ORIGINAL ARTICLE
Hospital Use, Morbidity, and Cancer Risk by Age Group in Neurofibromatosis Type 1: A Nationwide Retrospective Cohort Study
Minsu KIM1  , Suhyun HAN2 , Chong Won CHOI1 , Bo Ri KIM1 and Sang Woong YOUN1
, Suhyun HAN2 , Chong Won CHOI1 , Bo Ri KIM1 and Sang Woong YOUN1
1Department of Dermatology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Republic of Korea, and 2Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
Neurofibromatosis type 1 (NF1) affects multiple organs progressively, leading to a shortened life expectancy. This study aimed to identify the complications that are prominent in each age group by comparing 28,082 patients with NF1 and 84,246 matched controls. Benign and malignant neoplasms along with neurological complications were the primary contributors to hospital use across most age groups. Respiratory and circulatory disorders were a common cause of hospital use in children and older adults, respectively. Except for soft tissue and central nervous system-originated malignancies, which are well-established NF1-related tumours, the highest rate ratios (RR) of malignancies with statistical significance was observed in the adrenal gland (0–9 years, RR 50.67, 95% CI 6.74–380.76); female genital organs (10–14 years, RR 12.06, 95% CI 1.35–107.93); respiratory and intrathoracic organs (15–19 years, RR 15.10, 95% CI 1.76–129.22; 20–29 years, RR 7.59, 95% CI 2.94–19.56; ≥ 60 years, RR 1.38, 95% CI 1.18–1.61); lip, oral cavity, and pharynx (30–39 years, RR 6.11, 95% CI 1.53–24.42); and bone and articular cartilage (40–49 years, RR 3.06, 95% CI 1.37–6.81; 50–59 years, RR 4.73, 95% CI 2.35–9.50). Comorbidities and malignancies that predominantly affect patients vary by age group; physicians should be aware of the appropriate management strategies throughout their lifespan.
SIGNIFICANCE
Neurofibromatosis type 1 invades various organs simultaneously and is accompanied by diverse comorbidities and malignancies. We identified which system imposes the greatest health-related burden on patients with neurofibromatosis type 1 in each age group. Malignant and benign tumours as well as neurological complications posed significant burdens throughout the lifespan of patients with neurofibromatosis type 1. However, the primary reasons for hospital use and the types of malignancies that occurred varied by age group. Comorbidities commonly observed at each stage of life must be thoroughly understood to provide comprehensive treatment for patients with neurofibromatosis type 1.
Key words: neurofibromatosis 1; genetic skin disease; comorbidity; cancer; epidemiology.
Citation: Acta Derm Venereol 2025; 105: adv43416. DOI: https://doi.org/10.2340/actadv.v105.43416.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 19, 2025. Accepted after revision: Jun 5, 2025. Published: Jun 25, 2025.
Corr: Bo Ri Kim, MD, PhD, and Sang Woong Youn, MD, PhD, Department of Dermatology, Seoul National University Bundang Hospital, 82 Gumi-Ro 173 Beon-Gil, Seongnam, Gyeonggi 13620, Korea. E-mails: kbori87@naver.com; swyoun@snu.ac.kr
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by the Seoul National University Bundang Hospital Research Fund, 02-2024-0037.
INTRODUCTION
Neurofibromatosis type 1 (NF1) is a genetic disorder accompanying various clinical manifestations, including numerous benign and malignant neoplasms (1). They result in a reduction in life expectancy of approximately 8–20 years compared with the general population (2, 3).
Because of the multisystemic nature of the disease, patients with NF1 frequently require multidisciplinary treatment, which places a considerable burden on both patients and physicians (4, 5). Therefore, a comprehensive understanding of comorbidities across the lifespan of these patients, as well as their impact on the national healthcare system, is essential for adequate treatment. However, most studies examining comorbidities in patients with NF1 have focused on mortality data, emphasizing complications that contribute to death (2, 3, 6–9). Although several epidemiological studies have investigated comorbidities throughout the lifespan of patients with NF1, these analyses have primarily been limited to hospitalized patients’ records (10, 11).
Korea has a national health insurance system that provides coverage for most patients. Additionally, rare disorders, including NF1, are designated as conditions requiring specialized management, ensuring that patients can access hospitals without financial barriers. Along with these, Korea’s high accessibility to medical care is expected to facilitate more comprehensive and detailed patient research.
We aimed to analyse the outpatient and inpatient medical history of patients diagnosed with NF1 to identify all comorbidities, including relatively mild conditions, and to determine whether major changes in disease patterns occur with age. Understanding which organ systems are primarily affected at each stage of life may aid in the efficient management of NF1 and development of treatment guidelines.
MATERIALS AND METHODS
Study design and data source
A population-based retrospective cohort study was conducted using the Health Insurance Review and Assessment (HIRA) database between 1 January 2009, and 31 December 2023 (HIRA research data: M20240820001). As more than 98% of Koreans are covered by a single national healthcare system, the HIRA dataset provides overall medical information on each patient by anonymously reviewing them using personal registration codes.
