseases 10 (ICD-10) code L90.0 for the period 1 January 2004 to 31 December 2012, in hospital patient data in Turku University Hospital in Southwest Finland. Any diagnosis with at least one patient with LS was included in the study. For each patient with LS, 10 control patients of the same sex and birth year, but with no diagnosis of LS, were randomly selected from the Turku University Hospital patient register. Approximately 250,000 female persons live in this hospital district.
This study was approved by Turku University Hospital Clinical Research Center (study number T48/2014).
Statistical analysis
The relative risks (RRs), 95% confidence intervals (95% CIs), and p-values for each diagnosis were calculated using Pearson’s χ2 test. The first occurrence of the LS diagnosis code in the electronic health records was chosen as the index date from which the patient age was calculated. Patients with LS were excluded from the control population. All statistical tests were 2-tailed, and p < 0.05 was considered statistically significant. Statistical analyses were performed using R Statistics version 3.0.2 (Free Software Foundation, Boston, MA, USA).
RESULTS AND DISCUSSION
A total of 455 female patients with LS were identified, giving a prevalence of 1.8:1000. The diagnosis was solely clinical or, in 196 patients, also confirmed with a skin biopsy. Mean age at the time of diagnosis of LS of the patients was 64.4 years (age range 6–104 years). Statistically significant results are shown in Table I.
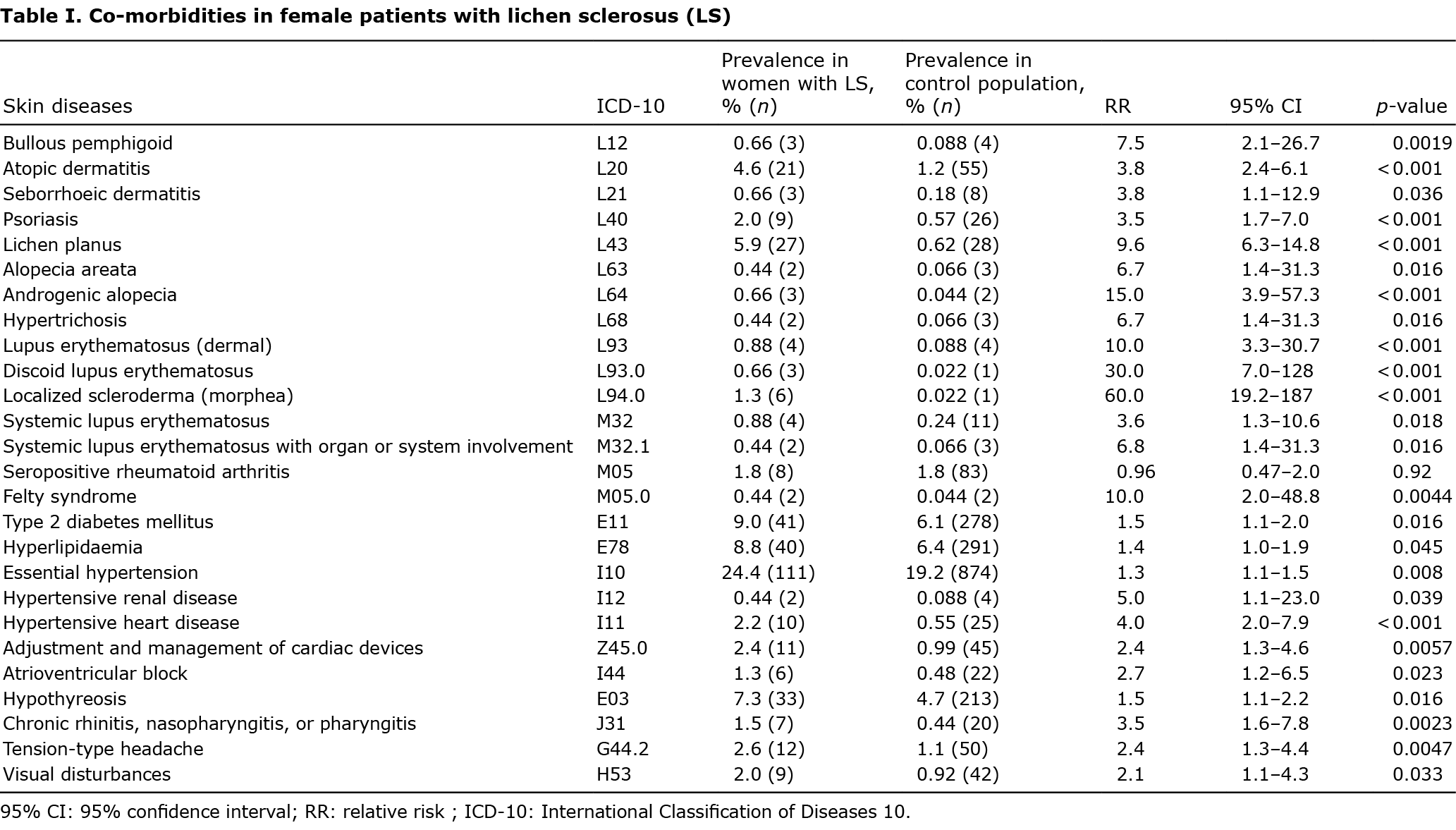
Skin diseases. In accordance with previous studies, atopic eczema and psoriasis were more common among patients with LS (3, 4). It has been hypothesized that LS and atopy might share a common immunological defect, or that LS might develop on top of atopically disturbed skin (5). The prevalence of psoriasis in the current study was 2.0% (RR 3.5), which is in line with previous studies showing a prevalence of 0.8–17% (3, 6–8, Table SI). In both LS and psoriasis, T-cells are activated and are believed to be involved in the pathogenesis of both conditions (9).
In the current study, 1.3% of patients with LS had morphea (RR 60.0), but none had systemic sclerosis. The association of LS and morphea (local dermal scleroderma) is well established. In studies concerning female patients with LS, 1.5–4.5% have morphea (3, 7, Table SI). The only study showing association of LS and systemic sclerosis presented 79 patients with systemic scleroderma, of whom 8% had LS, all of them women with limited cutaneous systemic scleroderma (10).
