ORIGINAL REPORT
Awareness, Patient Behaviour, and Treatment Expectations in a French Cohort with Actinic Keratosis (REAKT Survey)
Jean-Michel AMICI1, Pierre LÉVY2, Gregory CAILLET3, Chantal TOUBOUL4, Jean-Michel JOUBERT5 and Brigitte DRÉNO6
1Department of Dermatology, CHU Bordeaux University Hospital, Saint-André Hospital, Bordeaux, 2Paris-Dauphine University, PSL University, LEDA [LEGOS], Paris, 3Medical Affairs, Almirall SAS, Paris, 4Cerner Enviza France, Paris, 5Governmental Affairs, Almirall SAS, Paris, and 6Nantes University, INSERM, CNRS, Immunology and New Concepts in Immunotherapy, INCIT, UMR 1302/EMR6001, Nantes, France
This study was undertaken to evaluate disease awareness, attitudes, and expectations in people with actinic keratosis (AK) in France. A total of 639 participants aged ≥ 40 years reporting AK lesions diagnosed by a physician were recruited from a representative general population panel. Data were collected on disease awareness, care experience, sun protection behaviour,, and treatment expectations. The proportion of participants endorsing correct statements about AK rarely exceeded 50%. Only 332 participants (52.0%) reported that they knew much about treatments and 134 (21.0%) never felt the need to request information; 545 participants (85.3%) reported that waiting times to see dermatologists were excessive; 160 treated participants (40.8%) reported lesion persistence after treatment; and 140 (35.3%) that certain treatments made their skin painful or unsightly. Sun protection was sub-optimal, with 145 participants (22.7%) rarely or never going out in the sun with protection and 334 (52.3%) rarely or never putting on sunscreen in the morning. The most frequently desired improvements to care were “Treatments that make lesions disappear” (n = 528; 82.6%), “Treatments that are easy to use” (n = 524; 82.0%) and “Physicians to propose regular skin examinations” (n = 510; 79.8%). In conclusion, better information and education for AK patients are needed, as well as more acceptable topical treatments.
SIGNIFICANCE
Actinic keratosis is a common form of skin lesion, particularly in older individuals, caused by cumulative exposure to ultraviolet light. Actinic keratosis lesions may progress into squamous cell carcinoma. Since awareness of actinic keratosis in the general population is low, we conducted a questionnaire survey of disease perceptions. People diagnosed with actinic keratosis do not consider themselves particularly knowledgeable about their disease, its associated risks, or its treatment, and do not systematically engage in adequate sun protection behaviour. Better information and education for patients, as well as early use of an appropriate topical treatment, would help limit progression of lesions to squamous cell carcinoma.
Key words: actinic keratosis; sun protection; patient experience; treatment; patient perceptions.
Citation: Acta Derm Venereol 2025; 105: adv43351. DOI: https://doi.org/10.2340/actadv.v105.43351.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 12, 2025. Accepted after revision: Jun 5, 2025. Published: Jul 19, 2025.
Corr: Pr Jean-Michel Amici, Department of Dermatology, CHU Bordeaux University Hospital, Saint-André Hospital, CHU de Bordeaux, 1 Rue Jean Burguet, FR-33075 Bordeaux, France. E-mail: jmamici@gmail.com
Competing interests and funding: JMA has received consulting fees from Almirall SAS; PL has received honoraria for study development from Almirall SAS; BD has received consulting fees from Almirall SAS; GC is an employee of Almirall SAS, the sponsor of the study; CT is an employee of Cerner Enviza, which carried out the study sponsored by Almirall SAS; J-MJ is an employee of Almirall SAS, the sponsor of the study.
This study was funded by Almirall SAS.
INTRODUCTION
Actinic keratosis is a chronic skin disease characterized by rough, scaly keratotic lesions, typically on the face, scalp, or back of the hands, that develops with ageing (1). These lesions are caused by sun exposure and are considered to be precursors of squamous cell carcinoma (SCC) (1). In epidemiological surveys where cases are identified by systematic full-skin evaluation by a dermatologist, such as in the Rotterdam study (2), AK lesions may be identified in > 25% of individuals aged > 60 years. It has been estimated that up to 20% of AK lesions evolve to SCC (3,4). Apart from cumulative sun exposure, the principal risk factors for development of AK include skin phototype I or II, older age, male gender, and transplant patients (2,5).