Study population
Korea has a registration programme to aid financially patients with rare and intractable diseases, including NF1. After confirmation by specialists that patients meet the clinical diagnostic criteria and have undergone adequate radiological evaluation, those diagnosed with NF1 are assigned a V156 diagnostic code, which is highly reliable.
The NF1 group included patients whose medical records contained the V156 code or the International Classification of Diseases, 10th revision (ICD-10) code for neurofibromatosis (Q85.0). Patients with any other phacomatoses, not elsewhere classified (Q85) diagnostic codes (tuberous sclerosis [Q85.1], other phacomatoses, not elsewhere classified [Q85.8], phacomatosis, unspecified [Q85.9]) were excluded. As NF1 and neurofibromatosis type 2 cannot be distinguished based on ICD-10 codes, as with a previous study, patients with records of diagnostic codes for benign neoplasm of meninges (D32) or benign neoplasm of cranial nerves (D33.3), which indicate a diagnosis of neurofibromatosis type 2, were additionally excluded (11).
Because extracting data from the general population was not possible, the control group was defined as patients with diagnostic codes for haemangioma (D18.0). In the Korean system, since 2011, it has been possible to distinguish patients with haemangiomas of the skin and soft tissue from those with haemangiomas of other origins. Therefore, they were selected as the control group because they are associated with fewer systemic complications and comorbidities (12). Patients whose records contained the ICD-10 code Q85.0 were excluded. Each patient with NF1 was matched to 3 controls according to sex and birth year.
Evaluation of hospital use patterns and comorbidities
Every hospital visit was examined irrespective of the date of NF1 diagnosis because NF1 is a congenital disorder. To make the control group representative of the general population, hospital visits associated with the primary diagnosis of haemangioma were excluded.
Hospital use patterns were classified according to the main diagnostic group for the primary diagnosis at each visit. Absolute excess risk (AER) was calculated for hospital use in each diagnostic group by subtraction; that is, we analysed how many more times patients with NF1 used outpatient or inpatient hospital care for each diagnostic group per 10,000 person-years.
The incidence rate was calculated to analyse comorbidities. Incidence was defined as at least 1 hospitalization or 3 outpatient visits for any primary or all secondary diagnoses. Detailed diagnostic codes of the comorbidities used for analysis are provided in Table SI.
Statistical analysis
Continuous and categorical variables were compared using Student’s t-test, Pearson’s χ2 test or Fisher’s exact test, as appropriate.
For overall cancer cases, the standardized incidence ratio (SIR) was calculated at 1-year age intervals by sex. The trend line was determined using locally estimated scatterplot smoothing method.
Statistical analyses were performed using R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Clinical characteristics
Altogether, 28,082 patients with NF1 were matched to 84,246 patients in the control group (Table I, Fig. 1). Among patients with NF1, 18.5% were diagnosed with any type of cancer at least once during the observation period, which was significantly higher than that of the control group (12.9%, p < 0.001). Age at first diagnosis of any cancer was also low in the NF1 group (50.22 ± 19.25 years vs 56.92 ± 15.74 years, p < 0.001).
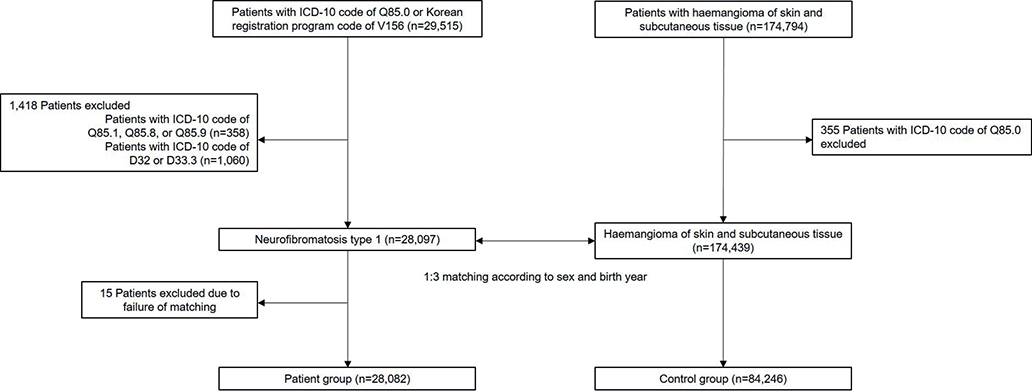
Fig. 1. Flowchart of study population selection. ICD-10: International Classification of Diseases, 10th revision
Hospital use
Compared with those of controls, patients with NF1 showed a significantly higher number of admissions (6.26 ± 19.59 vs 5.44 ± 29.57, p < 0.001), length of each hospitalization (6.24 ± 5.28 days vs 5.22 ± 4.37 days, p < 0.001), and total length of hospitalization (59.85 ± 256.84 days vs 39.28 ± 209.41 days, p < 0.001). The number of outpatient clinic visits was also high, but it failed to reach statistical significance (248.31 ± 242.96 vs 246.92 ± 239.94, p = 0.40).
