ORIGINAL REPORT
Oesophageal Lichen Planus: Case Series and Review of the Literature
Nerea MANZANARES1, Andrea MOLINA-ALVAREZ2, Mar IGLESIAS2, Juan ENRIQUE NAVES3, Ramon M. PUJOL1 and Sonia SEGURA1
1Dermatology Department, Hospital del Mar–Hospital del Mar Research Institute, Universitat Pompeu Fabra (UPF), Barcelona, 2Pathology Department, Hospital del Mar–Hospital del Mar Research Institute, Universitat Pompeu Fabra (UPF), Barcelona, and 3Gastroenterology Department, Hospital del Mar–Hospital del Mar Research Institute, Universitat Pompeu Fabra (UPF), Barcelona, Spain
Lichen planus affects 0.5% to 2% of the population. The involvement of the oesophagus is a rare manifestation with high morbidity and risk of malignancy. Clinical characteristics and diagnostic-therapeutic strategies were reviewed. A retrospective study of clinical-pathological characteristics, endoscopic findings, and follow-up of patients with oesophageal lichen planus treated at a tertiary hospital during 2006–2023 was conducted. Nine patients (1 man, 8 women) with a median age of 76 years were included. All patients had oral lichen planus. Dysphagia was the initial symptom, being the first manifestation of the disease in 2 cases. All presented lesions in the oral oesophagus with fibrous rings, stenosis, and mucosal denudation. Histological changes of the lichenoid type were observed in 8/9. After a median follow-up of 2 years, no progression to oesophageal squamous cell carcinoma was observed. Swallowed glucocorticoid therapy, proton pump inhibitors, prokinetics, and oesophageal dilatations were prescribed. Eight out of 9 patients showed partial improvement with clinical stabilization. Oesophageal lichen planus is an infrequent and underdiagnosed disease. Its diagnosis may be based on endoscopic features, histopathology, and direct immunofluorescence. The correct management is often challenging, but necessary because this entity has been associated with oesophageal squamous cell carcinoma and poor quality of life.
SIGNIFICANCE
Oesophageal lichen planus is a rare and underdiagnosed form of lichen planus, predominantly affecting middle-aged women with oral lichen planus. Dysphagia is the primary symptom. Diagnosis is based on endoscopic features, histopathology, and immunofluorescence. First-line treatment involves swallowed glucocorticoid therapy. This disease has been associated with oesophageal squamous cell carcinoma. The correct management is essential to improve quality of life and prevent complications.
Key words: lichen planus; oesophagus; dysphagia; squamous cell carcinoma.
Citation: Acta Derm Venereol 2025; 105: adv43358. DOI: https://doi.org/10.2340/actadv.v105.43358.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 13, 2025. Accepted after revision: Jun 23, 2025. Published: Aug 11, 2025.
Corr: Sonia Segura, MD, PhD, Department of Dermatology, Hospital del Mar–Institut Mar d’Investigacions Mèdiques, Universitat Pompeu Fabra (UPF) and UVic (Universitat de Vic-Universitat Central de Catalunya), Passeig Marítim, 25-29, ES-08003 Barcelona, Spain. E-mail: ssegura@hmar.cat
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Lichen planus (LP) is a chronic T-cell-mediated inflammatory mucocutaneous disorder of uncertain aetiology that affects the skin, cutaneous appendages, and mucous membranes. It affects 0.5% to 2% of the population with a predilection for middle-aged adults. LP often affects primarily the skin and oral or genital mucosa. However, other mucous membranes can be involved including the oesophagus, conjunctivae, bladder, nose, larynx, stomach, and anus (1).
