ORIGINAL REPORT
New-onset Autoimmune Diseases in Patients with Prurigo Nodularis: A Global-federated Retrospective Cohort Study
Hui-Chin CHANG1-3, Chia-Chi CHANG3, Yen-Ju CHU3, Wei-Ting HSU3, Yun-Feng LI3, Yi-Sheng JHANG4, Yu-Jung SU5, Shiu-Jau CHEN6,7#, Torsten ZUBERBIER8,9 and Shuo-Yan GAU1,5,8,10#
1Evidence-based Medicine Center, Chung Shan Medical University Hospital, Taichung, 2Library, Chung Shan Medical University Hospital, Taichung, 3School of Medicine, Chung Shan Medical University, Taichung, 4Department of Pharmacy, Chung Shan Medical University Hospital, Taichung, 5Orthopedics Department, Chi-Mei Medical Center, Tainan, 6Department of Neurosurgery, Mackay Memorial Hospital, Taipei, 7Department of Medicine, Mackay Medical College, New Taipei City, Taiwan, 8Institute of Allergology, Charité–Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, 9Fraunhofer Institute for Translational Medicine and Pharmacology, Immunology and Allergology, Berlin, Germany, and 10Department and Graduate Institute of Business Administration, National Taiwan University, Taipei, Taiwan
#These authors contributed equally and share the corresponding authorship equally.
Prurigo nodularis (PN) has been associated with autoimmune diseases, though longitudinal data are limited. This study investigates the risk of autoimmune disease development in PN patients using a global electronic health record database. This retrospective cohort study analysed data from the Global Collaborative Network within the TriNetX research network. Adults (≥ 18 years) with PN were compared with propensity score-matched controls without PN. Matching considered age, sex, comorbidities, race, and socioeconomic status. Patients with prior autoimmune diseases or cancers were excluded. Incident autoimmune diseases, including systemic lupus erythematosus (SLE), Sjögren’s syndrome, psoriasis, ankylosing spondylitis (AS), rheumatoid arthritis (RA), Crohn’s disease (CD), and ulcerative colitis (UC), were evaluated using hazard ratios (HR). Among 17,963 PN patients and the same amount of matched pairs, PN patients had higher risks for SLE (HR: 2.16, 95% CI: 1.44–3.24), Sjögren’s syndrome (HR: 1.86, 95% CI: 1.33–2.59), and psoriasis (HR: 3.20, 95% CI: 2.58–3.97). Stratified analysis revealed that female PN patients had higher risks for SLE and Sjögren’s syndrome, while psoriasis risk was elevated in both sexes, especially in males. Risks for AS, RA, CD, and UC were not significant. Sensitivity analyses validated these findings. In conclusion, PN is linked to increased risks for SLE, Sjögren’s syndrome, and psoriasis, highlighting the need for proactive screening and management of autoimmune diseases in PN patients.
SIGNIFICANCE
This study highlights that people with prurigo nodularis, a chronic, itchy skin condition, are more likely to develop autoimmune diseases like psoriasis, lupus, and Sjögren’s syndrome. By analysing real-world data from a large, diverse group of patients, our findings reveal important links that could improve early detection and care for those at risk. Understanding these associations not only helps doctors treat prurigo nodularis more effectively but also supports better long-term health planning. Ultimately, this research may guide future treatments and lead to better quality of life for people living with prurigo nodularis and related immune conditions.
Key words: prurigo nodularis; autoimmune diseases; psoriasis; cohort; epidemiology; electronic medical records.
Citation: Acta Derm Venereol 2025; 105: adv43515. DOI: https://doi.org/10.2340/actadv.v105.43515.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 1, 2025. Accepted after revision: Aug 14, 2025. Published: Sep 4, 2025.
Corr: Shuo-Yan Gau, MD, FRSPH, Department and Graduate Institute of Business Administration, National Taiwan University, No. 1, Sec. 4, Roosevelt Rd., Taipei 106319, Taiwan. E-mail: r13741020@ntu.edu.tw
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Prurigo nodularis (PN) is a chronic skin condition characterized by intensely itchy, thickened nodules and persistent inflammation (1). Current treatment options for PN-related pruritus include systemic immunomodulatory therapies such as corticosteroids, cyclosporine, methotrexate, and, more recently, biologics like dupilumab and nemolizumab, which target key cytokines involved in PN pathogenesis (2–5). The pathogenesis of PN is not yet fully understood, though the chronic itch–scratch cycle is believed to play a pivotal role, leading to immune and neural dysregulation.
PN is associated with various comorbidities, particularly autoimmune diseases. A US study reported significantly higher risks for conditions like thyroid disease, irritable bowel diseases, type 1 diabetes, coeliac disease, and psoriasis (ORs 1.39–4.82) (6). A cross-sectional Korean study further revealed sex-specific patterns, with females more likely to have hypothyroidism and Crohn’s disease, and males showing higher odds of rheumatoid arthritis (RA), hyperthyroidism, systemic lupus erythematosus (SLE), and autoimmune thyroiditis (ORs 0.55–4.20) (7).
Despite these reports, current research on the association between PN and autoimmune diseases is limited by small scale and cross-sectional study design. To address these gaps, we conducted this large-scale study aiming to assess the risk of new-onset autoimmune diseases in a longitudinal cohort design.
MATERIALS AND METHODS
This multicentre, retrospective cohort study utilized data from the TriNetX research network, a global database of electronic health records that is updated prospectively. In the TriNetX research network, collaborative institutions span regions including the United States, Latin America, Europe, and the Asia-Pacific. The TriNetX platform includes de-identified medical records from partnered healthcare organizations, providing a robust resource for epidemiological research (8–10). The Global Collaborative Network, a subset of TriNetX, was used in this study. In the supplementary files, Table SI depicts the specific coding algorithm in detail, and Table SII depicts the description of all applied sensitivity analysis models; further information regarding the TriNetX database is stated in Appendix S1.
