SHORT COMMUNICATION
Skin Rash on Immunotherapy: When Trombicula Mimics a Cutaneous Immune-related Adverse Event
Léa FRIGOUT1#, Taha TAGMOUTI1#, Pierre GOINEAU2, Anne DOMPMARTIN1,3 and Jean Matthieu L’Orphelin1,3 
1Department of Dermatology, Caen – Normandy University Hospital, Avenue de la Côte de Nacre - 14033 Caen, France, 2Department of Anatomical Pathology, Caen – Normandy University Hospital, Caen, and 3Caen University, Caen. E-mail: frigoutlea243@gmail.com
#These authors contributed equally.
Citation: Acta Derm Venereol 2025; 105: adv43467. DOI: https://doi.org/10.2340/actadv.v105.43467.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 26, 2025. Accepted after revision: May 22, 2025. Published: Jul 8, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Skin rashes occurring in the context of immunotherapy treatment are often immune-mediated (1). However, it is important not to overlook a parasitic infestation that may occur simultaneously with the treatment cycle. Trombiculiasis is a common parasitic infestation that causes local itching and irritation due to the larvae of a mite (chigger) (2). Although there are many species of parasitic mites in a variety of habitats worldwide, the species most commonly referred to as chiggers include Eutrombicula alfreddugesi in the south of the United States, Neotrombicula autumnalis in Europe, and the Leptotrombidium genus in the Asia-Pacific (2). Thus, Neotrombicula autumnalis has been reported as the most frequent causative agent of human trombiculiasis in Europe, but Kepkatrombicula desaleri, Blankaartia acuscutellaris, Trombicula toldti, and Neotrombicula inopinata have also been described (3). The reaction is usually mild and self-limiting, but the bites may transmit infections depending on the geographical area or lead to bacterial superinfection. Indeed, chiggers are known vectors of scrub typhus in humans, which is caused by the bacteria Orientia tsutsugamushi (2) and can be fatal (4). Adults live on the soil, but the 6-legged larvae, which have a characteristic orange colour, feed on warm-blooded vertebrates (5). In late summer and autumn in the Northern Hemisphere, they are found outdoors and bite at sites of constriction of clothing (2) and skin folds. We report a case of trombiculiasis in a patient with advanced melanoma on therapy with immune checkpoint inhibitors (ICI) mimicking a cutaneous immune-mediated event.
CASE REPORT
A 47-year-old woman with metastatic melanoma involving the lungs and lymph nodes with a complete response presented for her 8th nivolumab cycle. She presented with a pruritic rash that had been evolving for 1 week. She had a past medical history of autoimmune diseases: Crohn’s disease, ankylosing spondylitis, psoriasis, eosinophilic gastritis, immune-induced hypophysitis complicated by thyrotropin and corticotropin deficiency. Her medications included morphine, gabapentin, apixaban, esomeprazole, and metoclopramide.
The rash reportedly began on the abdomen and arms before spreading to the legs. There was no history of recent travel, close contacts presenting with pruritus, changes in lifestyle, or bed bugs found at home. She gardens and enjoys balneotherapy sessions. Biological workup was normal except for an undetectable cortisol level.
Clinical examination revealed pruritic, erythematous papules surrounded by a white halo on both popliteal fossae, abdomen, legs, and arms (Fig. 1A, B). The face and mucous membranes were spared. The diagnoses considered were urticaria, vasculitis, insect bites, or immune-related eruption.
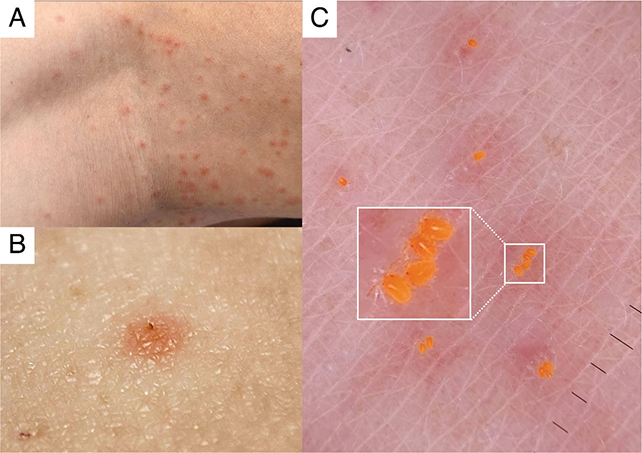
Fig. 1. (A) Clinical appearance of skin lesions in the popliteal fossa (Dr Tagmouti photo collection). (B) Macroscopic photograph of an isolated clinical lesion at the centre of which the body of the parasite can be seen (Dr Tagmouti photo collection). (C) Dermoscopic appearance of Neotrombicula autumnalis larvae with their 6 legs and characteristic orange colour (Dr Tagmouti photo collection).
Dermoscopic examination revealed orange lesions in the centre of some of the papules, which, with electronic zoom, appeared to be orange mites 0.2 mm in length (Fig. 1C), narrowing the differential diagnosis of Trombicula, Dermanyssus, or Ornythonyssus bites. Parasitological and histological examination confirmed the diagnosis of trombiculiasis (Fig. 2). Histology revealed the 0.23 mm parasite on the surface of the sample, and within the superficial dermis an abundant perivascular and interstitial inflammatory infiltrate composed of lymphocytes, histiocytes, and a few neutrophils and eosinophils. The epidermis showed lymphocytic exocytosis, the basal layer was slightly vacuolated, there was no keratinocyte necrosis, and the keratin layer was orthokeratotic. The hypodermis was normal. The findings were compatible with an insect bite.