Although the involvement of the oesophagus was initially described in 1982, there are only a few case reports of oesophageal lichen planus (OLP) and our understanding of this condition remains severely limited (1). It is suggested that it is an underdiagnosed condition, being more frequent if there is involvement of the oral mucosa. The exact prevalence is unknown, but some studies have estimated that it could be present in 26% of patients with LP (2). OLP is often asymptomatic and may develop either as an isolated manifestation or concomitantly with LP in other locations. Even though dysphagia is the most common symptom, odynophagia, heartburn, weight loss, and retrosternal pain have also been reported (3). Endoscopic findings can range from subtle mucosal changes to erosive oesophagitis with strictures. Histopathological examination is crucial for diagnosis and typically reveals characteristic features of LP, including lymphocytic T-cell infiltrate and intraepithelial apoptosis (3, 4). The management of OLP remains challenging. Treatment options are often limited and may include proton pump inhibitors (PPIs) to control acid reflux, topical therapies such as corticosteroids or calcineurin inhibitors, and systemic medications like immunosuppressants or immunomodulators. In severe cases, endoscopic dilation may be necessary to relieve dysphagia (5–7).
This study presents a series of 9 cases of OLP, providing valuable insights into the clinical spectrum, diagnostic challenges, and therapeutic approaches. A greater understanding of OLP within the medical community is essential to facilitate early diagnosis and improve the clinical outcomes for individuals affected by this disorder.
PATIENTS AND METHODS
We performed an observational retrospective study with those patients diagnosed with OLP at the Hospital del Mar, Barcelona (Spain). All patients with confirmed mucocutaneous LP followed at the Department of Dermatology from January 2006 to December 2023 were recruited. The indication for endoscopy with biopsy was based on the following protocol:
- Oesophageal symptoms: all patients with oral LP underwent a thorough medical history-taking to detect symptoms such as dysphagia, odynophagia, heartburn, weight loss, or retrosternal pain. If any of these symptoms were present, an endoscopy and biopsies were performed to rule out or confirm OLP.
- Extensive oral involvement: endoscopy was performed on patients with erosive-type oral LP and extensive involvement, even in the absence of clear oesophageal symptoms, due to the higher risk of co-occurrence with OLP in these cases.
All patients with endoscopic and pathological findings compatible with OLP were included in the study. Following a systematized protocol, we collected a number of epidemiological, clinical, endoscopic, histopathological, therapeutic, and evolutive data. This study was performed according to the recommendations of the Declaration of Helsinki and was approved by the Research Ethics Committee.
RESULTS
A total of 9 patients with OLP were enrolled. They were 8 females and 1 male, with a median age of 76 years (range 56–89). Clinical manifestations, endoscopic findings, pathological results of oesophageal biopsy, and treatment of all patients are given in Table I. All patients presented moderate to severe oral erosive LP, confirmed by oral mucosa biopsy in 8 out of 9 patients. Other manifestations included cutaneous LP (2/9), LP pilaris (2/9), and genital LP (2/9). Dysphagia was the initial and consistent symptom in all patients and oesophageal symptoms were the primary manifestation of the disease in 2 cases. In all individuals, LP lesions involved the first third of the oesophagus and were manifested by fibrous rings (“trachealization”), stenosis, elevated lacy white papules, denudation, and erosions of mucosa surface (Fig. 1). Biopsies of the oral oesophagus were performed and 8 out of 9 cases presented lichenoid changes in at least 1 biopsy consisting in apoptotic keratinocytes, epithelial detachment, lymphocytic infiltrate in the superficial lamina propria and/or dyskeratosis (Figs 2 and 3), while 1 patient presented nonspecific changes. Direct immunofluorescence (DIF) microscopy was conducted in only 1 case, revealing an absence of characteristic linear fibrinogen deposition along the basement membrane. Concomitant Candida colonization in affected areas of the oesophagus was observed in 1 case.