Patients who had more than 2 visit records between January 2005 and December 2018 and were 18 years or older were enrolled in the current study (Fig. 1). Participants with records of PN diagnosis were identified as the PN cohort, while heathy people without records of prior PN diagnosis were enrolled as the non-PN controls. The application of International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes in defining PN in real-world studies has been validated in previous studies (11). In both cohorts, patients who had been diagnosed for any neoplasms or have a previous record of autoimmune diseases, including ankylosing spondylitis (AS), RA, SLE, Sjögren’s syndrome, psoriasis, Crohn’s disease (CD) and ulcerative colitis (UC) and dermatopolymyositis, or deceased before or on the index date were excluded from the study. For each analysis, propensity score matching was applied, and the baseline characteristic differences between the PN and control cohorts were assessed both prior to and following matching (Table I). In the main analysis, covariates in the matching process included age at index, sex, race, body mass index, status of comorbidities (including diabetes mellitus, hypertension, hyperlipidaemia, cerebrovascular diseases, vitamin D deficiency, chronic kidney disease), status of co-medication use (glucocorticoids, methotrexate, dupilumab, antidepressants), lab data (C-reactive protein), status of smoking, alcoholism and substance use, medical utilization status (ambulatory and acute inpatient visit), and socioeconomic status (problems related to housing and economic circumstances, persons with potential health hazards related to socioeconomic and psychosocial circumstances). Outcome events were set as new-onset autoimmune diseases and disorders, including AS, RA, SLE, Sjögren’s syndrome, psoriasis, CD, and UC. Although the inclusion of psoriasis under the category of autoimmune diseases remains debated (12), we included it as 1 of the study endpoints of interest in this study due to its autoimmune-associated pathogenetic mechanisms identified to date and its clinical relationship with other autoimmune diseases. Incident outcome events occurring prior to 3 months after index date were excluded from further analysis to prevent potential bias. Detailed information on all sensitivity analysis applied is given in Table SII. To minimize potential bias from overmatching, the sensitivity analyses employed several distinct analytical algorithms. To mitigate the risk of reverse causality, models incorporating various wash-out periods were also utilized. Given that specific autoimmune-related diseases such as atopic dermatitis, psoriasis, type 1 diabetes, and thyroid disorders could introduce significant confounding bias to the incident outcomes, we conducted separate analyses excluding these diseases from both PN and non-PN controls to validate the results. To avoid confounding by indication, we have applied different inflammatory skin diseases, including hidradenitis suppurativa (HS), alopecia areata (AA), and rosacea as active comparator to compare the risk of autoimmune diseases with PN patients. Furthermore, stratified analyses were conducted to assess the varying risks of autoimmune diseases across different sex and age subgroups. Age subgroups were defined as 18–64 years and ≥ 65 years, with 65 years reflecting conventional age cutoffs used in epidemiological studies to differentiate between middle-aged and older adults (13, 14).
| Item | Before matching | After matchinga | ||||
| PN cohort (n = 17,973) | Control cohort (n = 44,446,550) | SMD | PN cohort (n = 17,963) | Control cohort (n = 17,963) | SMD | |
| Age at index | ||||||
| Mean ± SD | 45.0 ± 19.3 | 34.7 ± 20.3 | 0.52 | 45.0 ± 19.3 | 45.4 ± 19.6 | 0.02 |
