ORIGINAL REPORT
Assessing Atopic Dermatitis Control in Chinese Patients: Validation of the Chinese Version of Recap of Atopic Eczema Questionnaire (RECAP) and an Investigation into Its Interpretability
Junfen ZHANG1#, Shunmin ZHU2#, Liyan YUAN1, Xiaoling YU1, Shiqi LING1, Jiao ZHANG1 and Bin YANG1,2
1Dermatology Hospital, Southern Medical University, Guangzhou, 2School of Public Health, Southern Medical University, Guangzhou, China
#These authors share first authorship.
The lack of a validated Chinese version of the Recap of Atopic Eczema questionnaire (RECAP) questionnaire limits its applicability. This prospective study, conducted at a Chinese tertiary hospital between April and November 2024, aimed to evaluate measurement properties of the Chinese RECAP. Participants completed RECAP and reference instruments at baseline, 1–3 days, and 4–6 weeks. Construct validity was evaluated through hypothesis testing, while reliability was assessed using standard error of measurement (SEMagreement) and intraclass correlation coefficient (ICCagreement). Interpretability of both single and change scores was examined using anchor-based methods. In total, 153 adults with atopic dermatitis (AD) (mean age 28.4 years, 51.0% male) were included, with approximately half having moderate-to-severe disease. Of the predefined hypotheses, 57.1% (single score) and 71.4% (change score) were confirmed. The SEMagreement was 1.99, and the ICCagreement was 0.96. Final RECAP bandings were established, with a binary cutoff of ≥ 11 defining uncontrolled AD. The Smallest Detectable Change was 5.5. while the Minimally Important Change was 3.5 using the receiver operating characteristics (ROC) method and 0.6 after adjustment via predictive modelling. Our finding confirmed that the Chinese RECAP is a valid, reliable, and responsive tool for evaluating eczema control. An improvement of ≥ 6 represents a real and clinically meaningful change.
SIGNIFICANCE
Atopic dermatitis is a chronic skin disease with a relapsing-remitting disease course. The Recap of Atopic Eczema (RECAP) questionnaire was developed to measure how well atopic dermatitis is controlled. This study is the first to validate the Chinese version of RECAP and establish cutoff values for interpreting both single and change scores. Our findings highlight the influence of cultural differences on patients’ perception and reporting of eczema control.Moreover, we established population-specific interpretability thresholds, which are notably higher than those reported in previous studies.
Key words: atopic dermatitis; validity; reliability; responsiveness; interpretability; RECAP.
Citation: Acta Derm Venereol 2025; 105: adv43458. DOI: https://doi.org/10.2340/actadv.v105.43458.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 25, 2025. Accepted after revision: Jun 18, 2025. Published: Jul 8, 2025.
Corr: Bin Yang, Dermatology Hospital, Southern Medical University, Guangzhou, China, and School of Public Health, Southern Medical University, Guangzhou, China. E-mail: yangbin1@smu.edu.cn
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) is a chronic inflammatory skin disease that affects up to 10% of adults and 20% of children in high-income countries (1). In China, a nationwide population-based study estimated the 1-year prevalence of AD among adults at 6.0% (2). Due to its relapsing-remitting nature, AD imposes a significant burden on patients, impacting not only their physical health but also their psychological well-being and daily life (1). Given these challenges, long-term disease control has emerged as a core outcome in AD management, as emphasized by the Harmonizing Outcome Measures Eczema (HOME) initiative (3). Eczema control is a multifaceted construct encompassing symptom severity such as itch and sleep disturbance, functional impairment, emotional distress, and overall health-related quality of life (HRQoL) (3, 4). To comprehensively address these domains, the RECAP was developed (5) and subsequently recommended by the HOME initiative for measuring disease control in both clinical practice and research settings (6, 7).
While RECAP has been validated in multiple languages, including English (5, 8, 9), German (10), Dutch (11, 12), and Swedish (13), no validation study has been conducted for the Chinese version. Furthermore, the interpretability of RECAP scores – both single and change scores – has been examined only in Dutch (11, 12) and English populations (14). Cultural differences may influence how individuals perceive and report eczema control, particularly given that Chinese patients are generally more tolerant of disease symptoms compared with Western populations (15, 16). As a result, cutoff values established in Western populations may not be directly applicable to Chinese patients.