Specifically, regarding outpatient clinic visits and inpatient hospitalizations, treatments related to neoplasms, the nervous system, and mental and behavioural disorders showed high AER (Table SII). Hospitalizations related to mental and behavioural disorders had the longest hospitalization days per admission (15.18 ± 10.79 days) and total hospitalization days (335.17 ± 784.88 days).
Analysing which diagnostic groups-related hospital use was more prominent by age group, a high AER was confirmed in neoplasms and nervous system disorders in both outpatient and inpatient settings across most age groups (Fig. 2, Table SIII). Additionally, the AER of hospital use was high owing to problems related to the respiratory system in the younger age group and circulatory system in the older age group. Hospital use because of mental and behavioural disorders was prominent in both pre-adulthood and old age.
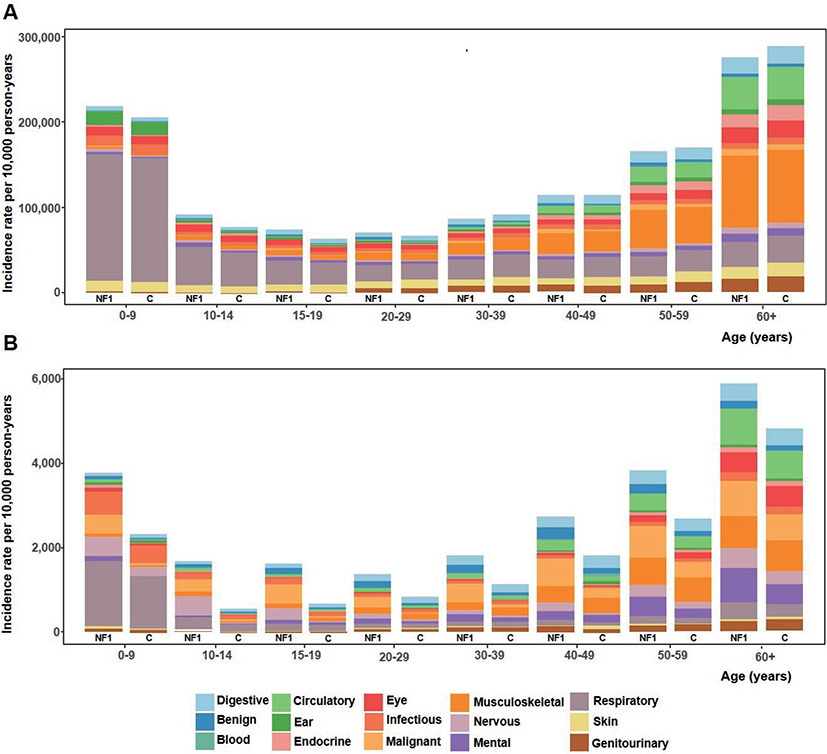
Fig. 2. Incidence rate for each main diagnostic group according to age group in the neurofibromatosis type 1 (NF1) group and control (C) group for (A) outpatient clinic visits and (B) inpatient hospitalizations.
Morbidities
In patients with NF1, we noticed especially high rate ratios (RR) for other congenital malformations of the central nervous system (CNS; RR 14.71, 95% CI 5.61–38.54), Arnold Chiari malformation (RR 7.66, 95% CI 3.37–17.39), mental retardation (RR 5.73, 95% CI 4.91–6.68), and hydrocephaly (RR 4.76, 95% CI 3.95–5.74), which are well-known complications associated with NF1 (Table II) (11).
Comorbidities with an RR over 2.0 included optic neuritis (RR 3.27, 95% CI 2.55–4.18), psychological development disorder (RR 3.02, 95% CI 2.59–3.52), renovascular hypertension (RR 2.77, 95% CI 1.79–4.30), multiple sclerosis (RR 2.55, 95% CI 1.63–4.00), lack of expected normal physiological development (RR 2.49, 95% CI 2.23–2.77), disorders of continuity of bone (RR 2.40, 95% CI 2.03–2.84), adult respiratory distress syndrome (RR 2.37, 95% CI 1.58–3.56), emphysema (RR 2.29, 95% CI 2.05–2.56), other disorders of CNS (RR 2.25, 95% CI 1.46–3.46), attention-deficit hyperactivity disorder (RR 2.06, 95% CI 1.87–2.26), visual impairment including blindness (RR 2.03, 95% CI 1.63–2.53), and scoliosis (RR 2.00, 95% CI 1.86–2.14).