| Sex | ||||||
| Male | 7110 (39.6) | 1921834 (43.2) | 0.07 | 7106 (39.6) | 6722 (37.4) | 0.04 |
| Female | 10446 (58.1) | 2383440 (53.6) | 0.09 | 10440 (58.1) | 10468 (58.3) | 0.00 |
| Unknown sex | 417 (2.3) | 141276 (3.2) | 0.05 | 417 (2.3) | 773 (4.3) | 0.11 |
| Race, n (%) | ||||||
| White | 8252 (45.9) | 2481957 (55.8) | 0.20 | 8250 (45.9) | 8336 (46.4) | 0.01 |
| Black or African American | 3319 (18.5) | 665418 (15.0) | 0.09 | 3314 (18.4) | 3305 (18.4) | 0.00 |
| Asian | 1130 (6.3) | 204144 (4.6) | 0.07 | 1127 (6.3) | 1113 (6.2) | 0.00 |
| American Indian or Alaska Native | 74 (0.4) | 14518 (0.3) | 0.01 | 74 (0.4) | 76 (0.4) | 0.00 |
| Native Hawaiian or other Pacific Islander | 66 (0.4) | 17884 (0.4) | 0.01 | 66 (0.4) | 124 (0.7) | 0.04 |
| Other race | 733 (4.1) | 233244 (5.2) | 0.06 | 733 (4.1) | 1095 (6.1) | 0.09 |
| Unknown race | 4399 (24.5) | 829385 (18.7) | 0.14 | 4399 (24.5) | 3914 (21.8) | 0.06 |
| Socioeconomic status | ||||||
| Persons with potential health hazards related to socioeconomic and psychosocial circumstances | 281 (1.6) | 32394 (0.7) | 0.08 | 280 (1.6) | 215 (1.2) | 0.03 |
| Lifestyle | ||||||
| Mental and behavioural disorders due to psychoactive substance use | 1340 (7.5) | 129951 (2.9) | 0.21 | 1339 (7.5) | 1275 (7.1) | 0.01 |
| Comorbidities | ||||||
| Hypertension | 2928 (16.3) | 348043 (7.8) | 0.26 | 2928 (16.3) | 2869 (16.0) | 0.01 |
| Hyperlipidaemia | 1731 (9.6) | 223639 (5.0) | 0.18 | 1731 (9.6) | 1744 (9.7) | 0.00 |
| Diabetes mellitus | 1601 (8.9) | 149365 (3.4) | 0.23 | 1601 (8.9) | 1540 (8.6) | 0.01 |
| Vitamin D deficiency | 623 (3.5) | 79863 (1.8) | 0.10 | 623 (3.5) | 590 (3.3) | 0.01 |
| Chronic kidney disease (CKD) | 461 (2.6) | 31006 (0.7) | 0.15 | 461 (2.6) | 400 (2.2) | 0.02 |
| Cerebrovascular diseases | 398 (2.2) | 40103 (0.9) | 0.11 | 398 (2.2) | 339 (1.9) | 0.02 |
| Medications | ||||||
| Glucocorticoids | 4511 (25.1) | 401726 (9.0) | 0.44 | 4501 (25.1) | 4488 (25.0) | 0.00 |
| Antidepressants | 2549 (14.2) | 232781 (5.2) | 0.31 | 2543 (14.2) | 2513 (14.0) | 0.00 |
| Methotrexate | 52 (0.3) | 2000 (0.0) | 0.06 | 48 (0.3) | 27 (0.2) | 0.03 |
| Dupilumab | 17 (0.1) | 55 (0.0) | 0.04 | 10 (0.1) | 10 (0.1) | 0.00 |
| Medical utilization status | ||||||
| Ambulatory visit | 11259 (62.6) | 2258806 (50.8) | 0.24 | 11249 (62.6) | 11204 (62.4) | 0.01 |
| Acute inpatient visit | 41 (0.2) | 2222 (0.1) | 0.05 | 41 (0.2) | 33 (0.2) | 0.01 |
| Laboratory data | ||||||
| CRP, n (%) | ||||||
| ≧ 3 (mg/l) | 585 (3.3) | 45658 (1.0) | 0.15 | 585 (3.3) | 515 (2.9) | 0.02 |
| BMI,n (%) | ||||||
| ≧ 25 (kg/m2) | 3857 (21.5) | 594677 (13.4) | 0.21 | 3856 (21.5) | 3809 (21.2) | 0.01 |
| aPropensity score matching was performed on age at index, sex, race, body mass index, status of comorbidities (including diabetes mellitus, hypertension, hyperlipidaemia, cerebrovascular diseases, vitamin D deficiency, chronic kidney disease), status of comedication use (glucocorticoids, methotrexate, dupilumab, antidepressants), lab data (C-reactive protein), status of smoking, alcoholism and substance use, medical utilization status (ambulatory and acute inpatient visit), and socioeconomic status (problems related to housing and economic circumstances, persons with potential health hazards related to socioeconomic and psychosocial circumstances). PN: prurigo nodularis; SMD: standardized mean difference. Bold font represents a standardized mean difference of more than 0.1. |
||||||
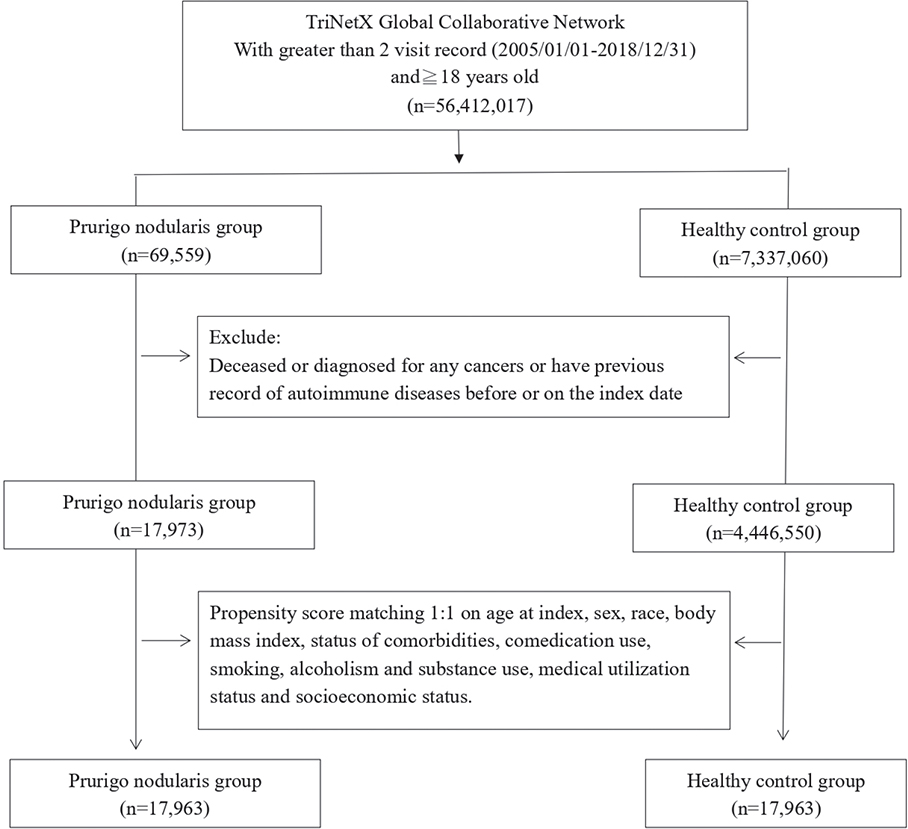
Fig. 1. Patient selection process. In the current study, autoimmune diseases includes ankylosing spondylitis, rheumatoid arthritis (with or without rheumatic factor positive), systemic lupus erythematosus, Sjögren’s syndrome, psoriasis, inflammatory bowel diseases, and dermatopolymyositis).