To our knowledge, the evaluation of disease control in AD patients using validated instruments has rarely been conducted in a Chinese population. A robust validation study of the Chinese version of RECAP, along with an investigation into its interpretability, could facilitate its adoption in routine clinical practice and research, ultimately enhancing patient-centred care.
Therefore, this study aims to evaluate the measurement properties of the Chinese versions of RECAP. Specifically, we assessed its construct validity, reliability, responsiveness, and interpretability to determine its suitability for measuring AD control in Chinese patients.
Materials and methods
Study design and population
This prospective study was conducted at the outpatient clinic of Dermatology Hospital, Southern Medical University, China, a specialized centre for the diagnosis and management of skin diseases (https://www.gdskin.com/). The study aimed to assess the measurement properties of RECAP, following the methodological guidelines established by the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) group (17, 18). The Chinese RECAP, previously translated by a Chinese research team, is available from the University of Nottingham’s Centre of Evidence Based Dermatology website (19).
Adults (aged ≥ 18 years) diagnosed with AD by a dermatologist based on the UK Working Party criteria (20), regardless of disease severity or ongoing treatments, were consecutively invited to participate between April and November 2024. After providing informed consent, participants were instructed to complete the RECAP questionnaire, reference instruments, and anchor measures at 3 time points via REDCap (https://projectredcap.org/): baseline (T0), 1–3 days after baseline (T1), and 4–6 weeks after baseline (T2) (Table SI). The reference instruments included the Atopic Dermatitis Control Tool (ADCT) (21), Patient-Oriented Eczema Measure (POEM) (22), Dermatology Life Quality Index (DLQI) (23), and Numerical Rating Scale (NRS) peak itch (24). The Patient’s Global Assessment (PtGA) of AD control (21) and the Global Rating of Change (GRC) scale (11, 12) were used as anchor measures at all 3 time points. Clinical disease severity was assessed by dermatologists using the Eczema Area and Severity Index (EASI) (25, 26), and the Investigator Global Assessment-AD (IGA) (27). The clinical data were extracted and merged with REDCap responses during analysis.
This non-interventional study was approved by the ethics committee of the Dermatology Hospital (reference: 2024027), and all participants provided digital informed consent.
RECAP
RECAP is a 7-item PROM that assesses symptoms, impact on daily activities and emotions, and acceptability, leading to a total score of 0–28, with higher scores indicating lower disease control (5).
Anchors
Patient’s Global Assessment of AD control. PtGA of AD control was used an anchor to interpret single scores (21). Patients were asked at each time point: “What is your overall impression of your atopic dermatitis control in the past week?”, with 5 response options: not at all, a little, moderately, mostly, and completely controlled.
Global Rating of Change scale. The GRC scale was used as an anchor for patient-perceived changes in eczema control at T1 and T2 (11, 12). It consists of 3 consecutive questions:
“Overall, has there been any change in the level of disease control in your atopic dermatitis since the last time you completed the RECAP?” (Response options: yes or no).
If yes, the next question assessed the direction and degree of change: “To what degree has the disease control of your atopic dermatitis changed?” (Response options: much/moderate/minor improvement or much/moderate/minor deterioration).
The final question assessed the importance of the change: “Was this change (improvement or deterioration) important to you?”(Response options: yes or no).
Patients were then categorized into 7 groups: no important change, important improvement (much/moderate/minor), and important deterioration (much/moderate/minor).
Statistical analysis
For all analyses, missing values were not imputed. SPSS Statistics for MacBook (V29.0; IBM Corp, Armonk, NY, USA) was used for all analyses.
Construct validity
Spearman’s rho (r) was used to test a priori hypotheses regarding the correlations between RECAP and reference instruments for single scores and change scores (see Tables II and III). Correlation strength was defined as: strong (+++) for r ≥ 0.7 (positive or negative), moderate (++) for 0.4 ≤ r < 0.7, and weak (+) for r < 0.4. For change-score validity (T0 and T2), 2 hypotheses were tested:
The correlation difference (∆r) between change scores of RECAP with PtGA of AD control vs that between reference instruments and PtGA of AD control was ≥ 0.1 (28).