Some disorders, including type 2 diabetes mellitus (RR 0.92, 95% CI 0.89–0.95), viral hepatitis (RR 0.87, 95% CI 0.82–0.92), alcoholic liver disease (RR 0.84, 95% CI 0.78–0.91), and obesity (RR 0.66, 95% CI 0.53–0.82), were observed at low rates in patients with NF1 (Table SIV).
Cancer risk
Patients with NF1 showed the highest RRs for malignancies of the spinal cord (RR 199.28, 95% CI 27.65–1436.09) and cranial nerves (RR 88.95, 95% CI 32.83–241.00), primarily driven by a significant increase in optic nerve tumours. Elevated risks were also observed for malignancies of the small intestine (RR 26.90, 95% CI 18.32–39.51), brain (RR 8.47, 95% CI 6.82–10.53), meninges (RR 7.88, 95% CI 3.29–18.86), and mesothelial and soft tissue (RR 6.87, 95% CI 6.01–7.86), which includes malignant peripheral nerve sheath tumours (Table III). Hepatocellular carcinoma (HCC; RR 0.78, 95% CI 0.64–0.94) and non-melanoma skin cancer (NMSC; RR 0.82, 95% CI 0.69–0.98) were less frequently observed in patients with NF1. However, NMSC was detected at a significantly younger age in patients with NF1 (61.99 ± 17.46 years vs 66.91 ± 16.85 years, p = 0.002).
As shown in Fig. 3, the SIR of total malignancies was high in the younger age groups. In particular, compared with controls, the risk of malignancies of mesothelial and soft tissue, and eye, brain, and other parts of the CNS was high in all age groups of patients with NF1 (Table SV). Aside from these, the highest RR with statistical significance was observed in malignancies of the thyroid and other endocrine glands in the 0–9 years group (RR 16.89, 95% CI 4.95–57.64), in which incidence was detected solely from the adrenal gland (incidence rate 4.55/10,000 person-years, RR 50.67, 95% CI 6.74–380.76). For the 10–14 years group, the highest RR was observed in malignancies of the female genital organs (RR 12.06, 95% CI 1.35–107.93), with the highest incidence rate in the ovary (1.42/10,000 person-years), followed by the vulva and vagina (0.47/10,000 person-years). The highest RR was observed in malignancies of the respiratory and intrathoracic organs in the 15–19 years group (RR 15.10, 95% CI 1.76–129.22) and 20–29 years group (RR 7.59, 95% CI 2.94–19.56). Specifically, in the 15–19 years group, the highest incidence rate was observed in the heart, mediastinum, and pleura (1.75/10,000 person-years), whereas in the 20–29 years group, it was observed in the bronchus and lung (1.76/10,000 person-years). Additionally, the highest RR was detected in malignancies of the lip, oral cavity, and pharynx (30–39 years, RR 6.11, 95% CI 1.53–24.42); bone and articular cartilage (40–49 years, RR 3.06, 95% CI 1.37–6.81; 50–59 years, RR 4.73, 95% CI 2.35–9.50); and respiratory and intrathoracic organs (≥ 60 years, RR 1.38, 95% CI 1.18–1.61). Lymphoid, hematopoietic, and related tissue malignancies were prominent before the age of 30 years, in contrast to breast cancer, which showed a high risk in patients aged 30–59 years. Although not statistical significant, NMSC showed a high rate in the NF1 group before 50 years of age; however, after that age, the risk was reversed.
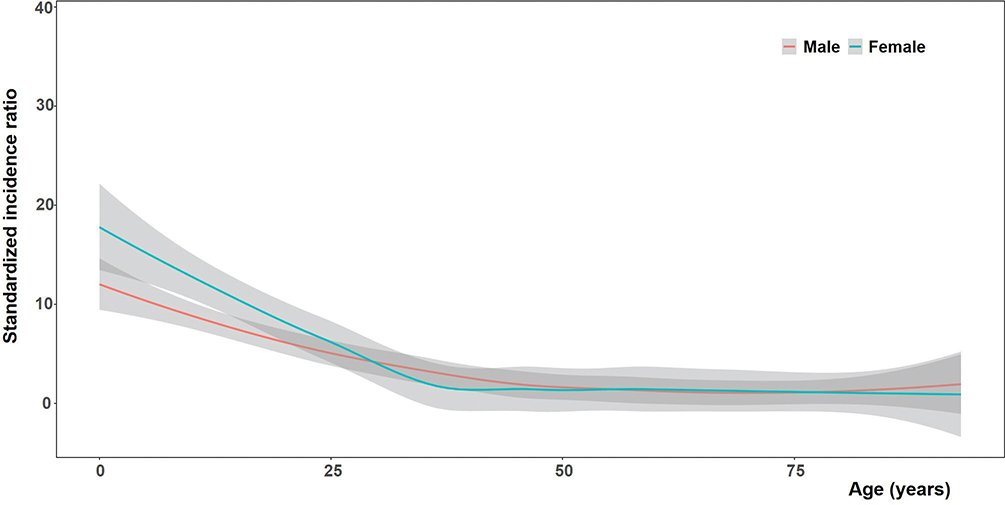
Fig. 3. Standardized incidence ratio of malignancy in patients with neurofibromatosis type 1 compared with that in the control group according to age and sex.