In all analyses, the statistical analytic function of the TriNetX research network (TriNetX research network) was applied. Python 3.12.7 (https://www.python.org/downloads/release/python-3127/) was also utilized. We conducted 1:1 nearest-neighbour propensity score matching, using a caliper width of 0.1 pooled standard deviations of the logit of the propensity score, as per the default configuration in the TriNetX platform. Calculating standardized mean differences (SMD), the difference in baseline characteristics was present before and after matching between PN group and control group. When SMD value surpassed 0.1, the difference between 2 cohorts was considered to be significant. Cox proportional hazards regression models were used to estimate hazard ratios (HRs) for the development of autoimmune diseases. The timescale for the survival analysis was defined as the respective wash-out period (in most analyses, 3 months) from the index date to the first occurrence of an autoimmune outcome. The follow-up time was defined as the duration from the end of the wash-out period to the first occurrence of the outcome or the end of data availability, whichever occurred first. Due to platform limitations, the TriNetX analytics environment does not support formal testing of the proportional hazard’s assumption (e.g., via Schoenfeld residuals). The significance of the findings was determined using 95% confidence intervals (95% CIs) for the HRs.
RESULTS
Baseline characteristics of the study participants
Table I displays the baseline characteristics of the PN and control cohorts, both before and after propensity score matching. Before matching, the PN cohort contained 17,973 eligible patients, and the non-PN control group contained 4,446,550 patients. After matching, the PN cohort had 17,963 patients, and the non-PN control group had the same number of patients. The PN cohort had a significantly higher mean age (45.0 ± 19.3 years) compared with the control cohort (34.7 ± 20.3 years) before matching. Sex distribution also differed slightly, with females representing 58.1% of the PN cohort and 53.6% of the control cohort. There were notable racial differences, with a higher percentage of White individuals in the control cohort (55.8%) compared with the PN cohort (45.9%). The PN cohort also showed higher prevalence rates for comorbidities including hypertension, hyperlipidaemia, and diabetes mellitus. Following matching, the SMDs for all baseline variables were reduced to under 0.1, signifying balanced matching across demographics, comorbidities, and medical utilization status.
Risk of autoimmune diseases in PN patients
The risk of autoimmune diseases in the PN patients is presented in Fig. 2. Compared with the control cohorts, individuals with PN were significantly more likely to develop SLE (HR: 2.16, 95% CI: 1.44–3.24), Sjögren’s syndrome (HR: 1.86, 95% CI: 1.33–2.59) and psoriasis (HR: 3.20, 95% CI: 2.58–3.97) in a 15-year follow-up period. However, other autoimmune diseases such as AS (HR: 1.41, 95% CI: 0.76–2.60), RA (HR: 1.03, 95% CI: 0.60–1.77), CD (HR: 0.98, 95% CI: 0.60–1.61) and UC (HR: 1.09, 95% CI: 0.74–1.62), presented insignificant risk in PN patients. The PN group had a mean follow-up time of 5.95 years (standard deviation: 4.48 years), with a median follow-up of 5.93 years and an interquartile range (IQR) of 7.74 years. Similarly, the PN-free control group had a mean follow-up of 6.19 years (standard deviation: 3.96), with a median follow-up of 6.25 years and an IQR of 5.80 years. Kaplan–Meiers plot of each outcome are presented in Fig. S1.

Fig. 2. Forest plot of autoimmune diseases risk in prurigo nodularis patients. The PN group had a mean follow-up time of 5.95 years (standard deviation: 4.48 years), with a median follow-up of 5.93 years and an interquartile range (IQR) of 7.74 years. Similarly, the PN-free control group had a mean follow-up of 6.19 years (standard deviation: 3.96), with a median follow-up of 6.25 years and an IQR of 5.80 years. Propensity score matching was performed on age at index, sex, race, body mass index, status of comorbidities (including diabetes mellitus, hypertension, hyperlipidaemia, cerebrovascular diseases, vitamin D deficiency, chronic kidney disease), status of comedication use (glucocorticoids, methotrexate, dupilumab, antidepressants), lab data (C-reactive protein), status of smoking, alcoholism and substance use, medical utilization status (ambulatory and acute inpatient visit), and socioeconomic status (problems related to housing and economic circumstances, persons with potential health hazards related to socioeconomic and psychosocial circumstances). Wash-out period was set as 3 months after index date. The follow-up time was set as 15 years.
Stratification analysis
The stratified analysis by sex and age revealed distinct patterns in autoimmune disease risk among PN patients (Tables II and III). Psoriasis risk in females was elevated, with an HR of 2.39 (95% CI: 1.83–3.13). For males with PN, the risk of psoriasis was particularly high, with an HR of 5.92 (95% CI: 3.90–8.99), indicating a more than fivefold increase compared with male controls. However, other diseases, such as SLE (HR: 1.61, 95% CI: 0.57–4.53) and Sjögren’s syndrome (HR: 0.66, 95% CI: 0.26–1.70), did not show elevated risks in males. In contrast, female PN patients exhibited a notably higher risk of SLE (HR: 2.96, 95% CI: 1.80–4.87) and Sjögren’s syndrome (HR: 2.47, 95% CI: 1.67–3.64). AS, RA, and CD showed no significant association with PN in the age and sex stratification analysis. However, in PN patients aged 18 to 64, a significant risk of UC was observed (HR: 2.75, 95% CI: 1.49–5.08).