Correlations between RECAP change scores and reference instruments measuring similar constructs were ≥ 0.5, while 0.3–0.5 for related but dissimilar constructs (28).
Construct validity was classified as high, moderate, or poor if < 25%, 25–50%, or > 50% of hypotheses were rejected, respectively. A sample size of ≥ 70 (item-to-participant ratio of 1:10) was considered necessary (29).
Known-groups validity
Known-groups validity was assessed by comparing mean RECAP scores across established severity bandings for EASI (25, 26), IGA (27), PtGA of AD control (21), POEM (22), and DLQI (23), with the hypothesis that higher severity bandings would correspond to higher RECAP scores.
Reliability
Test–retest reliability was assessed among unchanged patients (based on the GRC scale) between T0 and T1 using the intraclass correlation coefficient (ICCagreement) with a two-way mixed-effects model for absolute agreement(30). An acceptable reliability was defined as ICCagreement > 0.70. Standard error of measurement (SEMagreement) was also reported within this group. A sample size of ≥ 50 unchanged patients was deemed adequate, according to COSMIN guidelines (17).
Interpretability
Single-score cutoffs were estimated using PtGA of AD control as an anchor. Various cutoffs were explored based on RECAP scores corresponding to one-step increases in mean, median, and/or mode on the PtGA of AD control. The optimal banding was selected based on the highest linear weighted kappa agreement with PtGA of AD. Sensitivity analyses assessed whether patients within and outside the proposed banding differed by age or sex.
Change scores included the smallest detectable change (SDC) and minimally important change (MIC) values. SDC was calculated among unchanged patients at T1: SDC = 1.96 × √2 × SEMagreement. Next, MIC values for improvement were estimated using 2 methods: predictive modelling (MICpredict) (31) and receiver operating characteristics (ROC) (MICROC) (30), using the GRC scale at T2 to classify patients as “importantly improved” or “no important change”. Briefly, MICpredict was determined using binary logistic regression: MICpredict = [ln (oddspre)-C]/Bx, where the oddspre was calculated using the prevalence of importantly improved patients divided by 1 minus the prevalence; C represents the intercept and Bx represents the regression coefficient. Given a prevalence of importantly improved patients of 79.0% in our study population, not equal to 50%, the MICpredict value was adjusted accordingly (32). MICROC was identified as the point closest to the upper-left corner of the ROC curve. Notably, MIC values for deterioration were not calculated due to the small number of patients who reported important deterioration (n = 5). A sample size of at least 100 patients, including ≥ 50 with important improvement, was seen as adequate.
Floor and ceiling effects
Floor or ceiling effects were deemed present if > 15% of participants achieved the lowest or highest possible RECAP scores (33).
RESULTS
Patient characteristics
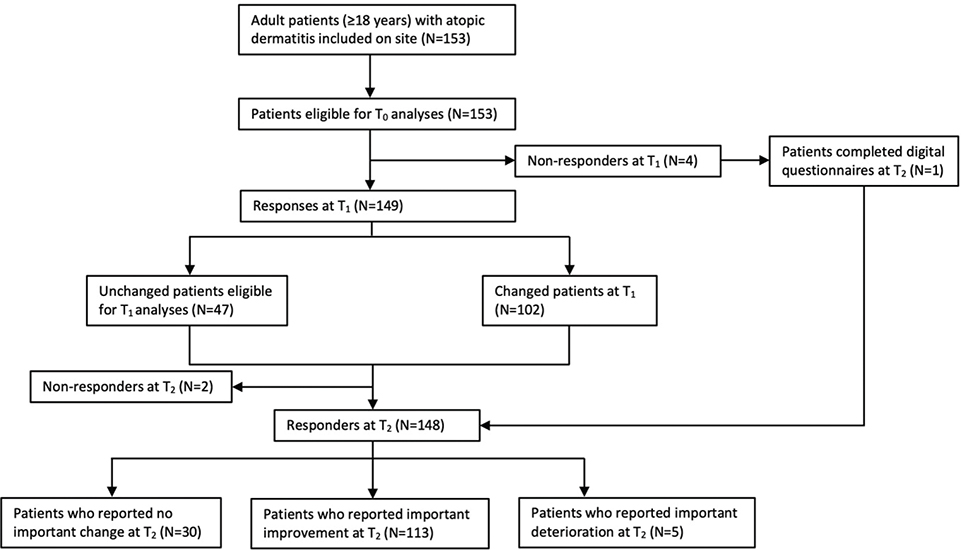
A total of 153 adult patients were included at T0, with a mean age of 28.4 years, of whom 51.0% were male. Patient characteristics are presented in Table I. Based on the EASI and IGA scores, approximately half of the study population had moderate-to-severe disease. Of the 153 adults recruited at T0, 149 completed the T1 questionnaire, and 148 completed the T2 questionnaire. Fig. 1 presents the study flow diagram.