| Demographics | Clinical manifestations | Endoscopic findings | Histopathology | DIF microscopy | Treatment | ||
| Case | Age | Sex | |||||
| 1 | 79 | M | Dysphagia, oral LP | Stenosis, ring structures, tearing and denudation of the mucosa | Nonspecific | NA | Fluticasone PDN 30mg/day PPI Prokinetics Dilation (2) |
| 2 | 63 | F | Dysphagia, oral LP | Stenosis, tearing of the mucosa | Lichenoid inflammatory infiltrate, detachment of squamous epithelium, intraepidermal apoptosis | NA | PPI Dilation (2) |
| 3 | 84 | F | Dysphagia, oral LP, genital LP | Ring structures, denudation of the mucosa | Lichenoid inflammatory infiltrate, intraepidermal apoptosis | NA | PPI Prokinetics NTG |
| 4 | 76 | F | Dysphagia, oral LP | Stenosis, ring structures, tearing of the mucosa | Nonspecific, concomitant Candida colonization | Negative | PPI Fluticasone |
| 5 | 77 | F | Dysphagia, oral LP, cutaneous LP | Ring structures, tearing and denudation of the mucosa | Lichenoid inflammatory infiltrate, detachment of squamous epithelium | NA | PPI |
| 6* | 75 | F | Dysphagia, oral LP, genital LP | Stenosis, ring structures | Lichenoid inflammatory infiltrate, detachment of squamous epithelium, intraepidermal apoptosis | NA | PPI Fluticasone Dilation (5) |
| 7 | 89 | F | Dysphagia, oral LP, LP pilaris |
Ring structures, denudation of the mucosa, whitish and rough surface | Lichenoid inflammatory infiltrate, intraepidermal apoptosis | NA | Fluticasone PPI Sucralfate Dilation (2) |
| 8 | 76 | F | Dysphagia, oral LP | Stenosis | Lichenoid inflammatory infiltrate, intraepidermal apoptosis | NA | Budesonide Dilation (2) |
| 9 | 56 | F | Dysphagia, oral LP, LP pilaris, cutaneous LP | Ring structures | Lichenoid inflammatory infiltrate, intraepidermal apoptosis | NA | PPI Fluticasone |
| LP: lichen planus; DIF: direct immunofluorescence; M: male; F: female; NA: not available; PDN: prednisone; PPI: proton pump inhibitors; NTG: nitroglycerin | |||||||
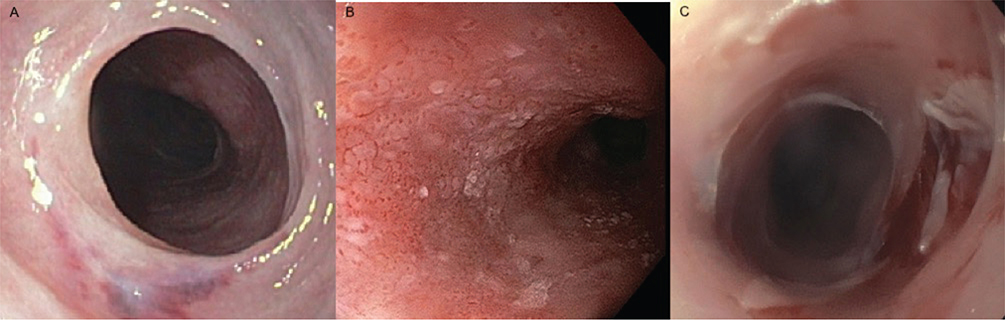
Fig. 1. Endoscopic findings in oesophageal lichen planus. (A) Fibrous rings. (B) Elevated lacy white papules. (C) Denudation and erosions of the mucosa.
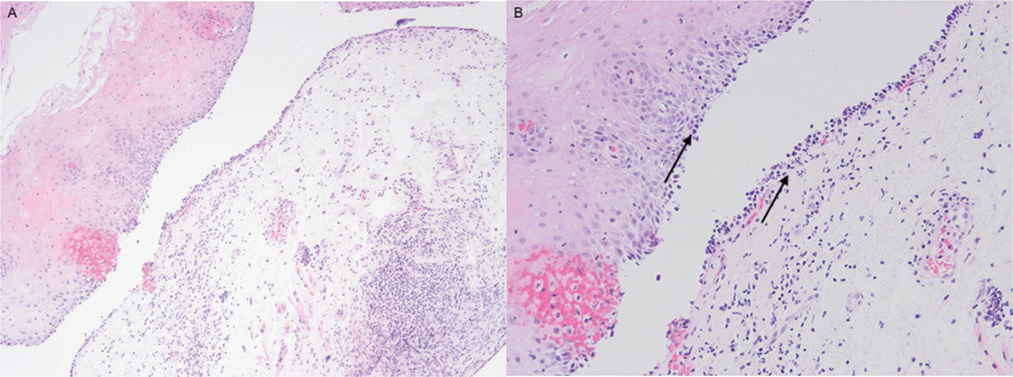
Fig. 2. Histological section ([A] H&E 100x; [B] H&E 200x) of oesophageal lichen planus reveals lichenoid lymphocytic infiltrate involving lamina propria and basal epithelium (black arrow).
