RESEARCH LETTER
Development of Multiple Cherry Haemangiomas in a Patient with Androgenetic Alopecia after Topical Minoxidil Use
Xiao-shuang YANG, Ru DAI and Zhong-fa LYU*
Department of Dermatology, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, P.R. China. *E-mail: lzfskin@zju.edu.cn
Citation: Acta Derm Venereol 2025; 105: adv43447. DOI: https://doi.org/10.2340/actadv.v105.43447.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 24, 2025; Accepted after revision: Mar 31, 2025. Published: Apr 29, 2025
Competing interests and funding: The authors have no conflicts of interest to declare.
Dear Editor,
A 35-year-old male, in robust health, revisited our hospital for a follow-up consultation concerning “progressive thinning of hair on the crown and forehead over 14 years”. Initially presenting 14 years earlier with hair loss, he was diagnosed with Hamilton–Norwood IV androgenetic alopecia and commenced on oral finasteride (1 mg/day) combined with topical 5% minoxidil (1). Hair loss improved after 1 year, leading him to discontinue finasteride independently while continuing minoxidil for an additional year. He noted multiple red round papules on his scalp appearing in the second year of minoxidil use, which gradually enlarged but have increased in neither number nor size for the past 12 years post-discontinuation of minoxidil.
Physical examination 14 years ago revealed sparse hair across the crown and forehead, with a solitary, bright-red papule on the right side of the crown, approximately the size of a green bean (approximately 2.0 mm in diameter) (Fig. 1A). Current physical examination showed multiple isolated red papules scattered across the crown and forehead (area of application), varying in size from a soybean to a rice grain (numbers 1–5) approximately 3.8 mm, 3.6 mm, 0.7 mm, 0.9 mm, and 0.4 mm respectively in diameter). No rashes were observed in the occipital or temporal regions, nor were similar rashes evident elsewhere on the body (Fig. 1B, C). Dermoscopic examination revealed multiple clustered blood vessel networks, with distinct boundaries of red cavities (Fig. 1D). The histopathological presentation is characterized by reduced follicular structures and smaller dermal papillae. The haemangioma protrudes above the skin surface, presenting as endothelial-lined vascular cavities of varying sizes containing erythrocytes (Fig. 1E).
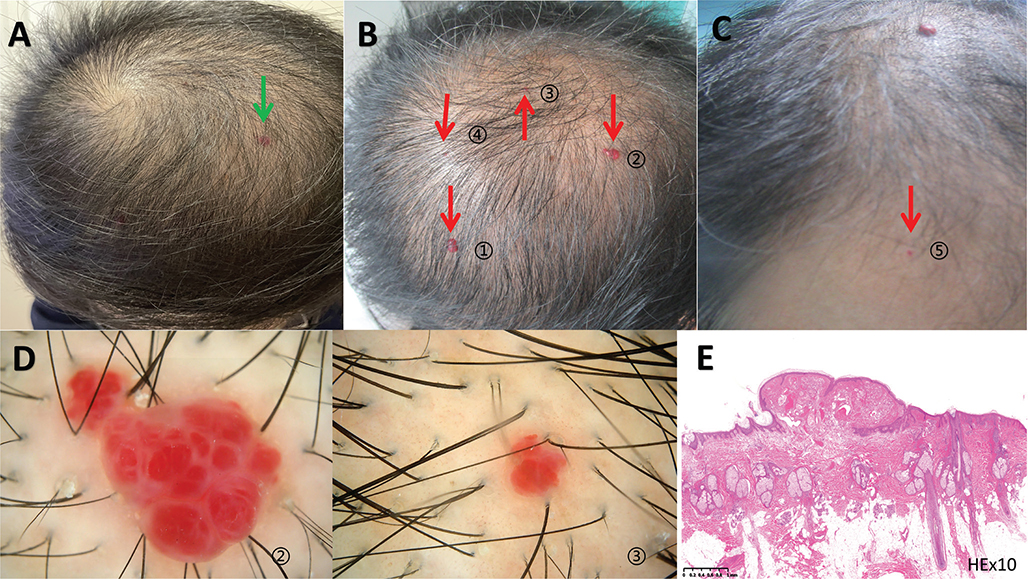
Fig. 1. Skin with 1 cherry angioma (approximately 2.0 mm in diameter) prior to the application of topical minoxidil. (A, green arrow) Scattered, multiple isolated bright-red papules on the crown and forehead (application area), varying from soybean to rice grain in size, 5 in total. (B ① ② ③ ④ and C ⑤ approximately 3.8 mm, 3.6 mm, 0.7 mm, 0.9 mm, and 0.4 mm respectively in diameter, red arrows). (D ② ③x50) Dermoscopic examination depicting multiple clustered blood vessel networks, with clearly demarcated red cavities. (E: haematoxylin-eosin x10) Histopathology shows reduced follicular structures, smaller dermal papillae, and a haemangioma protruding above the skin surface as endothelial-lined vascular cavities of varying sizes containing erythrocytes.