Single-score and change-score validity
For single-score validity, 57.1% of our a priori hypotheses were confirmed, indicating moderate convergent validity of the Chinese version of RECAP (Table II). The correlations that were rejected were lower than initially hypothesized. In total, 71.4% of the hypotheses for change-score validity were confirmed, suggesting moderate responsiveness (Table III).
Known-groups validity
Patients with greater AD severity, as assessed by EASI, IGA, and POEM, as well as those reporting higher daily life impairment on DLQI, had higher mean RECAP scores (Table SII). These findings supported the discriminative validity of RECAP.
Reliability
Reliability was assessed in 47 patients who remained unchanged between T0 and T1. The SEMagreement was 1.99 points. The ICCagreement was 0.96 (95% confidence interval [CI] 0.92–0.98), indicating excellent reliability.
Interpretability
Single scores. The relationship between PtGA of AD control and RECAP is presented in Fig. SI. The correlation between PtGA of AD control and RECAP was –0.53, exceeding the recommended threshold of > 0.4, supporting the appropriateness of using PtGA of AD control as an anchor (34, 35).
For RECAP, 41 banding options were tested (Tables SIII, SIV). The banding option with the highest kappa value (k = 0.447) was proposed for the final banding (completely controlled: 0–2; mostly controlled: 3–10; moderately controlled: 11–12; a little controlled: 13–18; not at all controlled: 19–28). After categorizing patients who reported moderately, a little, and not at all controlled AD into 1 group, a binary cutoff of ≥ 11 was determined to identify those with inadequately controlled AD. In the study population, 5 patients (3.3%) had a PtGA of AD control score > 2 points beyond the proposed banding, while 9 patients (5.9%) scored 2 points higher and 12 (7.9%) scored lower than the proposed banding (Table SV). No significant differences were observed in age (p = 0.13) or sex (p = 0.94) between those falling within and outside the proposed banding.
Change scores
Based on the same unchanged patient group used for reliability analyses, the SDC was 5.5 points.
The correlation of change scores on RECAP with the GRC scale was 0.58, exceeding the minimally recommended threshold of 0.3 (preferably > 0.5) for MIC estimation (36, 37). This confirms the GRC scale as an appropriate anchor. The MIC values for RECAP, obtained using 2 different methods, were: 3.5 for the ROC (Table SVI), and 0.6 for the predictive modelling after adjustment (unadjusted MIC = 1.0).
Floor and ceiling effects
No floor or ceiling effects were observed.
DISCUSSION
In this study, we evaluated the validity, reliability, and interpretability of the Chinese version of RECAP. We found that RECAP exhibited moderate validity for both single and change scores, strong known-groups validity, and excellent reliability. For single-score interpretability, bands for the RECAP scores were determined (completely controlled: 0–2; mostly controlled: 3–10; moderately controlled: 11–12; a little controlled: 13–18; not at all controlled: 19–28), with a binary cutoff of ≥ 11 for identifying adults with inadequate eczema control. For change-score interpretability, an improvement of ≥ 6 points was identified as clinically significant.
