ORIGINAL REPORT
LAight Therapy is an Effective and Gentle Treatment in Adolescents Suffering from Hidradenitis Suppurative: Results from 96 Patients Using Real-world Data
Alexandra STROBEL1,2, Michael SCHULTHEIS3, Petra STAUBACH3, Stephan GRABBE3, Katharina HENNIG3, Jacek SZEPIETOWSKI4, Łukasz MATUSIAK4, Esther VON STEBUT5, Uwe KIRSCHNER6, Hans BAYER7, Georgios NIKOLAKIS8 and Simone GARCOVICH9
1Institute of Medical Epidemiology, Biostatistics, and Informatics, Interdisciplinary Center for Health Sciences, Medical Faculty of Martin Luther University Halle-Wittenberg, Germany, 2Institute of Health, Midwifery and Nursing Science, Medical Faculty of Martin Luther University Halle-Wittenberg, University Medicine Halle, Germany, 3Department of Dermatology, University Medical Center, Johannes Gutenberg University, Mainz, Germany, 4Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, 5Department of Dermatology, University of Cologne, Faculty of Medicine, Cologne, Germany, 6Dermatology Outpatient Office Dr. Uwe Kirschner, Mainz, Germany, 7Dermatology Outpatient Office Hautmedizin Bad Soden, Bad Soden, Germany, 8Brandenburg Medical School Theodor Fontane, Department of Dermatology, Dessau Medical Center, Dessau, Germany, and 9Unicamillus, Faculty of Medicine, Rome, Italy
Hidradenitis suppurativa (HS) is a chronic skin condition characterized by the formation of painful nodules, abscesses, and tunnels, typically in intertriginous areas. While HS primarily affects adults, it causes in particular severe distress when it affects adolescent patients. Physicians prefer to avoid the use of systemic medications and surgery in children due to the potential side effects, psychological burden, and long-term consequences. The device-based LAight® therapy combines intense pulsed light and radiofrequency and received EU-wide approval in 2017 for the treatment of adults with all severities of HS. Since 2017, 96 adolescent patients in Germany and Austria have been treated off-label with LAight. A mixed model for repeated measures over 36 weeks on the endpoints Hidradenitis Suppurativa Severity Score System (IHS4), NRS Pain, and Dermatology Life Quality Index (DLQI) showed that patients starting treatment with a high burden significantly benefited from treatment, while those starting with a low burden could be effectively stabilized at a low level. HS and its management can cause considerable stress and anxiety for children and their families. Gentle and well-tolerated treatments, such as LAight therapy, can contribute to a more positive experience for patients and consequently improve their quality of life.
SIGNIFICANCE
Hidradenitis suppurativa in children and adolescents is a challenging disease with limited treatment options in current guidelines. Physical treatment of active inflammatory lesions of hidradenitis suppurativa with energy-based devices is rapidly increasing in adult patients but is poorly described in the paediatric patient population. LAight therapy, a combination of intense pulsed light and radiofrequency, has recently been shown to be beneficial in adult patients with HS across all severity levels. This retrospective study analysed the real-world use of this physical treatment protocol in paediatric hidradenitis suppurativa patients and found an overall improvement in clinical as well as patient-reported outcomes.
Key words: adolescence; paediatric; hidradenitis suppurativa; device-based therapy; side-effects; LAight therapy.
Citation: Acta Derm Venereol 2025; 105: adv43543. DOI: https://doi.org/10.2340/actadv.v105.43543.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 4, 2025. Accepted after revision: Aug 19, 2025. Published: Sep 22, 2025.
Corr: Michael Schultheis, MD, Johannes Gutenberg University, Department of Dermatology, University Medical Center, Langenbeckstraße 1, DE-55131, Mainz, Germany. Email: michael.schultheis@unimedizin-mainz.de
Competing interests and funding: The implementation of the questionnaire in the LENICURA software was provided free of charge by LENICURA GmbH. No other funding was received.