Although AK is an important medical issue, awareness of AK in the general population, and the importance of treating it to prevent progression to SCC, is limited. Two surveys performed in the early 2000s in Europe, North America, and Australia reported that only 6% (6) or 7% (7) of general population samples were aware that AK exists, although around half the sample in both surveys were concerned about skin cancers and were aware that sun exposure was the principal risk factor for skin cancer, although most did not consider there to be a risk associated with “moderate” tanning. In these studies, around a third of participants declared that they rarely or never used sunscreen while outside, although marked between-country differences were observed (6).
We have recently performed a large retrospective survey of individuals with diagnosed AK in France, the REAKT study (8). This reported a prevalence of self-reported AK in individuals aged ≥ 40 in France of 4%, with a significant proportion (27.7%) of affected subjects aged < 65 years. Although participants had been diagnosed with AK by a physician, one-third never received treatment. The REAKT study also collected information on participants’ perceptions of AK, and their experience of care. This was broken down into 4 themes: (i) what do participants know about AK?; (ii) what is their experience of care?; (iii) what sun protection measures do they take?; and (iv) what are their expectations for treatment?
MATERIALS AND METHODS
The REAKT study is an observational, cross-sectional survey conducted in a representative sample of the French general population aged ≥ 40 years participating in a panel of households (METASKOPE). Data were collected using a postal questionnaire, which was sent to participants and returned in a prepaid envelope. The survey was implemented by Cerner Enviza (Paris, France) between 14 November and 19 December 2022. A Scientific Committee oversaw the design and implementation of the study, and the interpretation of the data. The characteristics of the study population, their lesions,, and their treatment have been described in a previous publication (8), to which the reader is referred for further details of the study design and methodology.
Study questionnaire
This questionnaire contained 25 questions, some of which had several sub-questions. The questionnaire was devised by the Scientific Committee specifically for use in this study. The time to complete the questionnaire was around 15 min. The questionnaire opened with 2 screening questions. The first was “Have you ever had, or do you have at the moment, one or more actinic keratosis lesions? These are scabby skin lesions or lesions that are rough to the touch, also called sun keratosis.” Individuals who did not report such lesions stopped the questionnaire at this point. The second question was “Have your lesions been diagnosed as actinic keratosis by a physician?”. Those individuals who replied that this was the case were eligible for the study. The study questionnaire next collected information on demographics, characteristics of AK lesions, diagnosis, and treatments (8).
Specific questions asked participants about their knowledge and beliefs regarding AK (8 items), their experience with AK care (8 items), sun exposure behaviour (7 items), and ways to improve AK care (10 items). The questions on sun exposure invited participants to rate their behaviours on a 4-point Likert scale (always, sometimes, rarely, never). The other questions invited them to agree with different statements on 10-point numerical scales, which were divided into 3 arbitrary classes (disagree: 0–4; more-or-less agree: 5–7; fully agree: 8–10) for analysis.
Statistical analysis
The different response modalities are presented as frequency counts and percentages. The data were also analysed by subgroups defined by age group (40–64 years vs ≥ 65 years), gender, treatment (not treated, any treatment, and topical treatment), and by phototype (I and II vs III or higher). The distribution of variables of interest was compared between subgroups with the χ² test.
Data were controlled, validated, and analysed centrally using Dasie software (and Soft) version 2.4.84 (adn-soft, Paris, France; https://adn-soft.com/logiciels/).
RESULTS
Study population
A total of 19,426 individual questionnaires were sent and 15,246 returned, corresponding to a response rate of 78.5%. Of these responders, 936 (6.1%) declared having current or previous AK lesions and 639 (4.2%), who made up the study population, declared that these lesions had been diagnosed by a physician. The mean age of participants was 69.6±10.6 years and 296 (46.3%) were men; 432 participants reported current lesions (67.6%). A flow diagram illustrating the selection of participants and the different subgroups of interest is presented in Fig. 1.