Overall, our results support the Chinese version of RECAP as a valid and reliable tool for assessing eczema control, aligning with findings from previous validations in other languages (5, 8–13). As a PROM designed to capture multiple aspects of the patient experience, RECAP demonstrated moderate-to-high correlations with other AD-specific PROMs, such as POEM and NRS peak itch, as well as with skin-related QoL measures like the DLQI. However, compared with previous studies (8, 9, 12, 38), our study revealed lower correlations of RECAP with DLQI, NRS peak itch, and PtGA of AD control. Specifically, the correlation of RECAP with DLQI (0.58 vs 0.89), NRS peak itch (0.62 vs 0.89), and PtGA of AD control (–0.53 vs –0.82) was lower than those reported in a Dutch validation study (12) using the same methodology. Several factors may contribute to these differences. Cultural variations could influence how individuals perceive and report eczema control, as patients’ responses are shaped by social norms and values that differ across countries (15, 16). Chinese patients may place greater emphasis on AD-specific symptoms and signs when considering their disease control, while QoL impacts may be perceived as less central to their condition. This suggests that adapting RECAP’s content to better reflect culturally relevant aspects of eczema control for Chinese patients might enhance its performance. Moreover, a single-item measure such as the PtGA of AD control may not fully capture the complexity of their disease experience. Notably, a similar trend was observed for ADCT in our study (Table SVII), another recommended PROM for measuring eczema control, where its correlations with DLQI, NRS peak itch, and PtGA of AD control were also lower than those reported in previous validations (21, 39). These results underscore the importance of incorporating culturally diverse populations when developing and validating PROMs, particularly for instruments intended for use in international, multicentre studies. Further cross-cultural validation studies could provide deeper insights into the performance of RECAP across different language settings.
A binary threshold of RECAP total scores ≥ 11 was identified as the optimal cutoff for distinguishing Chinese patients with inadequately controlled AD. Interestingly, this cutoff is substantially higher than the cutoff of ≥ 6 reported in the Dutch validation study (12), which used the same methodology. The Dutch bandings (0–1, 2–5, 6–11, 12–19, 20–28) (12) yielded a kappa value of 0.292 in our study population, much lower than the highest kappa value of 0.447 for the proposed bandings in our study. This indicates that the Dutch bandings are not appropriate for Chinese patients. Such discrepancies may be due to cultural differences, where Chinese patients might have higher tolerance towards their disease and perceive more severe conditions as acceptable compared with Western populations (15, 16). In the context of a treat-to-target strategy for AD treatment (40), applying a universal cutoff without cultural adaptation may result in overtreatment or undertreatment across different settings. As yet, our study and the Dutch study are the only ones that have examined the interpretability of RECAP single scores, highlighting the need for further research in diverse populations. Moreover, applying our proposed bandings, only approximately one-third of Chinese patients had well-controlled AD, indicating a need for more advanced treatments in China. It is important to note that while the HOME initiative has recommended RECAP or ADCT for assessing eczema control in clinical practice and trials, no studies have evaluated AD control in Chinese patients using RECAP. Our findings provide valuable data that may facilitate the use of RECAP in routine clinical practice and clinical trials in China, further enabling comparisons between Chinese and international patient populations.
For change-score interpretability, an improvement of ≥ 6 points in RECAP should be considered a real and clinically meaningful change. We used 2 anchor-based methods, as endorsed by COSMIN, to estimate the MIC values, but observed a notable discrepancy between them (MICROC 3.5 vs. unadjusted MICpredict 1.0). However, it is important to note that the sum of the misclassification percentage used to determine the optimal MICROC cutoff was closer to those for cutoff values of 1.5 and 0.5 (differences of 0.007 and 0.008, respectively), both of which were closer to the unadjusted MICpredict. Additionally, given that 78.7% of our study population showed improvement, this may have introduced a bias towards a higher MIC than the “genuine” MIC (32), A correction formula has been proposed for MICpredict to account for this bias, but no similar correction exists for MICROC. Thus, we assumed that the adjusted MICpredict provides the best estimate of the true MIC. Beyond clinical significance, a change in RECAP should also exceed the measurement error to be considered reliable. In our study, the SDC was 5.5 points, larger than the adjusted MICpredict (0.6). Ideally, the SDC should be smaller than the MIC to minimize measurement-related uncertainty (41), The relatively large SDC in our study may stem from several causes, including variability in patient responses, cultural influences on self-reporting, and recall bias. Despite this, an improvement of ≥ 6 points can be interpreted as a real and meaningful change in clinical practice and research.