Lichen planus was found to be more common among patients with LS (5.9%, RR 9.6) in the current study. The prevalence of lichen planus among patients with LS has been studied in only 1 prior article, in which the prevalence of lichen planus was 2.5% (3). The prevalence of bullous pemphigoid in the current study was 0.66% (RR7.5), similar to a previous study (11).
According to the results of the current study, 0.44% of patients had alopecia areata. In previous studies, 0–9.0% of female patients with LS have had alopecia areata (3, 6, 11, Table SI). Male-type hair loss and hypertrichosis were also more common among female patients with LS in the current study (RR 15.0 and 6.7, respectively). There are no previous reports on hair loss or hypertrichosis.
Connective tissue diseases. The risk of systemic lupus erythematosus (SLE) was increased in the current patient cohort among patients with LS (RR 3.6); especially, the risk of SLE with organ or system involvement was increased (RR 6.7). There are few data available on the association of SLE with LS, and only a few case reports have been published.
In accordance with the previous studies, the risk of rheumatoid arthritis was not increased among patients with LS in the current study (RR 0.96). However, Felty syndrome, in which patients with rheumatoid arthritis also develop neutropaenia and splenomegaly, was more common among patients with LS (RR 10.0). In both LS and Felty syndrome the regulation of inflammatory processes is altered, but neither a specific molecular basis nor a clinical connection between the 2 diseases has been published previously.
Metabolic syndrome and heart diseases. The current study showed that 9.0% of female patients had type 2 diabetes compared with 6.1% among control patients (RR 1.5). Among female patients with LS, metabolic syndrome diseases have been studied only by Sideri et al. (12), who did not find an association; Virgili et al. (4), who found hypertension and overweight (body mass index ≥ 25 kg/m2) to be more common among a combined group of female and male patients with LS (age-standardized prevalence ratio 1.44 and 1.22, respectively); and Higgins & Cruickshank (6), who found 3.3% of female patients with LS to have type 2 diabetes compared with none among control patients. Patients with LS also had an increased risk of hyperlipidaemia (RR 1.4), hypertension (RR 1.3), and hypertensive kidney disease (RR 5.0).