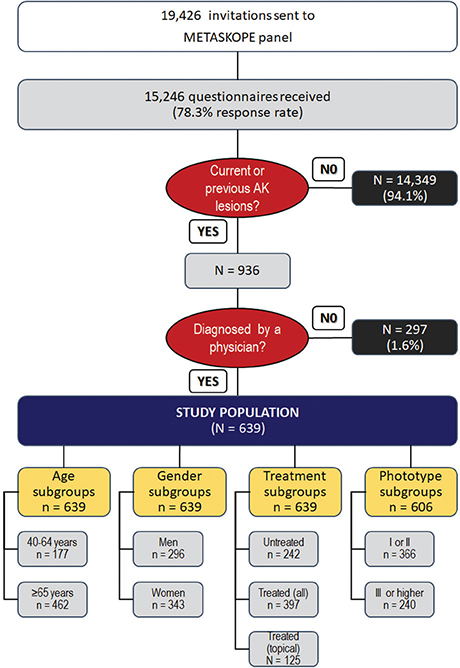
Fig. 1. Selection of participants and subgroups of interest. Twenty-four participants provided no information on phototypes. AK: actinic keratosis.
For the different themes of patient perceptions and expectations explored, the results are presented for all items for the full study population only. For the analysis of subgroups, items are presented in the results section only if there are significant differences between subgroups. Full information on responses for all items in all subgroups is available in Table SI.
Knowledge and beliefs about actinic keratosis
The level of agreement with the different statements is presented in Fig. 2. The items that received the highest percentage of “fully agree” responses were “If you have AK, you need sun protection every day” (80.0%), “AK lesions are caused by lifetime UV exposure” (58.4%), and “I feel that I do not know much about AK treatments” (52.0%). The items that received the lowest level of full agreement were “Treatments for AK are complicated to use” (19.3%), “AK is a skin condition that can be cured” (23.5%), and “Effective treatments for AK exist” (37.1%).
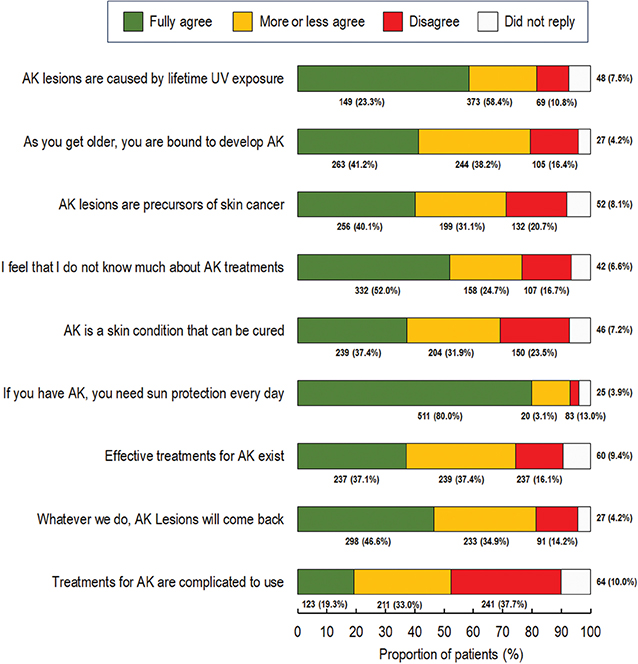
Fig. 2. Knowledge and beliefs regarding actinic keratosis. Analysis was performed for the 639 members of the study population. As questions were not obligatory, participants could skip questions and for this reason there are missing data for each item. The number of respondents (n, %) is provided below each bar.
Full information on item scores by subgroup is provided in Table SI. No significant differences were observed between men and women, except for the “I feel that I do not know much about AK treatments” item, with which women more fully agreed than men (55.4% vs 48.0%; p = 0.0175). Participants aged > 65 years were more frequently in full agreement than younger participants with the statements “AK lesions are caused by lifetime UV exposure” (61.9% vs 49.2%; p = 0.0003), “AK lesions are precursors of skin cancer” (43.5% vs 31.1%; p = 0.0011), and “If you have AK, you need sun protection every day” (81.8% vs 75.1%; p = 0.0495). Compared with never-treated participants, those who had received a topical treatment tended to be better informed, although they had a more negative opinion regarding treatments (Table I). No differences were observed for knowledge and beliefs items between the 2 phototype subgroups.