| Outcomes | Male | Female | ||||
| PN cohort (%)a | Control cohort (%) | HR (95% CI)a | PN cohort (%)a | Control cohort (%) | HR (95% CI)a | |
| Ankylosing spondylitis | 10 (≤ 0.1) | 10 (≤ 0.1) | 2.18 (0.66, 7.25) | 16 (0.2) | 10 (≤ 0.1) | 2.33 (0.96, 5.66) |
| Rheumatoid arthritis | 10 (≤ 0.1) | 10 (≤ 0.1) | 0.99 (0.32, 3.08) | 21 (0.2) | 30 (0.3) | 0.70 (0.40, 1.22) |
| Systemic lupus erythematosus | 10 (≤ 0.1) | 10 (≤ 0.1) | 1.61 (0.57, 4.53) | 59 (0.6) | 21 (0.2) | 2.96 (1.80, 4.87) |
| Sjögren’s syndrome | 10 (≤ 0.1) | 11 (0.2) | 0.66 (0.26, 1.70) | 88 (0.8) | 36 (0.3) | 2.47 (1.67, 3.64) |
| Psoriasis | 144 (2.0) | 26 (0.4) | 5.92 (3.90, 8.99) | 173 (1.7) | 76 (0.7) | 2.39 (1.83, 3.13) |
| Crohn disease | 10 (≤ 0.1) | 10 (≤ 0.1) | 1.31 (0.52, 3.32) | 19 (0.2) | 14 (≤ 0.1) | 1.39 (0.70, 2.77) |
| Ulcerative colitis | 20 (0.3) | 10 (≤ 0.1) | 2.05 (0.96, 4.39) | 28 (0.3) | 34 (0.3) | 0.82 (0.49, 1.35) |
| aPropensity score matching was performed on age at index, sex, race, body mass index, status of comorbidities (including diabetes mellitus, hypertension, hyperlipidaemia, cerebrovascular diseases, vitamin D deficiency, chronic kidney disease), status of comedication use (glucocorticoids, methotrexate, dupilumab, antidepressants), lab data (C-reactive protein), status of smoking, alcoholism and substance use, medical utilization status (ambulatory and acute inpatient visit), and socioeconomic status (problems related to housing and economic circumstances, persons with potential health hazards related to socioeconomic and psychosocial circumstances). PN: prurigo nodularis; 95% CI: 95% confidence interval; HR: hazard ratio. On the TriNetX analytics platform, for deidentification purposes, if the number of incident cases is 10 or fewer, it will be reported as 10. The bold content refers to significant hazard ratio. |
||||||
| Outcomes | 18–64 years old | Older than 65 years old | ||||
| PN cohort (%)a | Control cohort (%) | HR (95% CI)a | PN cohort (%)a | Control cohort (%) | HR (95% CI)a | |
| Ankylosing spondylitis | 19 (0.2) | 10 (≤ 0.1) | 2.17 (0.98, 4.80) | 10 (≤ 0.1) | 10 (≤ 0.1) | 1.08 (0.31, 3.73) |
| Rheumatoid arthritis | 17 (≤ 0.1) | 13 (≤ 0.1) | 1.29 (0.63, 2.67) | 10 (≤ 0.1) | 14 (0.2) | 0.75 (0.33, 1.70) |
| Systemic lupus erythematosus | 49 (0.4) | 21 (0.2) | 2.39 (1.43, 3.98) | 23 (0.4) | 16 (0.2) | 1.57 (0.83, 2.98) |
| Sjögren’s syndrome | 51 (0.4) | 22 (0.2) | 2.29 (1.39, 3.77) | 48 (0.7) | 31 (0.5) | 1.66 (1.06, 2.61) |
| Psoriasis | 223 (1.9) | 70 (0.6) | 3.31 (2.53, 4.33) | 110 (1.7) | 51 (0.8) | 2.38 (1.71, 3.33) |
| Crohn disease | 22 (0.2) | 15 (≤ 0.1) | 1.50 (0.78, 2.89) | 10 (≤ 0.1) | 10 (≤ 0.1) | 1.42 (0.53, 3.82) |
| Ulcerative colitis | 38 (0.3) | 14 (≤ 0.1) | 2.75 (1.49, 5.08) | 13 (0.2) | 14 (0.2) | 1.00 (0.47, 2.13) |
| aPropensity score matching was performed on age at index, sex, race, body mass index, status of comorbidities (including diabetes mellitus, hypertension, hyperlipidaemia, cerebrovascular diseases, vitamin D deficiency, chronic kidney disease), status of comedication use (glucocorticoids, methotrexate, dupilumab, antidepressants), lab data (C-reactive protein), status of smoking, alcoholism and substance use, medical utilization status (ambulatory and acute inpatient visit), and socioeconomic status (problems related to housing and economic circumstances, persons with potential health hazards related to socioeconomic and psychosocial circumstances). PN: prurigo nodularis; 95% CI: 95% confidence interval; HR: hazard ratio. On the TriNetX analytics platform, for deidentification purposes, if the number of incident cases is 10 or fewer, it will be reported as 10. The bold content refers to significant hazard ratio. |
||||||
Sensitivity analysis
In sensitivity analyses using alternative definitions and algorithms, increased risks for psoriasis, SLE, and Sjögren’s syndrome in the PN cohort remained robustly significant. For example, applying stricter PN criteria with frequently used medications (Table SIII, Algorithm 3), psoriasis risk showed an HR of 3.81 (95% CI: 2.94–4.93), with stable associations for SLE (HR: 1.91) and Sjögren’s syndrome (HR: 2.00). In shorter follow-up periods of 5 and 10 years, risks for psoriasis (HR: 2.92 and 2.70, respectively), SLE, and Sjögren’s syndrome remained significant, while risks for AS, RA, UC, and CD consistently showed no significance (Table SIV). Similarly, across wash-out periods of 12, 24, and 36 months, risks for psoriasis, SLE, and Sjögren’s syndrome remained stable, with an HR of 3.14 for psoriasis at 12 months and 2.96 at 36 months (Table SV). Matching for various covariates maintained significant associations for psoriasis, SLE, and Sjögren’s syndrome, while AS, RA, UC, and CD showed no significant association (Table SVI). After excluding patients with atopic dermatitis or psoriasis, PN remained significantly associated with increased risks of SLE, Sjögren’s syndrome, and psoriasis, but not RA, CD, or UC (Tables SVII and SVIII). Similar results were observed after excluding those with type 1 diabetes or thyroid disorders, with significant associations for SLE, Sjögren’s syndrome, psoriasis, UC, and ankylosing spondylitis, while RA and CD remained non-significant (Tables SIX and SX). Using different active comparators validated an elevated risk for psoriasis across all groups: HR 1.40 with HS, 2.23 with AA, and 1.82 with rosacea. SLE and Sjögren’s syndrome risks were significant only in the HS comparison, not with AA or rosacea (Table SXI). These findings support consistent associations of PN with psoriasis, SLE, and Sjögren’s syndrome across varying sensitivity analyses.