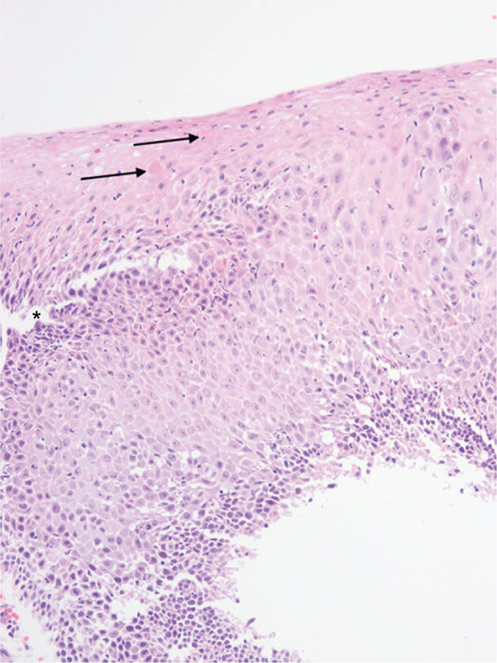
Fig. 3. Histological section (H&E 200x) of oesophageal lichen planus shows intraepidermal apoptosis (black arrow) and detachment of squamous epithelium (star).
The diagnosis was established after a median of 5 years (range 2 months–7 years) from the onset of symptoms. After a median follow-up period of 2 years (range 1–12), no cases of progression to oesophageal squamous cell carcinoma (ESCC) were observed. One patient died due to oral squamous cell carcinoma arising from oral LP 13 years after oral lichen planus diagnosis.
The treatment included swallowed glucocorticoid therapy (6/9), proton pump inhibitors (8/9), prokinetics (2/9), and oesophageal dilations (5/9, requiring 2 to 5 sessions per patient). Eight out of 9 patients showed partial improvement with clinical stabilization. This assessment of improvement was based on several key indicators: dysphagia monitoring via patient-reported symptomatic relief and qualitative changes in eating habits; endoscopic findings, where changes in mucosal lesions contributed to the definition of improvement; and the need for dilatations, as information on the frequency and success of oesophageal dilatations in patients who required them also served as a key indicator of treatment response. One remaining patient progressed despite the treatments, resulting in the decision to initiate a regimen of 30 mg/day prednisone.
DISCUSSION
OLP was first described by Al-Shihabi and Jackson in 1982 (1). Although initially considered a rare phenomenon, it is now accepted that it most likely represents an underrecognized entity, and the oesophagus is the gastrointestinal structure most commonly affected in LP. Dickens et al. (2) reported 19 patients with mucocutaneous LP and upper endoscopy revealed oesophageal lesions in 5 cases (26%), although only 1 of these patients had symptomatic dysphagia. In contrast, a larger study of 584 patients with oral LP from Cincinnati identified 8 cases who underwent endoscopy because of dysphagia; among these, only 4 showed both endoscopic and histological evidence indicative of OLP, suggesting a prevalence of less than 1% (3). The large discrepancy between these studies may result from high rate of asymptomatic or subtle disease, endoscopic and pathologic unfamiliarity with the condition, and the possibility that oesophageal involvement could be the sole manifestation of LP. This is evidenced by the considerable delay between the onset of oesophageal symptoms and the diagnosis of OLP (4, 5).
This condition has a predilection for middle-aged to older women (6) as observed in our series, with a clear predominance of females (female-to-male ratio 8:1) and a median age at diagnosis of 76 years.