| Item | Untreated (n = 242) | All treatments (n = 397) | Topical treatments (n = 125) |
| As you get older, you are bound to develop AK | p = 0.2837 | p = 0.0074 | |
| Fully agree | 106 (43.8%) | 157 (39.6%) | 38 (30.4%) |
| More or less agree | 92 (38.0%) | 152 (38.3%) | 51 (40.8%) |
| Disagree | 33 (13.6%) | 72 (18.1%) | 31 (24.8%) |
| Missing | 11 (4.6%) | 16 (4.0%) | 5 (4.0%) |
| AK lesions are precursors of skin cancer | p = 0.0646 | p = 0.0149 | |
| Fully agree | 82 (33.9%) | 174 (43.8%) | 59 (47.2%) |
| More or less agree | 79 (32.6%) | 120 (30.2%) | 42 (33.6%) |
| Disagree | 57 (23.6%) | 75 (18.9%) | 16 (12.8%) |
| Missing | 24 (9.9%) | 28 (7.1%) | 8 (6.4%) |
| If you have AK, you need sun protection every day | p = 0.2405 | p = 0.0287 | |
| Fully agree | 185 (76.5%) | 326 (82.1%) | 111 (88.8%) |
| More or less agree | 38 (15.7%) | 45 (11.3%) | 8 (6.4%) |
| Disagree | 7 (2.9%) | 13 (3.3%) | 4 (3.2%) |
| Missing | 12 (5.0%) | 13 (3.3%) | 2 (1.6%) |
| Whatever we do, AK lesions will come back | p = 0.0223 | p = 0.0207 | |
| Fully agree | 95 (39.3%) | 203 (51.1%) | 69 (55.2%) |
| More or less agree | 95 (39.3%) | 128 (32.2%) | 38 (30.4%) |
| Disagree | 39 (16.1%) | 52 (13.1%) | 14 (11.2%) |
| Missing | 13 (5.4%) | 14 (3.5%) | 4 (3.2%) |
| Treatments for AK are complicated to use | p = 0.0033 | p = 0.0004 | |
| Fully agree | 31 (12.8%) | 92 (23.2%) | 41 (32.8%) |
| More or less agree | 91 (37.6%) | 120 (30.2%) | 47 (37.6%) |
| Disagree | 81 (33.5%) | 160 (40.3%) | 33 (26.4%) |
| Missing | 39 (16.1%) | 25 (6.3%) | 4 (3.2%) |
| Only items where significant differences were observed between treatment groups are shown (as indicated in bold). Full information is provided in Table SI. | |||
Experience of care
The majority of the study population (n = 505; 79.1%) fully agreed that they wanted explanations or advice about their AK lesions while 444 (69.5%) reported receiving all the information that they wanted. The only difference observed between subgroups was that treated participants more frequently reported needing advice (n = 335; 84.4%) than did untreated participants (n = 170; 70.2%). The information or advice received related to the importance of sun protection for 390/444 participants (87.8%), the cause of AK for 325 (73.2%), potential health consequences of AK for 150 (33.8%), for 106 (23.9%) the importance of taking medication as prescribed, and treatment side effects for 53 (11.9%). No differences between subgroups were observed for any of these items.
In the full study population, 545 (85.3%) fully agreed that the waiting time to see a dermatologist was too long, whereas 88 (13.8%) felt that several consultations were necessary before a diagnosis of AK was made. Differences between subgroups for these items were modest and generally not statistically significant (see Table SI). For the 397 treated participants, 68 (17.1%) fully agreed that they had to consult several physicians before finding a treatment that worked, 160 (40.8%) that their AK lesions did not go away after treatment, and 140 (35.3%) that certain treatments made their skin painful or unsightly. The proportion of participants fully agreeing with these statements was somewhat higher in the 125 participants who had received a topical treatment than it was for all treated participants combined (Table SI).
Behaviours to limit sun exposure
Avoiding being outdoors in the sun between 10.00 h and 16.00 h was one of the sun protection measures that a greater proportion of participants said they always followed (42.9%), together with putting on protective clothing or sunscreen before going out in the sun (40.5%) (Fig. 3). However, only 17.7% put on sunscreen each morning and 25.5% never did. Some 10% or less always avoided outdoor activities (holidays, having lunch, or participating in sports) and > 33% never avoided such activities (Fig. 3).