DISCUSSION
Our study showed that PN is associated with increased risks of SLE, Sjögren’s syndrome, and psoriasis, with the psoriasis risk notably higher than in other inflammatory skin diseases like HS, AA, and rosacea. These findings offer large-scale, real-world evidence to support the autoimmune comorbidity profile of PN.
PN is marked by a shift from Th2 responses to a pro-fibrotic state driven by COL11A1+ fibroblasts and keratinocyte interactions. It involves chronic inflammation and T-cell–mediated cytokines (IL-4, IL-13, IL-31), which are also implicated in autoimmune diseases (15–18). Our analysis showed a strong association between PN and psoriasis (HR 3.20, 95% CI: 2.58–3.97), aligning with previous findings (6), though psoriasis is not a classical but still considered an autoimmune disorder. Psoriasis is driven by the Th1/IL-23/IL-17 axis, while PN is primarily mediated by Th2 responses (1, 19). Both conditions share skin barrier dysfunction, which may promote a bidirectional inflammatory cycle and their coexistence (20). Moreover, IL-22, a major pro-inflammatory cytokine produced by Th17, Th22, NK, and γδ T cells, may represent another crucial link between PN and psoriasis (21). Elevated IL-22 levels, linked to chronic inflammatory diseases like coronary artery disease and type II diabetes, may contribute to comorbidities in psoriasis and PN patients (6, 22–24). Its role in promoting keratinocyte hyperplasia and acanthosis, which are hallmark features of both PN and psoriasis, suggests that systemic IL-22 expression could drive disease progression in both conditions (25). Given that IL-22 promotes keratinocyte proliferation and acts synergistically with IL-17 to upregulate antimicrobial peptides, the Th22/IL-22 polarization observed in PN may reflect a shared inflammatory pathway with psoriasis, contributing to their coexistence in patients (26,27). Additionally, although IL-17 plays a central role in psoriasis, studies have shown its involvement in some Th2-driven diseases as well (28). A 2020 study on cutaneous transcriptomics found that PN and psoriasis share more genetic similarities than either does with atopic dermatitis (29). Among the shared differentially expressed genes (DEGs) between PN and psoriasis, several are related to the Th17/Th22 pathways (e.g., CXCL1, DEFB4A, S100A7/8/9), suggesting common immune-driven mechanisms and further reinforcing the link between these 2 conditions. However, psoriasis often occurs before age 45, which is close to the mean age of PN patients in this study. Although psoriasis and PN share symptoms like pruritus and their association has been confirmed across models with different wash-out periods and proxy algorithms, potential misclassification and reverse causation biases should not be overlooked. The role of common biologics for both PN and psoriasis is also worth noting. While dupilumab is a potential treatment for refractory PN, especially in patients with comorbid AD, it has been associated with new or worsening psoriasis (30). Caution is advised when using dupilumab in PN patients with psoriasis, and combination therapies such as dupilumab with ustekinumab may offer a solution, pending further research (31).
Our analysis found a significantly increased risk of SLE in PN patients (HR: 2.16), though this was not significant in males. Given the clinical heterogeneity of SLE, especially its cutaneous forms, further research is needed to assess whether specific subtypes are more strongly linked to PN. The PN–Sjögren’s syndrome association was generally supported, but became non-significant under stricter PN definitions, suggesting possible misclassification bias. As for ulcerative colitis, a significant association was observed only in younger PN patients, while most models showed no consistent link, highlighting uncertainty in contrast to earlier studies suggesting associations with both UC and Crohn’s disease (6). Interestingly, while no significant association was observed between PN and RA in the primary analysis, sensitivity analyses using inflammatory skin diseases such as AA and rosacea as comparators revealed a relatively lower risk of RA among PN patients. This discrepancy may be attributed to underlying immunological differences. PN is predominantly associated with Th2- and Th22-skewed inflammation, characterized by elevated levels of IL-4, IL-13, and IL-31(27), whereas RA and AA are driven by Th1 or Th17 pathways, involving interferon-γ, TNF-α, IL-6, and IL-17 (32, 33). These divergent immune profiles may result in differential susceptibility to systemic autoimmune joint involvement. These findings highlight the complexity of immune dysregulation in PN and underscore the need for mechanistic studies exploring disease-specific immune trajectories and cross-organ immune interactions.
Prior epidemiological studies have established significant associations between PN and both diabetes mellitus and thyroid disorders (6,7). Given the existing strength of evidence and our intent to investigate less well-characterized autoimmune comorbidities, we did not include diabetes and thyroid disease as primary outcome endpoints. Nevertheless, both conditions are clinically relevant and may influence the associations between PN and other autoimmune outcomes. To account for this potential confounding, we conducted additional sensitivity analyses. The associations between PN and SLE, Sjögren’s syndrome, and psoriasis remained consistent with the findings from the main analyses. However, inconsistent associations were observed for AS and UC. Given the relatively small number of incident cases for these outcomes, the statistical power was limited. These findings may be subject to confounding and misclassification biases, underscoring the need for future studies with larger datasets to validate these associations.
Our study focused on common autoimmune diseases based on existing literature; however, it is essential to acknowledge that the autoimmune comorbidity profile associated with PN may vary across populations. For example, studies based on Western population have reported a higher co-occurrence of PN with autoimmune thyroiditis, type 1 diabetes mellitus, and coeliac disease (34). A population-based claims analysis from Germany further highlighted unique comorbidity patterns in European PN patients (35). Ethnic, geographic, and environmental differences, along with healthcare access and diagnostic practices, may shape the spectrum of autoimmune diseases linked to PN. To enhance the generalizability and precision of PN comorbidity profiling, future research should consider stratified analyses by geographic region or ancestry.