DISCUSSION
As NF1 is a progressive disorder affecting multiple organs throughout life, patients with NF1 experience prolonged hospital stays because of various comorbidities and malignancies. In this study, we aimed to comprehensively explore hospital use, morbidity, and cancer risk in patients with NF1, particularly according to age group, and to investigate which systemic complications are prominent at different life stages.
In our cohort, the period prevalence of NF1 was approximately 1 in 1,840 individuals, which was higher than the pooled prevalence of 1 in 3,164 individuals (95% CI 1 in 2,132–1 in 4,712) reported in a recent study (13). This difference may be due to early and sensitive detection in Korea, facilitated by regular infant checkups, a registration programme that provides financial support for patients with NF1, and high medical accessibility.
Among non-neoplastic comorbidities, neurological disorders contributed to hospital utilization across almost all age groups in patients with NF1. We reinforced the findings of an American study that observed an increased risk of epilepsy, Parkinson’s disease, and multiple sclerosis (14). The marginally increased rate of headache supports a previous study reported that headache is not specific to NF1 and is not always secondary to NF1-related CNS deformities (15). Considering their chronic and neuropathic nature, however, physicians should pay attention not only to the overt diseases accompanying NF1 but also to non-specific symptoms that affect quality of life (16).
Several psychiatric disorders were also associated with NF1, particularly in pre-adulthood and older ages. Studies have shown early developmental delays in infants with NF1, especially in motor functioning and communication skills (17, 18). Moreover, significant depression and anxiety have been reported in adolescent patients (19). Therefore, early evaluation and intervention may be crucial for improving development and mental health. Regarding older adults, we reaffirmed the high risk of dementia in patients with NF1, consistent with findings from Finnish research (20). Unlike findings from a Danish cohort study, we observed an increased risk of bipolar disorder and schizophrenia in patients with NF1 (21).
To date, it has been noted that respiratory comorbidities of NF1, such as interstitial lung diseases and pulmonary hypertension, primarily appear in adulthood (22). In an Italian study, the increase in mortality because of respiratory diseases was significant only in patients aged > 40 years (3). While controversy remains regarding the true association between interstitial lung diseases, including pulmonary fibrosis, and NF1, we did not find a significant association between these conditions (23). Instead, we recognized a prominent excess of hospital use because of respiratory problems during childhood, which seems to have been underestimated. Accordingly, recent studies have found a common presence of diffuse lung disease in paediatric patients with NF1 and a comparable rate of abnormal structural findings in the lungs, except for pulmonary cysts, between different age groups, including those under the age of 12 (24, 25). Respiratory problems in childhood may not have received attention as a complication of NF1 so far, as NF1 is occasionally diagnosed late because it takes time for affected individuals to meet the diagnostic criteria. Considering the vagueness of symptoms in children, physicians should inform caregivers of the risks and symptoms of respiratory complications.
Conversely, circulatory problems imposed an increased hospitalization burden on older adults. Vasculopathy is a well-known morbidity in patients with NF1 and a Swedish study revealed that hypertension was significantly related to higher mortality (6, 26). However, contrary to respiratory comorbidities, vascular disease was associated with mortality before the age of 29 years but not with the older patients (7). The discrepancy between the impact on mortality and hospital utilization patterns across age groups for respiratory and circulatory complications highlights the importance of the current study, which also analysed medical care use, which, even if it may not directly affect mortality, can have a serious impact on patients’ lives.
Consistent with previous studies, we found a low rate of type 2 diabetes mellitus in patients with NF1 (27, 28). Although the underlying mechanism has not been fully elucidated, the possibility of Ras signalling involvement has been suggested (27). We also recognized a low prevalence of obesity, as previous studies have observed a lower body mass index, particularly in men, than in the general population, possibly owing to altered metabolism (29–32). The reduced prevalence of these risk factors for HCC, as well as that of other risk factors, including alcoholic liver disease and viral hepatitis, may ultimately explain the reduced risk of HCC in this cohort (33). Although previous studies reported a high risk of liver cancer, they included all subtypes of cancer originating from the liver and intrahepatic bile ducts (11, 34). Regarding NMSC, however, considering the low age of first diagnosis in the NF1 group and the higher rate of incidence before age of 50, patients with NF1 seem to be more susceptible to NMSC. We believe that NMSC was less frequently detected in patients with NF1 because of their shorter life expectancy, as the age distribution of NMSC is concentrated in older individuals.