Extra-oesophageal LP may be present in up to 99% of patients, and it is more commonly found in the oral cavity. Oesophageal symptoms may precede, occur in conjunction with, or develop after the diagnosis of mucocutaneous LP. In addition, there has been a single report of OLP in a patient without lesions in other sites (6, 7). Seven of our patients (78%) had extra-oesophageal LP (skin and oral mucosa) prior to presenting with OLP, whereas in 2 cases the oesophageal symptoms preceded the diagnosis of mucocutaneous LP.
Dysphagia is the most common symptom and is present in up to 40% of cases, most probably influenced by the severity of disease and related to a stricture formation in the first third of the oesophagus. Odynophagia, heartburn, weight loss, and retrosternal pain have also been reported (8–10). In our case series, dysphagia was the predominant symptom with a median duration of symptoms prior to diagnosis of 5 years.
Endoscopic findings are non-specific and can be subtle, but include stenosis and ring fibrosis (“trachealization”), elevated lacy white papules, pseudomembranes, desquamation, erosions, and friable mucosa. These changes may be observed in all parts of the oesophagus, but the first third is the most frequent location (2, 4). The endoscopic findings in our patients included fibrous rings, stenosis, elevated lacy white papules, denudation of mucosal surface, and erosions of the mucosa. These lesions were localized in the first third of the oesophagus. In the differential diagnosis of OLP, especially if there is oesophageal stricture, there may be different potential causes: peptic oesophagitis, eosinophilic oesophagitis, mucous membrane pemphigoid, infectious oesophagitis, and neoplasms. To ensure an accurate diagnosis it is crucial to perform biopsies of strictures and other areas of the oesophageal mucosa.
Diagnostic histological criteria for OLP have been extensively examined in the literature (8). Most studies describe a consistent set of histological features typically associated with OLP, including epithelial detachment (subepithelial/intraepithelial), lymphocytic T-cell infiltrate (subepithelial, junctional, intraepithelial), intraepithelial apoptosis (Civatte bodies), and dyskeratosis (11). However, these findings lack specificity and may resemble those observed in other oesophageal disorders, including gastroesophageal reflux and drug-induced lichenoid lesions, posing challenges for the diagnosis of OLP (3, 4). Eight of our patients presented lichenoid features in at least 1 biopsy. These changes included apoptotic keratinocytes, epithelial detachment, lymphocytic infiltrate in superficial lamina propria, and/or dyskeratosis. Only in 1 case was the biopsy nonspecific, demonstrating that, in cases of suspected disease, performing an endoscopy and biopsy of the oesophagus can lead to the correct diagnosis in most cases.
DIF microscopy serves as a valuable adjunctive tool, particularly in cases where the differential diagnosis involves entities such as other lichenoid lesions, mucous membrane pemphigoid, or pemphigus vulgaris. Positive DIF microscopy results, characterized by linear fibrinogen deposition along the basement membrane, support the diagnosis of OLP when consistent with corresponding macroscopic and microscopic findings (8). This technique is not always performed because it requires frozen tissue samples and special laboratory procedures that are not carried out if the diagnosis is not suspected during endoscopy examination. Unfortunately, in our case series DIF microscopy was conducted in only a single biopsy, revealing the absence of immune deposits along the basal membrane.
It is important to emphasize that the definitive diagnosis of OLP cannot rely solely on histology. Clinical suspicion plays a crucial role in achieving an accurate diagnosis, especially given that endoscopic findings can be subtle and easily overlooked. Furthermore, histological findings, while important, lack specificity and may lead to misdiagnosis in the absence of comprehensive evaluation of symptoms and clinical history. Integrating clinical, endoscopic, histological, and DIF microscopy findings enhances diagnostic accuracy, as indicated by the current literature (11).
Due to chronic inflammation, increased turnover of basal cells, and the use of immunosuppressive agents, malignant transformation may be a concern and has been documented in case reports. In 2003, Calabrese et al. reported the first case of malignant transformation of OLP to oesophageal squamous cell carcinoma (ESCC), almost 10 years after the initial diagnosis (12). Several additional cases have subsequently been reported and the risk of malignancy in symptomatic OLP has been estimated to range from 5.55% to 6.1% with a median time to progression of 3.5 years, and the highest risk is present ≈ 5 years after OLP diagnosis (13–15). The prognostic significance of this potential complication highlights the importance of early diagnosis and accurate therapy. Therefore, periodic annual surveillance endoscopy with mucosal biopsies has been proposed in patients with OLP (12–15). One of the patients in our series developed oral squamous carcinoma, but none of the patients developed oesophageal malignancy after a median follow up of 2 years.