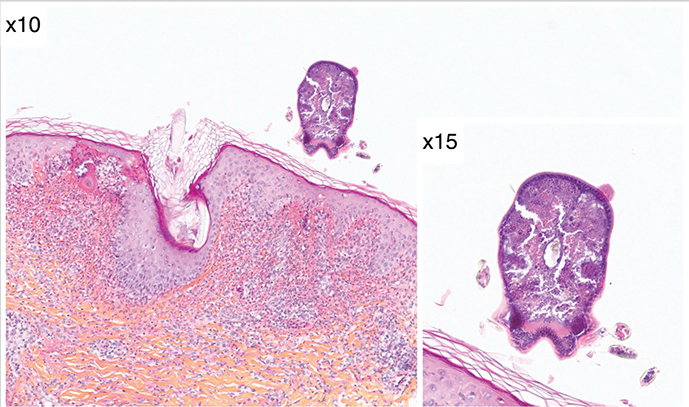
Fig. 2. Histological image of a Neotrombicula autumnalis larva. Haematoxylin-eosin-saffron staining (HES), x10 and x15. (P. Goineau photo collection).
The patient, who was experiencing this infestation for the first time in her life, was treated with antihistamines and topical corticosteroids, which led to a regression of the pruritus within a few days.
DISCUSSION
Cases of trombiculiasis are rarely reported in the literature (6) as they are rarely visualized on clinical and/or histological examination. The diagnosis is initially suspected from the history of the pruritic lesions. Indeed, cutaneous findings are nonspecific (7). The host’s reaction is largely caused by sensitization to the saliva injected by Trombicula, ranging from a slightly irritable erythema to papules or papulovesicles matched with intense itch (6). In some rare cases, patients may react with regional adenitis (6), urticarial, bullous, or morbilliform eruptions (8). The management of chigger bites is supportive, focused on symptom control with oral antihistamines or topical corticosteroid creams to reduce itching (2). Washing exposed clothes at 55°C minimum (6) or treating with insecticides to kill the larvae is also important (2). However, prevention is key: avoid areas of chigger infestation, cover the skin completely if exposure is unavoidable, and use N,N-diethyl-3-methylbenzamide repellent and permethrin (2).
The naked eye rarely visualizes the parasite and dermoscopic examination is an important aid to see the pathognomonic orange parasite. The usefulness of dermoscopy in the diagnosis of many parasitic skin disorders has led to the introduction of the concept of “entodermoscopy” (7). In our case, we were able to confirm the diagnosis through dermoscopy, serial histological sections, and parasitological examination. It was difficult to differentiate, based solely on clinical presentation, urticaria regardless of its origin, from a reaction to chigger bites: pruritic erythematous papules surrounded by a white halo are characteristic and very commonly found in urticaria. Moreover, given the context of treatment with ICI, an immune-induced urticaria could reasonably be considered. However, the fixed and non-migratory nature of the lesions and their location, particularly their large number in the popliteal fossae, could lead to questioning of this diagnosis and consideration of ectoparasite bites.
Pruritic lesions in a patient treated with nivolumab with a past history of autoimmune diseases could have been misdiagnosed as an immune-mediated rash (1), leading to the discontinuation of treatment. A thorough dermatologic evaluation including a dermoscopic examination therefore seems mandatory and justifies the continued involvement of the dermatologist in the oncologic care pathway of patients undergoing ICI, in a context where rapid labelling of an immune-mediated skin rash tends to be easy, albeit inappropriate.
ACKNOWLEDGEMENT
Informed consent: The authors obtained written consent from patients for their photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.
REFERENCES
- L’Orphelin JM, Cassecuel J, Kandolf L, Harwood CA, Tookey P, Junejo MH, et al. Cutaneous manifestations induced by check point inhibitors in 120 melanoma patients: the European MelSkinTox Study. J Eur Acad Dermatol Venereol 2023; 37: 1606–1615. https://doi.org/10.1111/jdv.19112
- Alexander L, Chen RJ, Buckley CJ. Chigger bites and trombiculiasis. In: StatPearls. Orlando, FL: StatPearls Publishing; 2024.
- Stekolnikov AA, Santibáñez P, Palomar AM, Oteo JA. Neotrombicula inopinata (Acari: Trombiculidae): a possible causative agent of trombiculiasis in Europe. Parasites Vectors 2014; 7: 90. https://doi.org/10.1186/1756-3305-7-90
- Saraswati K, Baird JK, Blacksell SD, Grijsen ML, Day NPJ. History of scrub typhus in Indonesia. Trans R Soc Trop Med Hyg 2025; 119: 338–345. https://doi.org/10.1093/trstmh/traf017
- Ramondetta A, Ribero S, Peano A, Quaglino P, Broganelli P. In vivo observation of trombiculosis with fluorescence-advanced videodermatoscopy. Emerg Infect Dis 2020; 26: 1904–1905. https://doi.org/10.3201/eid2608.200077
- Di Meo N, Fadel M, Trevisan G. Pushing the edge of dermoscopy in new directions: entomodermoscopy of Trombicula autumnalis. Acta Dermatovenerol Alp Pannonica Adriat 2017; 26: 45–46. https://doi.org/10.15570/actaapa.2017.14
- Nasca MR, Lacarrubba F, Micali G. Diagnosis of trombiculosis by videodermatoscopy. Emerg Infect Dis 2014; 20: 1059–1060. https://doi.org/10.3201/eid2006.130767
- Jones JG. Chiggers. Am Fam Physician 1987; 36: 149–152. https://pubmed.ncbi.nlm.nih.gov/3618452/