In general, the significant contribution of malignancies to morbidity and mortality in patients with NF1 is well established. Changes in SIR according to age and sex showed similar patterns to those observed in Finnish and French studies, with SIR being greatest before the age of 15 years, higher in women, reversing around the age of 25 years, and then reversing again around the age of 50 (11, 35). Our data also support previous studies that reported an increased incidence of leukaemia in children and a high risk of breast cancer in young women with NF1 (7, 36–38). The significance of the increased risk was lost after the age of 30 years for haematologic malignancies and after the age of 60 years for breast cancer. This suggests the necessity of age-specific screening guidelines for these diseases in patients with NF1. Small intestinal cancer also showed a remarkably high rate, consistent with previous studies (11, 34).
Except for the aforementioned NF1-related malignancies, we analysed the types of cancer that showed a relatively higher rate compared with that of the control group for each age group. We observed the highest risk of malignancy in the adrenal glands in the 0–9 years group. Pheochromocytoma is known to be an NF1-related tumour, and while some cases are malignant, its mean age of onset has been reported to be later than that associated with other genetic diseases (39). Although detailed diagnostic codes could not be identified, the discovery of NF1 gene mutations in a subset of paediatric patients with pheochromocytoma, along with our findings, implies their association from an early age (40). The risk was high for malignancies of the intrathoracic organs in both the 15–19 years and 20–29 years groups, but the specific sites of high incidence differed. Unlike the general population, because the incidence of tumours is high from an early age in patients with NF1, and symptom complaints may be ambiguous at a young age, it is necessary to consider the development of screening criteria based on these results.
Limitations
The main limitations of this study are that it was conducted in a single racial population and that a completely randomly selected general population could not be used as the control. Additionally, surveillance bias may have influenced our findings, as patients with NF1 are likely to undergo more frequent medical evaluations, potentially leading to overestimation of certain RRs. Nevertheless, our additional analysis of outpatient use history, combined with nationwide claims data, enabled detection of even relatively mild complications. This approach provides a more comprehensive understanding of the clinical burden and comorbidity profile of NF1 across different age groups.
Conclusion
NF1 is associated with various non-neoplastic and neoplastic comorbidities, resulting in an increased burden on hospital utilization across multiple diagnostic groups. This study characterized the pattern of organ involvement and malignancies that frequently occurred according to age group, which may benefit physicians in optimizing the management of patients with NF1 suffering from diverse comorbidities.
ACKNOWLEDGEMENTS
The authors thank Zarathu Co, Ltd for performing the statistical analyses.
IRB approval status: The study was approved by the Institutional Review Board of Seoul National University Bundang Hospital; IRB no. X-2410-930-904.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Gutmann DH, Ferner RE, Listernick RH, Korf BR, Wolters PL, Johnson KJ. Neurofibromatosis type 1. Nat Rev Dis Primers 2017; 3: 17004. https://doi.org/10.1038/nrdp.2017.4
- Evans DG, O’Hara C, Wilding A, Ingham SL, Howard E, Dawson J, et al. Mortality in neurofibromatosis 1: in North West England: an assessment of actuarial survival in a region of the UK since 1989. Eur J Hum Genet 2011; 19: 1187–1191. https://doi.org/10.1038/ejhg.2011.113
- Masocco M, Kodra Y, Vichi M, Conti S, Kanieff M, Pace M, et al. Mortality associated with neurofibromatosis type 1: a study based on Italian death certificates (1995–2006). Orphanet J Rare Dis 2011; 6: 11. https://doi.org/10.1186/1750-1172-6-11
- Oates EC, Payne JM, Foster SL, Clarke NF, North KN. Young Australian adults with NF1 have poor access to health care, high complication rates, and limited disease knowledge. Am J Med Genet A 2013; 161A: 659–666. https://doi.org/10.1002/ajmg.a.35840