Diagnoses of atrioventricular block and adjusting pacemaker, suggesting a background conductive heart disease, were also more common in those with LS than in controls (RR 2.7 and 2.7, respectively). We did not find any publications about conduction defects related to LS. In lupus erythematosus, conduction defects have been reported, but are uncommon (13). The aetiology is unclear, but the effects of autoantibodies reacting with the conduction system, myocardial disease, and adverse effects of antimalarials have all been suggested as a cause (13). Autoantibodies might also be related to conduction defects in LS.
Endocrinological diseases. The prevalence of hypothyreosis among the patients with LS in this study was 7.3% (RR 1.5). Goitre and hyperthyreosis were not more common among patients with LS. Thyroid diseases have been shown to be common among female patients with LS, ranging in prevalence from 6.3% to 29.9% (11, 3, 6–8, Table SI).
Miscellaneous. Chronic rhinitis, nasopharyngitis, and pharyngitis were more common among patients with LS (1.5%, RR 3.5). These may all be forms of allergic rhinitis and related to the increased risk of atopic eczema.
Among ocular and neurological diseases, only tension-type headache and visual disturbances were more common among patients with LS (RR 2.4 and 2.1, respectively). There were no otological or psychiatric diseases with increased risk among patients with LS.
The current study also examined whether LS might be a protective factor against some diseases, but no correlation was found.
These results further advance the idea that the pathophysiology of LS includes several alterations in the regulation of both inflammatory and autoimmune processes and in the regulation of extracellular matrix formation and degradation. The exact mechanisms are the subject of further studies.
REFERENCES
- Singh N, Ghatage P. Etiology, Clinical features, and diagnosis of vulvar lichen sclerosus: a scoping review. Obstet Gynecol Int 2020; 2020: 7480754.
- Leibovitz A, Kaplun VV, Saposhnicov N, Habot B. Vulvovaginal examinations in elderly nursing home women residents. Arch Gerontol Geriatr 2000; 31: 1–4.
- Simpkin S, Oakley A. Clinical review of 202 patients with vulval lichen sclerosus: a possible association with psoriasis. Australas J Dermatol 2007; 48: 28–31.
- Virgili A, Borghi A, Cazzaniga S, Di Landro A, Naldi L, Minghetti S, et al. New insights into potential risk factors and associations in genital lichen sclerosus: data from a multicentre Italian study on 729 consecutive cases. J Eur Acad Dermatol Venereol 2017; 31: 699–704.
- Becker K, Meissner V, Farwick W, Bauer R, Gaiser MR. Lichen sclerosus and atopy in boys: coincidence or correlation? Br J Dermatol 2013; 168: 362–326.
- Higgins CA, Cruickshank ME. A population-based case-control study of aetiological factors associated with vulval lichen sclerosus. J Obstet Gynaecol 2012; 32: 271–275.
- Kreuter A, Kryvosheyeva Y, Terras S, Moritz R, Möllenhoff K, Altmeyer P, et al. Association of autoimmune diseases with lichen sclerosus in 532 male and female patients. Acta Derm Venereol 2013; 93: 238–241.
- Bieber AK, Steuer AB, Melnick LE, Wong PW, Pomeranz MK. Autoimmune and dermatologic conditions associated with lichen sclerosus. J Am Acad Dermatol 2021; 85: 228–229.
- Farrell AM, Marren P, Dean D, Wojnarowska F. Lichen sclerosus: evidence that immunological changes occur at all levels of the skin. Br J Dermatol 1999; 140: 1087–1092.
- Goussot R, Francès C, Cury K, Bessis D, Martin T, Chatelus E, et al. Prospective evaluation of the frequency of genital lichen sclerosus in 79 patients with systemic sclerosis. Br J Dermatol 2018; 179: 999–1000.
- Meyrick Thomas RH, Ridley CM, McGibbon DH, Black MM. Lichen sclerosus et atrophicus and autoimmunity – a study of 350 women. Br J Dermatol 1988; 118: 41–46. Erratum in Br J Dermatol 1988; 118: 736.
- Sideri M, Parazzini F, Rognoni MT, La Vecchia C, Negri E, Garsia S, et al. Risk factors for vulvar lichen sclerosus. Am J Obstet Gynecol 1989; 161: 38–42.
- Natsheh A, Shimony D, Bogot N, Nesher G, Breuer GS. Complete heart block in lupus. Lupus 2019; 28: 1589–1593.