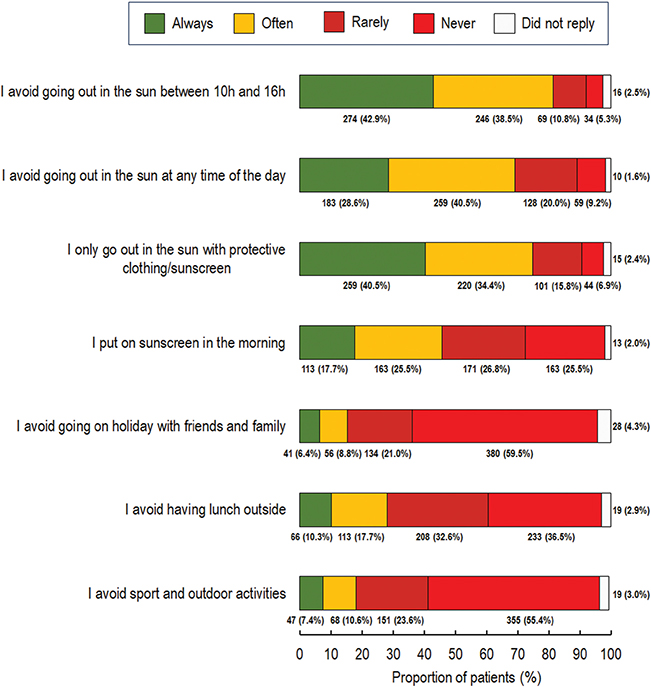
Fig. 3. Behaviours to limit sun exposure. Analysis was performed for the 639 members of the study population. As questions were not obligatory, participants could skip questions and for this reason there are missing data for each item. The number of respondents (n, %) are provided below each bar.
Differences in sun exposure limitation behaviours between subgroups are presented in Table II. With respect to age, participants aged > 65 years less frequently engaged in outdoor activities (going on holiday with friends or family, having lunch outside, sport, and outdoor activities). Women avoided going out in the sun between 10.00 h and 16.00 h and having lunch outside more frequently than men and more frequently put on sunscreen in the morning. Participants who had received a topical treatment for AK more frequently took sun exposure limitation measures than never treated participants across a range of items. The only difference in sun exposure limitation observed between phototypes was that participants with fairer phototypes (I and II) more frequently avoided going out in the sun at any time of day.
| Differences with respect to age | Total (n = 639) | Age 40–65 years (n = 177) | Age > 65 years (n = 462) |
| I avoid going on holiday with friends or family | p = 0.0127 | ||
| Always | 41 (6.4%) | 12 (6.8%) | 29 (6.3%) |
| Often | 56 (8.8%) | 11 (6.2%) | 45 (9.7%) |
| Rarely | 134 (21.0%) | 26 (14.7%) | 108 (23.4%) |
| Never | 380 (59.5%) | 124 (70.1%) | 256 (55.4%) |
| Missing | 28 (4.3%) | 4 (2.3%) | 24 (5.2%) |
| I avoid having lunch outside | p < 0.001 | ||
| Always | 66 (10.3%) | 15 (8.5%) | 51 (11.0%) |
| Often | 113 (17.7%) | 22 (12.4%) | 91 (19.7%) |
| Rarely | 208 (32.6%) | 49 (27.7%) | 159 (34.4%) |
| Never | 233 (36.5%) | 88 (49.7%) | 145 (31.4%) |
| Missing | 19 (2.9%) | 3 (1.7%) | 16 (3.5%) |
| I avoid sport and outdoor activities | p = 0.0181 | ||
| Always | 47 (7.4%) | 9 (5.1%) | 38 (8.2%) |
| Often | 68 (10.6%) | 18 (10.2%) | 50 (10.8%) |
| Rarely | 151 (23.6%) | 31 (17.5%) | 120 (26.0%) |
| Never | 354 (55.4%) | 116 (65.5%) | 238 (51.5%) |
| Missing | 19 (3.0%) | 3 (1.7%) | 16 (3.5%) |
| Differences with respect to gender | Total (n = 639) | Men (n = 296) | Women (n = 343) |
| I avoid going out in the sun between 10.00 and 16.00 h | p = 0.0065 | ||