To date, there are no therapy guidelines for OLP. Current therapeutic approaches are primarily based on case reports, small case series, and extrapolation from cutaneous or oral LP. The primary goals of therapy are to alleviate symptoms, improve dysphagia, prevent stricture formation, and induce remission. Both systemic or topical steroids and swallowed fluticasone propionate have been postulated as effective initial therapy. Patients with a mild form of the disease may be treated with topical or swallowed steroids, whereas in more severe cases systemic corticosteroids induce a rapid response and are considered the first line of treatment. However, clinical relapses are a frequent event (85%) when tapering. Furthermore, there is a possibility of a dose-dependent systemic contribution to the observed therapeutic effects, even if the primary intent is local action. Other therapies include topical tacrolimus, topical and systemic retinoids, oral cyclosporine, methotrexate, dapsone, azathioprine, rituximab, adalimumab, and IFN-α. In symptomatic oesophageal stenosis non-responsive to steroids, endoscopic dilation may be necessary (5, 11, 16–24). The limited long-term success with conventional therapies and the side effect profile of systemic corticosteroids highlight the need for alternative, targeted approaches. Small molecules represent a growing class of therapeutic agents that typically work by inhibiting specific intracellular enzymes or signalling pathways, offering more targeted immunosuppression compared with broader systemic agents. Oral tacrolimus suppresses T-cell activation and proliferation. Case reports and small series suggest its efficacy in inducing remission and preventing relapses in patients unresponsive to or dependent on systemic corticosteroids (26, 27). Tofacitinib is a small molecule inhibitor of JAK1 and JAK3. By blocking these pathways, tofacitinib can reduce the inflammatory cascade characteristic of OLP. Its success in refractory OLP has been reported in recent literature (28–30). Further research, including controlled trials, is needed to establish the long-term efficacy and safety of tofacitinib and other JAK inhibitors in OLP. It is important to note that dilation of the strictures can trigger the Koebner phenomenon, which involves the development of isomorphic pathological lesions in the traumatized uninvolved skin or mucosa (12). Endoscopic dilation was performed in 5 patients, with 2 to 5 sessions per patient, in our series. All patients reported improvement in dysphagia but developed recurrent symptoms, requiring repeated dilations.
In essence, OLP is a fairly common underdiagnosed disorder that should be suspected in middle-aged female patients with oral LP who present with dysphagia. Increased awareness regarding the diagnosis of OLP seems important in order to avoid unnecessary diagnostic delays and adopt specific therapeutic strategies that may permit an improvement in the quality of life of patients and probably prevent potential serious complications (malignant transformation).
These findings should be interpreted with caution due to the limitations of this study. First, DIF microscopy was not performed in all cases, which limits the definitive diagnostic certainty, particularly in differentiating our findings from other immune-mediated conditions. Consequently, alternative diagnoses such as lichen planus pemphigoid or mucous membrane pemphigoid–lichen planus overlap cannot be definitively excluded in some instances. Furthermore, future prospective studies with larger sample sizes and standardized diagnostic protocols, including routine DIF microscopy, are needed to confirm our results.
In conclusion, OLP is a fairly common underdiagnosed disorder. It should be suspected in middle-aged female patients with oral LP who present with dysphagia. Diagnosis can be based on endoscopic features and histopathology. The biopsy can be nonspecific, and it is important to recognize and suspect this entity in order to establish the diagnosis and avoid unnecessary diagnostic delays. Correct management is often challenging, but swallowed glucocorticoid therapy should be a prudent therapeutic option over other systemic and more toxic therapies. Additionally, in cases with symptomatic oesophageal stricture, endoscopic dilation may be necessary. Close follow-up is crucial because OLP is associated with a significantly increased risk of ESCC and poor quality of life. Unfortunately, as with other forms of lichen planus, there are currently no therapeutic guidelines or drugs that have shown evidence of their efficacy. Hopefully, with new biological drugs and targeted therapies such as JAK inhibitors, the desert-like scenario of this disease will change in the not too distant future.