The strength of this study included the use of propensity score matching to reduce confounding, sensitivity analyses with stricter PN definitions to minimize misclassification, and inclusion of active comparators to validate observed associations. Limitations of this study should be stated. The retrospective design of the current study restricts our ability to determine a causal link between PN and the risk of autoimmune diseases. There is also the possibility of reverse causality, meaning the observed risk differences cannot be directly attributed to PN. As an observational study, our results may be subject to survival bias, where patients who live longer are overrepresented. Additionally, despite adjusting for known variables, unmeasured confounders, such as environmental factors or genetic predispositions, may introduce residual confounding. (36), potentially influencing the current results. Moreover, because TriNetX data are derived from a network of selected healthcare institutions, there is a risk of selection bias, as the patient population may not fully represent the general population. The use of administrative data also raises concerns about incomplete diagnoses, which could introduce potential misclassification bias. Furthermore, it is unclear whether all diagnoses were made by specialists, further increasing the risk of misclassification. Issue of generalizability should also be considered. Though the current study applied a global-federated electronic health record database, patient-level geographic identifiers are not accessible within the analytic environment. As a result, we are unable to report country- or region-specific baseline distributions.
In summary, our study demonstrates a strong association between PN and several autoimmune diseases, particularly psoriasis, SLE, and Sjögren’s syndrome. These findings highlight the need for further research into the underlying mechanisms and potential targeted therapies.
ACKNOWLEDGEMENTS
This study is partially supported by the funding from Chung Shan Medical University Hospital (CSH-2025-C-007) and the Taiwan Global Pathfinders Initiative (Program No:190).
Data availability statement: Data in this study were retrieved from TriNetX Research Network. All data available in the database were administrated by the TriNetX platform. Detailed information can be retrieved at the official website of the research network (https://trinetx.com).
Ethics declarations and trial registry information: This research has been approved by Institutional Review Board of Chung Shan Medical University Hospital (IRB No. CS1-25002) and the need for informed consent is exempted by the Institutional Review Board. Trial registry is not applicable as the current study is not a clinical trial.
REFERENCES
- Shao Y, Wang D, Zhu Y, Xiao Z, Jin T, Peng L, et al. Molecular mechanisms of pruritus in prurigo nodularis. Front Immunol 2023; 14: 1301817. https://doi.org/10.3389/fimmu.2023.1301817
- McCampbell LE, Zaino ML, Ranpariya M, Patel T, Feldman SR. Systemic medication for the treatment of prurigo nodularis: a systematic review. J Cutan Med Surg 2023; 27: 641–645. https://doi.org/10.1177/12034754231211797
- Williams KA, Huang AH, Belzberg M, Kwatra SG. Prurigo nodularis: pathogenesis and management. J Am Acad Dermatol 2020; 83: 1567–1575. https://doi.org/10.1016/j.jaad.2020.04.182
- Brooks SG, Yosipovitch G. Prurigo nodularis in 2025: current and emerging treatments. Clin Dermatol 2025; S0738-081X(25)00096-3. https://doi.org/10.1016/j.clindermatol.2025.03.013
- Geng RSQ, Sood S, Waked J, Mahmood R, Maliyar K, Sachdeva M, et al. Disease severity and pruritus treatment outcomes in prurigo nodularis: a systematic review of randomized-controlled trials. J Am Acad Dermatol 2025; 93: 263–265. https://doi.org/10.1016/j.jaad.2025.03.009
- Huang AH, Canner JK, Khanna R, Kang S, Kwatra SG. Real-world prevalence of prurigo nodularis and burden of associated diseases. J Invest Dermatol 2020; 140: 480–483.e484. https://doi.org/10.1016/j.jid.2019.07.697
- Woo YR, Wang S, Sohn KA, Kim HS. Epidemiology, comorbidities, and prescription patterns of Korean prurigo nodularis patients: a multi-institution study. J Clin Med 2021; 11. https://doi.org/10.3390/jcm11010095
- Gau S-Y, Lo S-W, Hsu C, Chen S-J, Zuberbier T, Chang H-C. Human papillomavirus infection is associated with increased risk of new-onset hidradenitis suppurativa: a population-based cohort study. J Am Acad Dermatol 2025; 92: 444–451. https://doi.org/10.1016/j.jaad.2024.10.055.