| Always | 274 (42.9%) | 114 (38.5%) | 160 (46.7%) |
| Often | 246 (38.5%) | 111 (37.5%) | 135 (39.4%) |
| Rarely | 69 (10.8%) | 44 (14.9%) | 25 (7.3%) |
| Never | 34 (5.3%) | 19 (6.4%) | 15 (4.4%) |
| Missing | 16 (2.5%) | 8 (2.7%) | 8 (2.2%) |
| I put on sunscreen every morning | p < 0.0001 | ||
| Always | 113 (17.7%) | 38 (12.8%) | 75 (21.9%) |
| Often | 179 (28.0%) | 70 (23.7%) | 109 (31.8%) |
| Rarely | 171 (26.8%) | 79 (26.7%) | 92 (26.8%) |
| Never | 163 (25.5%) | 103 (34.8%) | 60 (17.5%) |
| Missing | 13 (2.0%) | 6 (2.0%) | 7 (2.0%) |
| I avoid having lunch outside | p = 0.0492 | ||
| Always | 66 (10.3%) | 34 (11.5%) | 32 (9.3%) |
| Often | 113 (17.7%) | 63 (21.3%) | 50 (14.6%) |
| Rarely | 208 (32.6%) | 84 (28.4%) | 124 (36.2%) |
| Never | 233 (36.5%) | 105 (35.5%) | 128 (37.3%) |
| Missing | 19 (2.9%) | 10 (3.4%) | 9 (2.6%) |
| Only items where significant differences were observed between treatment groups are shown (as indicated in bold). Full information is provided in Table SI. | |||
Ways to improve care
Of 10 proposed ways to improve management of AK, those to which participants most adhered (highest proportion of “fully agree”) were “Treatments that make lesions disappear” (82.6%), “Treatments that are easy to use” (82.0%), and “Physicians to propose regular skin examinations” (78.9%) (Fig. 4). However, for all the proposals, > 50% of participants fully agreed that they would improve care of AK.
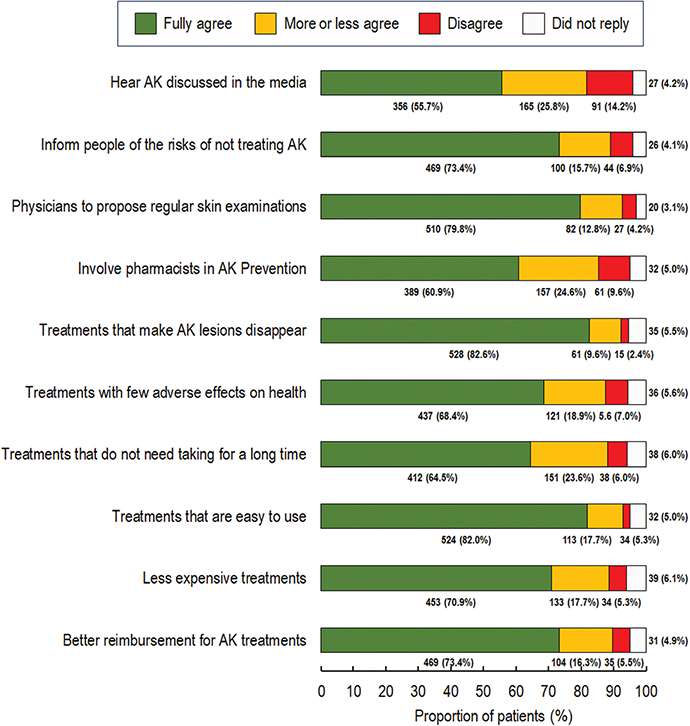
Fig. 4. Ways to improve care. Analysis was performed for the 639 members of the study population. As questions were not obligatory, participants could skip questions and for this reason there are missing data for each item. The number of respondents (n, %) is provided below each bar.
Differences in responses to these questions between age, gender, and phototype subgroups were, although occasionally statistically significant, modest (see Table SI). Differences between untreated participants and those who had received topical treatments were more substantial, with 91.2% of the latter group fully agreeing on the need for treatments that were easy to use compared with 77.3% of untreated participants. Similarly, 82.4% of participants with topical treatments fully agreed that there was a need for AK treatments that were better reimbursed, compared with 66.5% of untreated participants.