A main strength of this study is its adherence to the COSMIN guidelines, high follow-up rates at T1 and T2, and inclusion of patients with varying disease severities. However, several limitations should be noted. First, MIC values for deterioration could not been estimated due to the small sample size. Additionally, the single-centre study of Chinese adults limits result generalizability, necessitating confirmation in diverse Chinese populations and validation in paediatric and other linguistic groups in the future. Also, cultural differences within language groups (e.g., urban vs rural areas, level of education, socioeconomic status) may influence RECAP response through health literacy; however, the lack of such data in this study limits their evaluation. The absence of prior content validity assessment for the Chinese RECAP may affect our results. Lastly, the anchors used in this study – PtGA of AD control and the GRC scale – have not been formally validated, as no validated instruments specifically designed for these constructs currently exist.
To conclude, the Chinese version of RECAP demonstrates moderate validity for both single and change scores, strong known-groups validity, and excellent test–retest reliability. We propose final bandings for RECAP single scores and identify a binary cutoff of ≥ 11 points for detecting uncontrolled AD in Chinese adult patients. Additionally, an improvement of ≥ 6 points in RECAP is considered a real and clinically meaningful change. These findings indicate the influence of cultural factors on individuals’ perceptions and reporting of eczema control. With the newly established population-specific thresholds, the validated Chinese RECAP could serve as a robust tool for evaluating eczema control in both clinical practice and research settings.
ACKNOWLEDGEMENTS
The authors gratefully thank all the patients for their participation.
Data availability: The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics statement: This research was reviewed and approved by the Medical Ethical Review Board of the Dermatology Hospital, Southern Medical University (reference: 2024027).
Patient consent on file: All patients provided digital informed consent.
REFERENCES
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet 2020; 396: 345–360. https://doi.org/10.1016/S0140-6736(20)31286-1
- Mao D, Li J, Liu S, Liu P, Tian J, Liu X, et al. Prevalence and risk factors of atopic dermatitis in Chinese adults: a nationwide population-based cross-sectional study. Chin Med J (Engl) 2023; 136: 604–606. https://doi.org/10.1097/CM9.0000000000002560
- Schmitt J, Spuls P, Boers M, Thomas K, Chalmers J, Roekevisch E, et al. Towards global consensus on outcome measures for atopic eczema research: results of the HOME II meeting. Allergy 2012; 67: 1111–1117. https://doi.org/10.1111/j.1398-9995.2012.02874.x
- Barbarot S, Rogers NK, Abuabara K, Aubert H, Chalmers J, Flohr C, et al. Strategies used for measuring long-term control in atopic dermatitis trials: a systematic review. J Am Acad Dermatol 2016; 75: 1038–1044. https://doi.org/10.1016/j.jaad.2016.05.043
- Howells LM, Chalmers JR, Gran S, Ahmed A, Apfelbacher C, Burton T, et al. Development and initial testing of a new instrument to measure the experience of eczema control in adults and children: Recap of Atopic Eczema (RECAP). Br J Dermatol 2020; 183: 524–536. https://doi.org/10.1111/bjd.18780
- Leshem YA, Chalmers JR, Apfelbacher C, Katoh N, Gerbens LAA, Schmitt J, et al. Measuring atopic eczema control and itch intensity in clinical practice: a consensus statement from the Harmonising Outcome Measures for Eczema in Clinical Practice (HOME-CP) Initiative. JAMA Dermatol 2022; 158: 1429–1435. https://doi.org/10.1001/jamadermatol.2022.4211
- Williams HC, Schmitt J, Thomas KS, Spuls PI, Simpson EL, Apfelbacher CJ, et al. The HOME Core outcome set for clinical trials of atopic dermatitis. J Allergy Clin Immunol 2022; 149: 1899–1911. https://doi.org/10.1016/j.jaci.2022.03.017