- Kokkinou E, Roka K, Alexopoulos A, Tsina E, Nikas I, Krallis P, et al. Development of a multidisciplinary clinic of neurofibromatosis type 1 and other neurocutaneous disorders in Greece: a 3-year experience. Postgrad Med 2019; 131: 445–452. https://doi.org/10.1080/00325481.2019.1659708
- Zoller M, Rembeck B, Akesson HO, Angervall L. Life expectancy, mortality and prognostic factors in neurofibromatosis type 1: a twelve-year follow-up of an epidemiological study in Goteborg, Sweden. Acta Derm Venereol 1995; 75: 136–140. https://doi.org/10.2340/0001555575136140
- Rasmussen SA, Yang Q, Friedman JM. Mortality in neurofibromatosis 1: an analysis using U.S. death certificates. Am J Hum Genet 2001; 68: 1110–1118. https://doi.org/10.1086/320121
- Duong TA, Sbidian E, Valeyrie-Allanore L, Vialette C, Ferkal S, Hadj-Rabia S, et al. Mortality associated with neurofibromatosis 1: a cohort study of 1895 patients in 1980–2006 in France. Orphanet J Rare Dis 2011; 6: 18. https://doi.org/10.1186/1750-1172-6-18
- Uusitalo E, Leppavirta J, Koffert A, Suominen S, Vahtera J, Vahlberg T, et al. Incidence and mortality of neurofibromatosis: a total population study in Finland. J Invest Dermatol 2015; 135: 904–906. https://doi.org/10.1038/jid.2014.465
- Kenborg L, Duun-Henriksen AK, Dalton SO, Bidstrup PE, Doser K, Rugbjerg K, et al. Multisystem burden of neurofibromatosis 1 in Denmark: registry- and population-based rates of hospitalizations over the life span. Genet Med 2020; 22: 1069–1078. https://doi.org/10.1038/s41436-020-0769-6
- Diaz E, Bergqvist C, Peiffer B, Fertitta L, Jannic A, Ferkal S, et al. In-hospital clinical features, morbidity, and mortality of patients with neurofibromatosis 1 in France: a nationwide, population-based retrospective cohort study. J Invest Dermatol 2023; 143: 2408–2415 e7. https://doi.org/10.1016/j.jid.2023.04.034
- Maguiness SM, Frieden IJ. Current management of infantile hemangiomas. Semin Cutan Med Surg 2010; 29: 106–114. https://doi.org/10.1016/j.sder.2010.03.009
- Lee TJ, Chopra M, Kim RH, Parkin PC, Barnett-Tapia C. Incidence and prevalence of neurofibromatosis type 1 and 2: a systematic review and meta-analysis. Orphanet J Rare Dis 2023; 18: 292. https://doi.org/10.1186/s13023-023-02911-2
- Madubata CC, Olsen MA, Stwalley DL, Gutmann DH, Johnson KJ. Neurofibromatosis type 1 and chronic neurological conditions in the United States: an administrative claims analysis. Genet Med 2015; 17: 36–42. https://doi.org/10.1038/gim.2014.70
- Clementi M, Battistella PA, Rizzi L, Boni S, Tenconi R. Headache in patients with neurofibromatosis type 1. Headache 1996; 36: 10. https://doi.org/10.1046/j.1526-4610.1996.3601010.x
- Kongkriangkai AM, King C, Martin LJ, Wakefield E, Prada CE, Kelly-Mancuso G, et al. Substantial pain burden in frequency, intensity, interference and chronicity among children and adults with neurofibromatosis Type 1. Am J Med Genet A 2019; 179: 602–607. https://doi.org/10.1002/ajmg.a.61069
- Lorenzo J, Barton B, Acosta MT, North K. Mental, motor, and language development of toddlers with neurofibromatosis type 1. J Pediatr 2011; 158: 660–665. https://doi.org/10.1016/j.jpeds.2010.10.001
- Kolesnik AM, Jones EJH, Garg S, Green J, Charman T, Johnson MH, et al. Early development of infants with neurofibromatosis type 1: a case series. Mol Autism 2017; 8: 62. https://doi.org/10.1186/s13229-017-0178-0
- Cavallo ND, Maggi G, Ferraiuolo F, Sorrentino A, Perrotta S, Carotenuto M, et al. Neuropsychiatric manifestations, reduced self-esteem and poor quality of life in children and adolescents with neurofibromatosis type 1 (NF1): the impact of symptom visibility and bullying behavior. Children (Basel) 2023; 10: 330. https://doi.org/10.3390/children10020330
- Kallionpaa RA, Valtanen M, Auranen K, Uusitalo E, Rinne JO, Peltonen S, et al. Increased risk for dementia in neurofibromatosis type 1. Genet Med 2021; 23: 2219–2222. https://doi.org/10.1038/s41436-021-01261-3
- Kenborg L, Andersen EW, Duun-Henriksen AK, Jepsen JRM, Doser K, Dalton SO, et al. Psychiatric disorders in individuals with neurofibromatosis 1 in Denmark: a nationwide register-based cohort study. Am J Med Genet A 2021; 185: 3706–3716. https://doi.org/10.1002/ajmg.a.62436
- Reviron-Rabec L, Girerd B, Seferian A, Campbell K, Brosseau S, Bergot E, et al. Pulmonary complications of type 1 neurofibromatosis. Rev Mal Respir 2016; 33: 460–473. https://doi.org/10.1016/j.rmr.2014.09.010