We attribute these findings to cherry angiomas induced by topical minoxidil. Given the benign nature of these lesions and their number, no specific treatment was administered; instead, follow-up observation was recommended.
The patient’s case is characterized by: (1) the sudden appearance of multiple cherry angiomas during the second year of using 5% minoxidil solution; (2) lesions exclusively confined to the areas of minoxidil application (crown and forehead); and (3) absence of new lesions or growth in the years following the cessation of minoxidil treatment. This phenomenon suggests that the cherry angiomas of our case are associated with topical minoxidil. Instances of cherry angiomas triggered by topical minoxidil are exceedingly rare, with only one other case reported (2). The pathogenesis of cherry angiomas remains elusive; research suggests a correlation between cherry angiomas and certain underlying conditions and adverse environmental exposures (3). This case indicates the angiogenic potential of minoxidil; The exact mechanism of minoxidil action is not yet known, but it is proposed to increase blood flow causing vasodilation and proliferation of blood vessels surrounding hair follicles and leading to an increase in vascular endothelial growth factor (VEGF) levels (4). Minoxidil may be considered an effective vasoactive agent for the stimulation of angiogenesis in rat cutaneous flaps (5, 6). But as our case has found, true angiogenesis visible to the naked eye in patients has so far rarely been reported. More cases and studies need to be identified.
ACKNOWLEDGEMENTS
This work was supported by the National Natural Science Foundation of China (82273553).
Written informed consent was obtained from the patient for this case report.
REFERENCES
- Norwood OT. Male pattern baldness: classification and incidence. South Med J 1975; 68: 1359–1365. https://doi.org/10.1097/00007611-197511000-00009
- Pavlovitch JH, Hubert H, Leibovitch J. Angiogenesis and minoxidil. Lancet 1990; 336: 889. https://doi.org/10.1016/0140-6736(90)92411-A
- Pastor-Tomás N, Bañuls J, Nagore E. Clinical relevance of cherry angiomas. Actas Dermosifiliogr 2023; 114: 240–246. https://doi.org/10.1016/j.ad.2022.10.040
- Yum S, Jeong S, Kim D, Lee S, Kim W, Yoo JW, et al. Minoxidil induction of VEGF is mediated by inhibition of HIF-prolyl hydroxylase. Int J Mol Sci 2017; 19: 53. https://doi.org/10.3390/ijms19010053
- Gümüş N, Odemiş Y, Yılmaz S, Tuncer E. Effect of topically applied minoxidil on the survival of rat dorsal skin flap. Aesthetic Plast Surg 2012; 36: 1382–1386. https://doi.org/10.1007/s00266-012-9966-2
- Gümüş N, Odemiş Y, Tuncer E, Yılmaz S. The effect of topical minoxidil pretreatment on nonsurgical delay of rat cutaneous flaps: further studies. Aesthetic Plast Surg 2013; 37: 809–815. https://doi.org/10.1007/s00266-013-0161-x