- Bhanot A, Peters TJ, Ridd MJ. Assessing the validity, responsiveness and reliability of the Recap measure of eczema control. Br J Dermatol 2021; 184: 955–957. https://doi.org/10.1111/bjd.19709
- Yew YW, Phuan CZY, Zhao X, Howells L, Apfelbacher CJ. Validation of the Recap of Atopic Eczema (RECAP) measurement instrument for eczema control in adult patients in an Asian clinical setting. Acta Derm Venereol 2024; 104: adv32323. https://doi.org/10.2340/actadv.v104.32323
- Gabes M, Ragamin A, Baker A, Kann G, Donhauser T, Gabes D, et al. Content validity of the Recap of atopic eczema (RECAP) instrument in Dutch, English and German to measure eczema control in young people with atopic eczema: a cognitive interview study. Br J Dermatol 2022; 187: 919–926. https://doi.org/10.1111/bjd.21767
- Ragamin A, Zhang J, Pasmans SGMA, Schappin R, Romeijn GLE, van Reusel MA, et al. The construct validity, responsiveness, reliability and interpretability of the Recap of Atopic Eczema questionnaire (RECAP) in children. Br J Dermatol 2024; 190: 867–875. https://doi.org/10.1093/bjd/ljae017
- Zhang J, Ragamin A, Romeijn GLE, Loman L, Oosterhaven JAF, Schuttelaar MLA. Validity, reliability, responsiveness and interpretability of the Recap of Atopic Eczema (RECAP) questionnaire. Br J Dermatol 2023; 189: 578–587. https://doi.org/10.1093/bjd/ljad247
- Sigurdardottir G, Alsterholm M, Andersson CD, Bradley M, Sandström Falk M, Johansson EK, et al. Cross-cultural validation of the RECAP of Atopic Eczema Questionnaire in a Swedish population. Acta Derm Venereol 2024; 104: adv38889. https://doi.org/10.2340/actadv.v104.38889
- Baker A, Stuart B, Howells L, Mitchell EJ, Thomas KS. Determining the minimal important change of the Recap of Atopic Eczema (RECAP) instrument in clinical trials. Skin Health Dis 2024; 4: e470. https://doi.org/10.1002/ski2.470
- Fischer MJ, Inoue K, Matsuda A, Kroep JR, Nagai S, Tozuka K, et al. Cross-cultural comparison of breast cancer patients’ quality of life in the Netherlands and Japan. Breast Cancer Res Treat 2017; 166: 459–471. https://doi.org/10.1007/s10549-017-4417-z
- Lima XT. Cumulative life course impairment across cultures and medical systems. Curr Probl Dermatol 2013; 44: 137–144. https://doi.org/10.1159/000350178
- Mokkink LB, Prinsen CA, Patrick DL, et al. COSMIN study design checklist for patient-reported outcome measurement instruments. 2019
- de Vet HC, Terwee CB, Mokkink L et al. Measurement in medicine: a practical guide. Cambridge: Cambridge University Press, 2011.
- University of Nottingham. Recap of Atopic Eczema (RECAP): an outcome measurement instrument to capture ‘eczema control’ [accessed 25 May 2025]. Available from: https://www.nottingham.ac.uk/research/groups/cebd/resources/recap.aspx#:~:text = RECAP%20is%20a%20seven%2Ditem,reported%20version%20for%20younger%20children
- Williams HC, Burney PG, Pembroke AC, Hay RJ. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol 1994; 131: 406–416. https://doi.org/10.1111/j.1365-2133.1994.tb08532.x
- Pariser DM, Simpson EL, Gadkari A, Bieber T, Margolis DJ, Brown M, et al. Evaluating patient-perceived control of atopic dermatitis: design, validation, and scoring of the Atopic Dermatitis Control Tool (ADCT). Curr Med Res Opin 2020; 36: 367–376. https://doi.org/10.1080/03007995.2019.1699516
- Charman CR, Venn AJ, Ravenscroft JC, Williams HC. Translating Patient-Oriented Eczema Measure (POEM) scores into clinical practice by suggesting severity strata derived using anchor-based methods. Br J Dermatol 2013; 169: 1326–1332. https://doi.org/10.1111/bjd.12590
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- Yosipovitch G, Reaney M, Mastey V, Eckert L, Abbé A, Nelson L, et al. Peak Pruritus Numerical Rating Scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol 2019; 181: 761–769. https://doi.org/10.1111/bjd.17744