- Ryu JH, Parambil JG, McGrann PS, Aughenbaugh GL. Lack of evidence for an association between neurofibromatosis and pulmonary fibrosis. Chest 2005; 128: 2381–2386. https://doi.org/10.1378/chest.128.4.2381
- Spinnato P, Facchini G, Tetta C, Lotrecchiano L, Colangeli M, Bazzocchi A, et al. Neurofibromatosis type-1-associated diffuse lung disease in children. Pediatr Pulmonol 2019; 54: 1760–1764. https://doi.org/10.1002/ppul.24481
- Avanesov M, Well L, Laqmani A, Derlin T, Riccardi VM, Adam G, et al. Structural alteration of lung parenchyma in patients with NF1: a phenotyping study using multidetector computed tomography (MDCT). Orphanet J Rare Dis 2021; 16: 29. https://doi.org/10.1186/s13023-021-01672-0
- Oderich GS, Sullivan TM, Bower TC, Gloviczki P, Miller DV, Babovic-Vuksanovic D, et al. Vascular abnormalities in patients with neurofibromatosis syndrome type I: clinical spectrum, management, and results. J Vasc Surg 2007; 46: 475–484. https://doi.org/10.1016/j.jvs.2007.03.055
- Kallionpaa RA, Peltonen S, Leppavirta J, Poyhonen M, Auranen K, Jarvelainen H, et al. Haploinsufficiency of the NF1 gene is associated with protection against diabetes. J Med Genet 2021; 58: 378–384. https://doi.org/10.1136/jmedgenet-2020-107062
- Kenborg L, Ebbehoj A, Ejerskov C, Handrup MM, Ostergaard JR, Hove H, et al. Endocrine morbidity in neurofibromatosis 1: a nationwide, register-based cohort study. Eur J Endocrinol 2023; 189: 190–198. https://doi.org/10.1093/ejendo/lvad101
- Koga M, Yoshida Y, Imafuku S. Nutritional, muscular and metabolic characteristics in patients with neurofibromatosis type 1. J Dermatol 2016; 43: 799–803. https://doi.org/10.1111/1346-8138.13218
- Basto DL, de Souza Vieira G, Andrade-Losso RM, Almeida PN, Riccardi VM, Rozza-de-Menezes RE, et al. Head circumference and anthropometric changes and their relation to plexiform and skin neurofibromas in sporadic and familial neurofibromatosis 1 Brazilian adults: a cross-sectional study. Orphanet J Rare Dis 2022; 17: 341. https://doi.org/10.1186/s13023-022-02482-8
- Souza MLR, Jansen AK, Rodrigues LOC, Vilela DLS, Kakehasi AM, Martins AS, et al. Increased resting metabolism in neurofibromatosis type 1. Clin Nutr ESPEN 2019; 32: 44–49. https://doi.org/10.1016/j.clnesp.2019.05.006
- Tritz R, Benson T, Harris V, Hudson FZ, Mintz J, Zhang H, et al. Nf1 heterozygous mice recapitulate the anthropometric and metabolic features of human neurofibromatosis type 1. Transl Res 2021; 228: 52–63. https://doi.org/10.1016/j.trsl.2020.08.001
- Gupta A, Das A, Majumder K, Arora N, Mayo HG, Singh PP, et al. Obesity is independently associated with increased risk of hepatocellular cancer-related mortality: a systematic review and meta-analysis. Am J Clin Oncol 2018; 41: 874–881. https://doi.org/10.1097/COC.0000000000000388
- Seminog OO, Goldacre MJ. Risk of benign tumours of nervous system, and of malignant neoplasms, in people with neurofibromatosis: population-based record-linkage study. Br J Cancer 2013; 108: 193–198. https://doi.org/10.1038/bjc.2012.535
- Uusitalo E, Rantanen M, Kallionpaa RA, Poyhonen M, Leppavirta J, Yla-Outinen H, et al. Distinctive cancer associations in patients with neurofibromatosis type 1. J Clin Oncol 2016; 34: 1978–1986. https://doi.org/10.1200/JCO.2015.65.3576
- Kampitsi CE, Nordgren A, Mogensen H, Ponten E, Feychting M, Tettamanti G. Neurocutaneous syndromes, perinatal factors, and the risk of childhood cancer in Sweden. JAMA Netw Open 2023; 6: e2325482. https://doi.org/10.1001/jamanetworkopen.2023.25482
- Wang X, Levin AM, Smolinski SE, Vigneau FD, Levin NK, Tainsky MA. Breast cancer and other neoplasms in women with neurofibromatosis type 1: a retrospective review of cases in the Detroit metropolitan area. Am J Med Genet A 2012; 158A: 3061–3064. https://doi.org/10.1002/ajmg.a.35560
- Seminog OO, Goldacre MJ. Age-specific risk of breast cancer in women with neurofibromatosis type 1. Br J Cancer 2015; 112: 1546–1548. https://doi.org/10.1038/bjc.2015.78
- Welander J, Soderkvist P, Gimm O. Genetics and clinical characteristics of hereditary pheochromocytomas and paragangliomas. Endocr Relat Cancer 2011; 18: R253–276. https://doi.org/10.1530/ERC-11-0170
- Bausch B, Wellner U, Bausch D, Schiavi F, Barontini M, Sanso G, et al. Long-term prognosis of patients with pediatric pheochromocytoma. Endocr Relat Cancer 2014; 21: 17–25. https://doi.org/10.1530/ERC-13-0415