REFERENCES
- Al-Shihabi BM, Jackson JM. Dysphagia due to pharyngeal and oesophageal lichen planus. J Laryngol Otol 1982; 96: 567–571. https://doi.org/10.1017/S0022215100092835
- Dickens CM, Heseltine D, Walton S, Bennett JR. The oesophagus in lichen planus: an endoscopic study. BMJ 1990; 300: 84. https://doi.org/10.1136/bmj.300.6717.84
- Eisen D. The evaluation of cutaneous, genital, scalp, nail, esophageal, and ocular involvement in patients with oral lichen planus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88: 431–436. https://doi.org/10.1016/S1079-2104(99)70057-0
- Shenfine J, Preston SR. Lichen planus in the oesophagus: are we missing something? Eur J Gastroenterol Hepatol 2006; 18: 1043–1045. https://doi.org/10.1097/01.meg.0000236870.01151.c2
- Chandan VS, Murray JA, Abraham SC. Esophageal lichen planus. Arch Pathol Lab Med 2008; 132: 1026–1029. https://doi.org/10.5858/2008-132-1026-ELP
- Oliveira JP, Uribe NC, Abulafia LA, Quintella LP. Esophageal lichen planus. An Bras Dermatol 2015; 90: 394–396. https://doi.org/10.1590/abd1806-4841.20153255
- Plentz RR, Müller CC, Laenger F, Manns MP, Meier PN. Lichenoide Ösophagitis ohne Haut-, Genital- oder Mundschleimhautbeteiligung [Lichen planus oesophagitis without skin, genital or oral mucosa involvement]. Z Gastroenterol 2004; 42: 379–382. https://doi.org/10.1055/s-2004-813116
- Decker A, Schauer F, Lazaro A, Monasterio C, Schmidt AR, Schmitt-Graeff A, et al. Esophageal lichen planus: current knowledge, challenges and future perspectives. World J Gastroenterol 2022; 28: 5893–5909. https://doi.org/10.3748/wjg.v28.i41.5893
- Rosic Despalatovic B, Bratanic A, Puljiz Z, Bozikovic J. Esophageal stenosis in a patient with lichen planus. Case Rep Gastroenterol 2019; 13: 134–139. https://doi.org/10.1159/000498907
- Franco DL, Islam SR, Lam-Himlin DM, Fleischer DE, Pasha SF. Presentation, diagnosis, and management of esophageal lichen planus: a series of six cases. Case Rep Gastroenterol 2015; 9: 253–260. https://doi.org/10.1159/000437292
- Schauer F, Monasterio C, Technau-Hafsi K, Kern JS, Lazaro A, Deibert P, et al. Esophageal lichen planus: towards diagnosis of an underdiagnosed disease. Scand J Gastroenterol 2019; 54: 1189–1198. https://doi.org/10.1080/00365521.2019.1674375
- Calabrese C, Fabbri A, Benni M, Areni A, Scialpi C, Miglioli M, et al. Squamous cell carcinoma arising in esophageal lichen planus. Gastrointest Endosc 2003; 57: 596–599. https://doi.org/10.1067/mge.2003.154
- Schwartz MP, Sigurdsson V, Vreuls W, Lubbert PH, Smout AJ. Two siblings with lichen planus and squamous cell carcinoma of the oesophagus. Eur J Gastroenterol Hepatol 2006; 18: 1111–1115. https://doi.org/10.1097/01.meg.0000221854.25039.83
- Ravi K, Codipilly DC, Sunjaya D, Fang H, Arora AS, Katzka DA. Esophageal lichen planus is associated with a significant increase in risk of squamous cell carcinoma. Clin Gastroenterol Hepatol 2019; 17: 1902–1903.e1. https://doi.org/10.1016/j.cgh.2018.10.018
- Abraham SC, Ravich WJ, Anhalt GJ, Yardley JH, Wu TT. Esophageal lichen planus: case report and review of the literature. Am J Surg Pathol 2000; 24: 1678–1682. https://doi.org/10.1097/00000478-200012000-00014