- Chopra R, Vakharia PP, Sacotte R, Patel N, Immaneni S, White T, et al. Severity strata for Eczema Area and Severity Index (EASI), modified EASI, Scoring Atopic Dermatitis (SCORAD), objective SCORAD, Atopic Dermatitis Severity Index and body surface area in adolescents and adults with atopic dermatitis. Br J Dermatol 2017; 177: 1316–1321. https://doi.org/10.1111/bjd.15641
- Hanifin JM, Thurston M, Omoto M, Cherill R, Tofte SJ, Graeber M. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol 2001; 10: 11–18. https://doi.org/10.1034/j.1600-0625.2001.100102.x
- Simpson E, Bissonnette R, Eichenfield LF, Guttman-Yassky E, King B, Silverberg JI, et al. The Validated Investigator Global Assessment for Atopic Dermatitis (vIGA-AD): the development and reliability testing of a novel clinical outcome measurement instrument for the severity of atopic dermatitis. J Am Acad Dermatol 2020; 83: 839–846. https://doi.org/10.1016/j.jaad.2020.04.104
- Prinsen C a C, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet HCW, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res Int J Qual Life Asp Treat Care Rehabil 2018; 27: 1147–1157. https://doi.org/10.1007/s11136-018-1798-3
- Anthoine E, Moret L, Regnault A, Sébille V, Hardouin J-B. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual Life Outcomes 2014; 12: 176. https://doi.org/10.1186/s12955-014-0176-2
- de Vet HCW, Terwee CB, Knol DL, Bouter LM. When to use agreement versus reliability measures. J Clin Epidemiol 2006; 59: 1033–1039. https://doi.org/10.1016/j.jclinepi.2005.10.015
- Terluin B, Eekhout I, Terwee CB, de Vet HCW. Minimal important change (MIC) based on a predictive modeling approach was more precise than MIC based on ROC analysis. J Clin Epidemiol 2015; 68: 1388–1396. https://doi.org/10.1016/j.jclinepi.2015.03.015
- Terluin B, Eekhout I, Terwee CB. The anchor-based minimal important change, based on receiver operating characteristic analysis or predictive modeling, may need to be adjusted for the proportion of improved patients. J Clin Epidemiol 2017; 83: 90–100. https://doi.org/10.1016/j.jclinepi.2016.12.015
- McHorney CA, Tarlov AR. Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res 1995; 4: 293–307. https://doi.org/10.1007/BF01593882
- Norman GR, Sridhar FG, Guyatt GH, Walter SD. Relation of distribution- and anchor-based approaches in interpretation of changes in health-related quality of life. Med Care 2001; 39: 1039–1047. https://doi.org/10.1097/00005650-200110000-00002
- Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med 1993; 118: 622–629. https://doi.org/10.7326/0003-4819-118-8-199304150-00009
- Cella D, Hahn EA, Dineen K. Meaningful change in cancer-specific quality of life scores: differences between improvement and worsening. Qual Life Res 2002; 11: 207–221. https://doi.org/10.1023/a:1015276414526
- Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol 2008; 61: 102–109. https://doi.org/10.1016/j.jclinepi.2007.03.012
- Onteniente-Gomis MM, Ortiz-Romero PL, Tous Romero F, Salamanca Castro AB, Ortiz de Frutos FJ. Spanish version of the RECAP questionnaire to assess control of atopic eczema: translation, cultural adaptation, validation, and correlations with other patient-reported outcome measures. Actas Dermosifiliogr 2023; 114: 488–493. https://doi.org/10.1016/j.ad.2023.02.018
- Zhang J, Miltner L, Loman L, Ragamin A, Oosterhaven JAF, Schuttelaar MLA. Validation of the Atopic Dermatitis Control Tool (ADCT) and a comparison with the Recap of Atopic Eczema Questionnaire (RECAP). Acta Derm Venereol 2025; 105: adv42364. https://doi.org/10.2340/actadv.v105.42364
- Vestergaard C, Skovsgaard C, Johansen C, Deleuran M, Thyssen JP. Treat-to-target in atopic dermatitis. Am J Clin Dermatol 2024; 25: 91–98. https://doi.org/10.1007/s40257-023-00827-y
- van Kampen DA, Willems WJ, van Beers LWAH, Castelein RM, Scholtes VAB, Terwee CB. Determination and comparison of the smallest detectable change (SDC) and the minimal important change (MIC) of four-shoulder patient-reported outcome measures (PROMs). J Orthop Surg 2013; 8: 40. https://doi.org/10.1186/1749-799X-8-40