DISCUSSION
This study of perceptions of AK and AK care by people with diagnosed AK (REAKT) showed that the majority of participants had received information on their disease. However, the proportion of participants who were in full agreement with correct statements about the disease rarely exceeded 50% and up to 25% had erroneous beliefs about their disease (for example, 20.7% disagreed that AK lesions could be precursors of skin cancer). In addition, only 52.0% fully agreed that they knew much about treatments and 21% of participants never felt the need to ask for information. Participants who had previously been treated were generally better informed than untreated participants, and those aged > 65 years better informed than younger participants. Although study participants all reported having been diagnosed with AK by a physician, there is clearly a knowledge gap in this general population sample regarding AK and its management. This gap may not be widely appreciated by physicians, and ensuring adequate information and education of patients with AK should be a priority for them.
Interestingly, 79.8% of participants fully agreed that physicians should propose regular skin examinations. In a general population survey performed over 20 years ago, < 10% of French participants had had a routine skin check proposed (6), and this proportion is unlikely to have changed radically since then. This would be a relatively straightforward policy to implement, assuming that the resources are available in terms of dermatologists’ time. An increased role for general practitioners could also facilitate timely diagnosis of AK. Although general practitioners would not be expected to perform full skin evaluations, they could routinely check hands, face, and scalp, which are the most common sites of AK lesions, and systematically refer all patients with suspect lesions to a dermatologist. Over 85% of participants, notably those in the older age group, considered that they had to wait a long time for a dermatologist appointment. We have previously reported that the dermatologist was responsible for AK diagnosis and treatment for > 80% of REAKT participants (8), suggesting that the dermatologist is the “gatekeeper” for AK care. However, as the number of community dermatologists has been declining over the last 20 years (9), access to dermatologists is likely to remain a problem and the transfer of some care provision for AK to the general practitioner, including diagnosis and prescription of topical treatments, could help resolve this issue.
Sun protection behaviour was sub-optimal, with 22.7% of participants rarely or never going out in the sun with sunscreen or protective clothing and 52.3% rarely or never putting on sunscreen in the morning. However, 39.0% of participants had either never sought or never received advice on the importance of sun protection from a healthcare professional, and this is one area of care that could easily be improved at little or no cost to the health system. Of interest, we found that participants who had received treatment for AK more frequently took measures to avoid sun exposure than did untreated participants, suggesting that physicians who prescribe treatments also make the effort to communicate effectively on the need for sun protection. Our findings can be compared with similar data collected 20 years ago in an earlier general population survey, in which 52% of French participants wore hats when going out in the sun, 11% spent less time in the sun, but 38% rarely or never used sunscreen (6). A more recent large international survey (10) reported that, in Europe, 48% of participants exposed themselves to the sun between 10.00 h and 16.00 h and that only 24.1% applied sunscreen every 2 h when out in the sun. Although the questions are not asked in the same way between studies, participants with AK in our study appear to be somewhat more adherent to sun protection measures than the general population, which is to be desired. As in the 2024 general population survey (10), we found that women were more adherent than men.
Another area where participants considered that care of AK could be improved was treatments, with > 80% fully agreeing that there was a need for treatments that make AK lesions disappear and for treatments that are easy to use. Of interest, participants who had already received a topical treatment had a more negative opinion of current treatments than untreated participants, and more frequently agreed with the interest in developing treatments that were easy to use. With regard to their own treatment experience, a majority of treated participants fully or partially agreed that their own lesions did not resolve after treatment, and that certain treatments made their skin painful or unsightly, and were complicated to use. Taken together, these findings suggest that current topical treatments are not entirely satisfactory from the patient’s point of view and that there is an unmet need for more effective and acceptable treatments. Moreover, reinforcement of post-treatment care could alleviate local skin reactions associated with AK treatments. The cost of treatment was also recognized as an issue, with > 70% fully agreeing that less expensive treatments and better reimbursement were needed. Reimbursement rates for licensed topical treatments of AK in France are variable, ranging from zero to 65%, which may generate significant out-of-pocket expenses for patients; this heterogeneity is difficult to understand given that such treatments may play an important role in reducing the risk of SCC.