- Kern JS, Technau-Hafsi K, Schwacha H, Kuhlmann J, Hirsch G, Brass V, et al. Esophageal involvement is frequent in lichen planus: study in 32 patients with suggestion of clinicopathologic diagnostic criteria and therapeutic implications. Eur J Gastroenterol Hepatol 2016; 28: 1374–1382. https://doi.org/10.1097/MEG.0000000000000732
- Nielsen JA, Law RM, Fiman KH, Roberts CA. Esophageal lichen planus: a case report and review of the literature. World J Gastroenterol 2013; 19: 2278–2281. https://doi.org/10.3748/wjg.v19.i14.2278
- Ukleja A, DeVault KR, Stark ME, Achem SR. Lichen planus involving the esophagus. Dig Dis Sci 2001; 46: 2292–2297. https://doi.org/10.1023/A:1011943805711
- Keate RF, Williams JW, Connolly SM. Lichen planus esophagitis: report of three patients treated with oral tacrolimus or intraesophageal corticosteroid injections or both. Dis Esophagus 2003; 16: 47–53. https://doi.org/10.1046/j.1442-2050.2003.00289.x
- Zamani F, Haghighi M, Roshani M, Sohrabi M. Esophageal lichen planus stricture. Middle East J Dig Dis 2019; 11: 52–54. https://doi.org/10.15171/mejdd.2018.128
- Westbrook R, Riley S. Esophageal lichen planus: case report and literature review. Dysphagia 2008; 23: 331–334. https://doi.org/10.1007/s00455-007-9136-x
- Ynson ML, Forouhar F, Vaziri H. Case report and review of esophageal lichen planus treated with fluticasone. World J Gastroenterol 2013; 19: 1652–1656. https://doi.org/10.3748/wjg.v19.i10.1652
- Katzka DA, Smyrk TC, Bruce AJ, Romero Y, Alexander JA, Murray JA. Variations in presentations of esophageal involvement in lichen planus. Clin Gastroenterol Hepatol 2010; 8: 777–782. https://doi.org/10.1016/j.cgh.2010.04.024
- Koszoru K, et al. Low-dose oral glucocorticoid therapy in lichen planus: a retrospective cohort study. Indian J Dermatol Venereol Leprol 2023; 89: 568–571. https://doi.org/10.25259/IJDVL_1111_2021
- Bagger-Jörgensen H, Abdulrasak M, Sandeman K, Binsalman M, Sjöberg K. Oesophageal lichen planus successfully treated with budesonide orodispersible tablets: a case report. Case Rep Gastroenterol 2024; 18: 266–272. https://doi.org/10.1159/000538894
- Kukreja K, Kumar A, Camisa C, Jacobs J, Richter JE. Esophageal lichen planus: the efficacy and safety of tacrolimus in reducing inflammation and need for dilation. Clin Transl Gastroenterol 2024; 15: e00752. https://doi.org/10.14309/ctg.0000000000000752
- Keate RF, Williams JW, Connolly SM. Lichen planus esophagitis: report of three patients treated with oral tacrolimus or intraesophageal corticosteroid injections or both. Dis Esophagus 2003; 16: 47–53. https://doi.org/10.1046/j.1442-2050.2003.00289.x
- Mansouri P, Jafari MA, Chalangari R, Roohaninasab M, Goodarzi A. Successful treatment of erosive lichen planus with tofacitinib: a case series and review of the literature. Clin Med Insights Case Rep 2024; 17: 11795476241237350. https://doi.org/10.1177/11795476241237350
- Bieneck V, Decker A, Schmitt-Graeff A, Kreisel W, Schauer F. Remission of refractory esophageal lichen planus induced by tofacitinib. Z Gastroenterol 2024; 62: 1384–1388. https://doi.org/10.1055/a-2300-0375
- Kozlov M, Levit EK, Silvers DN, Brichkov I. Severe esophageal lichen planus treated with tofacitinib. Cutis 2023; 111: 155–163. https://doi.org/10.12788/cutis.0717