- Chang H-C, Lin C-Y, Guo Y-C, Lu H-Y, Lee C-Y, Wu M-C, et al. Association between hidradenitis suppurativa and atopic diseases: a multi-center, propensity-score-matched cohort study. Int J Med Sci 2024; 21: 299–305. https://doi.org/10.7150/ijms.90086
- Chang H-C, Wu C-L, Chiu T-M, Liao W-C, Gau S-Y. Risk of osteoarthritis in patients with hidradenitis suppurativa: a global federated health network analysis. Front Immunol 2023; 14. https://doi.org/10.3389/fimmu.2023.1285560
- Roh YS, Marani M, Choi U, Sutaria N, Parthasarathy V, Deng J, et al. Validation of International Classification of Diseases Tenth Revision code for prurigo nodularis. J Am Acad Dermatol 2022; 87: 482–484. https://doi.org/10.1016/j.jaad.2021.10.026
- Fry L, Baker BS, Powles AV, Engstrand L. Psoriasis is not an autoimmune disease? Exp Dermatol 2015; 24: 241–244. https://doi.org/10.1111/exd.12572
- Liu A, Liao P, Jiang H, Huang S, Li S, Wei JC, et al. COVID-19 vaccination reduces new-onset fibromyalgia risk in survivors. BMC Med 2025; 23: 255. https://doi.org/10.1186/s12916-025-04069-z
- Li CP, Lo SW, Tsai RY, Chang HC, Gau SY. New-onset hidradenitis suppurativa in psoriasis patients: a multi-center, retrospective cohort study. Life (Basel, Switzerland) 2024; 14. https://doi.org/10.3390/life14060730
- Schuler CFt, Billi AC, Maverakis E, Tsoi LC, Gudjonsson JE. Novel insights into atopic dermatitis. J Allergy Clin Immunol 2023; 151: 1145–1154. https://doi.org/10.1016/j.jaci.2022.10.023
- Yang G, Seok JK, Kang HC, Cho YY, Lee HS, Lee JY. Skin barrier abnormalities and immune dysfunction in atopic dermatitis. Int J Mol Sci 2020; 21. https://doi.org/10.3390/ijms21082867
- Vermeer E, Hebing RCF, van de Meeberg MM, Lin M, de Meij TGJ, Struys EA, et al. Oral versus subcutaneous methotrexate in immune-mediated inflammatory disorders: an update of the current literature. Curr Rheumatol Rep 2023; 25: 276–284. https://doi.org/10.1007/s11926-023-01116-7
- Ma F, Gharaee-Kermani M, Tsoi LC, Plazyo O, Chaskar P, Harms P, et al. Single-cell profiling of prurigo nodularis demonstrates immune-stromal crosstalk driving profibrotic responses and reversal with nemolizumab. J Allergy Clin Immunol 2024; 153: 146–160. https://doi.org/10.1016/j.jaci.2023.07.005
- Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci 2019; 20. https://doi.org/10.3390/ijms20061475
- Kwatra SG. Breaking the itch–scratch cycle in prurigo nodularis. N Engl J Med 2020; 382: 757–758. https://doi.org/10.1056/NEJMe1916733
- Jiang Q, Yang G, Xiao F, Xie J, Wang S, Lu L, et al. Role of Th22 Cells in the pathogenesis of autoimmune diseases. Front Immunol 2021; 12: 688066. https://doi.org/10.3389/fimmu.2021.688066
- Gong F, Wu J, Zhou P, Zhang M, Liu J, Liu Y, et al. Interleukin-22 might act as a double-edged sword in type 2 diabetes and coronary artery disease. Mediators Inflamm 2016; 2016: 8254797. https://doi.org/10.1155/2016/8254797
- Daudén E, Castañeda S, Suárez C, García-Campayo J, Blasco AJ, Aguilar MD, et al. Clinical practice guideline for an integrated approach to comorbidity in patients with psoriasis. J Eur Acad Dermatol Venereol 2013; 27: 1387–1404. https://doi.org/10.1111/jdv.12024
- Zheng Y, Li T. Interleukin-22, a potent target for treatment of non-autoimmune diseases. Hum Vaccin Immunother 2018; 14: 2811–2819. https://doi.org/10.1080/21645515.2018.1509649
- Mashiko S, Bouguermouh S, Rubio M, Baba N, Bissonnette R, Sarfati M. Human mast cells are major IL-22 producers in patients with psoriasis and atopic dermatitis. J Allergy Clin Immunol 2015; 136: 351–359.e351. https://doi.org/10.1016/j.jaci.2015.01.033
- Wolk K, Witte E, Wallace E, Döcke WD, Kunz S, Asadullah K, et al. IL-22 regulates the expression of genes responsible for antimicrobial defense, cellular differentiation, and mobility in keratinocytes: a potential role in psoriasis. Eur J Immunol 2006; 36: 1309–1323. https://doi.org/10.1002/eji.200535503
- Belzberg M, Alphonse MP, Brown I, Williams KA, Khanna R, Ho B, et al. Prurigo nodularis is characterized by systemic and cutaneous T helper 22 immune polarization. J Invest Dermatol 2021; 141: 2208–2218.e2214. https://doi.org/10.1016/j.jid.2021.02.749
- Furue M. Regulation of filaggrin, loricrin, and involucrin by IL-4, IL-13, IL-17A, IL-22, AHR, and NRF2: pathogenic implications in atopic dermatitis. Int J Mol Sci 2020; 21. https://doi.org/10.3390/ijms21155382
- Sutaria N, Alphonse MP, Roh YS, Choi J, Parthasarathy V, Deng J, et al. Cutaneous transcriptomics identifies fibroproliferative and neurovascular gene dysregulation in prurigo nodularis compared with psoriasis and atopic dermatitis. J Invest Dermatol 2022; 142: 2537–2540. https://doi.org/10.1016/j.jid.2022.02.010
- Su Z, Zeng YP. Dupilumab-associated psoriasis and psoriasiform manifestations: a scoping review. Dermatology 2023; 239: 646–657. https://doi.org/10.1159/000530608
- Kabbani M, Mboyo Mpita G, Benhadou F. Ustekinumab plus dupilumab in the treatment of concomitant psoriasis and prurigo nodularis. J Eur Acad Dermatol Venereol 2022; 36: e1050–e1051. https://doi.org/10.1111/jdv.18445
- McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med 2011; 365: 2205–2219. https://doi.org/10.1056/NEJMra1004965
- Strazzulla LC, Wang EHC, Avila L, Lo Sicco K, Brinster N, Christiano AM, et al. Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. J Am Acad Dermatol 2018; 78: 1–12. https://doi.org/10.1016/j.jaad.2017.04.1141
- Yook HJ, Lee JH. Prurigo nodularis: pathogenesis and the horizon of potential therapeutics. Int J Mol Sci 2024; 25: 5164. https://doi.org/10.3390/ijms25105164
- Augustin M, Garbe C, Hagenström K, Petersen J, Pereira MP, Ständer S. Prevalence, incidence and presence of comorbidities in patients with prurigo and pruritus in Germany: a population-based claims data analysis. J Eur Acad Dematol Venereol 2021; 35: 2270–2276. https://doi.org/10.1111/jdv.17485
- Gau SY. Methotrexate use and liver outcomes in psoriasis and rheumatoid arthritis patients: a commentary on “Risk of liver disease in patients with psoriasis, psoriatic arthritis and rheumatoid arthritis receiving methotrexate: A population-based study”. J Am Acad Dermatol 2021; 85: e399–e400. https://doi.org/10.1016/j.jaad.2021.07.069