Strengths and limitations
This study has several strengths and limitations. The strengths include the general population setting, the large number of individuals sampled and the high response rate (> 75%). In addition, the questionnaire comprehensively covered multiple themes related to AK and its importance to the participant. The principal limitation is the absence of clinical ascertainment of the presence (or absence) of AK lesions. Similarly, as all the information was self-reported, its veracity cannot be guaranteed. For example, participants may have declared taking more sun protection measures than was actually the case. Although the response rate was high, it cannot be excluded that participants were more engaged with their skin disease than those who declined to participate, which may have introduced some bias into the findings.
Conclusion
This study identified, from the patient point of view, several areas where the management of AK could be improved. People diagnosed with AK do not consider themselves particularly knowledgeable about their disease, its associated risks, or its treatment, and do not systematically engage in adequate sun protection behaviour. The risk of progression of AK to SCC must be clearly explained to patients to motivate them to adhere to the therapeutic strategy. This could be achieved by improving access to dermatologists and giving general practitioners a more important role in the management of AK. Regular full skin examinations as part of routine management of AK would be welcomed by patients. As AK is caused by the total cumulative dose of UV radiation received, it is vital to promote public information on the dangers of excessive photo-exposure and the need for photoprotection. Finally, participants perceived the need for effective, well-tolerated treatments that are easy to use. Better information and education for patients, with the availability of more suitable topical treatments used early on, would help reduce the incidence of AK and limit progression to squamous cell carcinoma.
ACKNOWLEDGEMENTS
IRB approval status: The survey was conducted in accordance with the ESOMAR International Code on Market and Social Practice, the EphMRA Code of Conduct, relevant current French and European legislation, and Good Epidemiological Practice guidelines. Analyses performed using the METASKOPE panel have been approved by the Commission Nationale de l’Informatique et des Libertés (CNIL), the French national data protection authority. Ethical committee approval is not required for this form of survey in France.
REFERENCES
- de Oliveira ECV, da Motta VRV, Pantoja PC, Ilha CSO, Magalhães RF, Galadari H, et al. Actinic keratosis: review for clinical practice. Int J Dermatol 2019; 58: 400–407. https://doi.org/10.1111/ijd.14147
- Flohil SC, van der Leest RJ, Dowlatshahi EA, Hofman A, de Vries E, Nijsten T. Prevalence of actinic keratosis and its risk factors in the general population: the Rotterdam Study. J Invest Dermatol 2013; 133: 1971–1978. https://doi.org/10.1038/jid.2013.134
- Eisen DB, Asgari MM, Bennett DD, Connolly SM, Dellavalle RP, Freeman EE, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol 2021; 85: e209–e233. https://doi.org/10.1016/j.jaad.2021.02.082
- Balcere A, Konrāde-Jilmaza L, Pauliņa LA, Čēma I, Krūmiņa A. Clinical characteristics of actinic keratosis associated with the risk of progression to invasive squamous cell carcinoma: a systematic review. J Clin Med 2022; 11: 5899. https://doi.org/10.3390/jcm11195899
- Rosen T, Lebwohl MG. Prevalence and awareness of actinic keratosis: barriers and opportunities. J Am Acad Dermatol 2013; 68: S2–9. https://doi.org/10.1016/j.jaad.2012.09.052
- MacKie RM. Awareness, knowledge and attitudes to basal cell carcinoma and actinic keratoses among the general public within Europe. J Eur Acad Dermatol Venereol 2004; 18: 552–555. https://doi.org/10.1111/j.1468-3083.2004.00993.x
- Halpern AC, Kopp LJ. Awareness, knowledge and attitudes to non-melanoma skin cancer and actinic keratosis among the general public. Int J Dermatol 2005; 44: 107–111. https://doi.org/10.1111/j.1365-4632.2005.02090.x
- Dréno B, Lévy P, Caillet G, Touboul C, Joubert JM, Amici JM. Epidemiology and management of actinic keratosis in France: a general population survey (REAKT). Acta Derm Venereol 2025: 105: adv42372. https://doi.org/10.2340/actadv.v105.42372
- Société Française de Dermatologie. Livre blanc: les défis de la dermatologie en France. Paris: SFD, 2018.
- Lim HW, Saint Aroman M, Skayem C, Halioua B, Perez Cullell N, Ben Hayoun Y, et al. Sun exposure and protection habits: self-reported attitudes, knowledge and behaviours. J Eur Acad Dermatol Venereol 2024; 38: 2024–2033. https://doi.org/10.1111/jdv.20080