INTRODUCTION
Hidradenitis suppurativa (HS) is a chronic inflammatory follicular condition characterized by painful, recurrent lesions in intertriginous skin regions, leading to tissue damage and scarring. HS can manifest in the paediatric age group, affecting both children and adolescents, with a higher incidence observed in females. The clinical phenotype typically presents similarly to adult-onset HS (1). Paediatric HS constitutes a distinct patient population with unique clinical considerations and remains significantly underrepresented in research compared to adult disease. Procedural and physical therapies, including lasers and energy-based devices (EBDs), are increasingly used for the management of adult HS, but poorly described in the paediatric patient population (2). The EBD protocol LAight therapy®, which uniquely combines intense-pulsed light (IPL) and radiofrequency (RF), represents a novel physical adjunctive treatment for adult HS. It gained European approval in 2017 for use across all severity stages of HS (3). Technical details can be found in Table I. LAight therapy is performed in outpatient centres across Germany and Austria and is accompanied by specific manufacturer-provided software, which facilitates standardized data collection following patient-informed consent.
| Treatment passes | RF* intensities in J/cm2 | Impulse characteristics RF | IPL* wavelength interval in nm | IPL intensities in J/cm2 | Impulse characteristics IPL |
| 1st treatment pass | 12.2 | 1 impulse with 1 s duration and frequency of 1 MHz | 420–1200 | 6.0 | 4 sub-impulses with 8 ms duration and 8 ms pause |
| 2nd treatment pass | 12.2 | 1 impulse with 1 s duration and frequency of 1 MHz | 510–1200 | 5.6 | 4 sub-impulses with 8 ms duration and 8 ms pause |
| 3rd treatment pass | 12.2 | 1 impulse with 1 s duration and frequency of 1 MHz | 690–1200 | 4.4 | 4 sub-impulses with 8 ms duration and 8 ms pause |
| *RF: radiofrequency; IPL: intense pulsed light. | |||||
The primary objective of this study was to report the “real-world” safety and effectiveness of LAight therapy in HS patients aged less than 18 years during a period of 36 weeks.
MATERIALS AND METHODS
The real-world data presented in this publication were analysed by the international consortium of the EpiCAi (Epidemiology and Care in Acne inversa) project led by the Department of Dermatology, University Medical Centre Mainz, Germany. For the retrospective study, the legal guardians of all included children and adolescents with HS gave written consent for the documentation and analysis of data collected during routine care with LAight therapy in the manufacturer’s software. Patient data were extracted from the treatment databases of the LAight therapy provider network. The anonymised data were subsequently submitted to the Institute of Medical Biometry at Martin Luther University Halle-Wittenberg for independent evaluation.
Patients aged less than 18 years were included in the study if they had a confirmed diagnosis of HS by a treating physician and had received at least 1 treatment with LAight therapy. For disease severity (evaluated by medical staff) Hurley staging was documented and the disease activity was measured by the International Hidradenitis Suppurativa Severity Score System (IHS4) as the sum of inflammatory nodules + 2 x number of abscesses + 4 x number of draining tunnels. In addition, the patient-reported outcomes (PROs), pain on the numeric rating scale from zero “no pain” to 10 “worst pain imaginable” (NRS Pain), and the Dermatology Life Quality Index (DLQI) were collected.
Statistical analysis
Data on sociodemographic variables, risk factors, and disease-describing instruments were analysed using means and corresponding standard deviations or relative/absolute frequencies. All endpoints, including IHS4, NRS Pain, and DLQI, were analysed using a linear mixed model for repeated measures (MMRM), including 36 weeks of LAight therapy treatment, with a distinction between patients according to their baseline values. The first subgroup (group A) included patients with relevant disease activity (at least 3 active inflammatory lesions) and burden (NRS Pain ≥ 3, DLQI ≥ 6), allowing for a significant improvement in the respective endpoint. The second subgroup (group B) comprised the remaining patients, who started treatment with low baseline disease activity, in line with the treatment objective of preventing disease progression. To meet the assumptions of linearity and normal distribution, each endpoint was logarithmically transformed. MMRMs were adjusted for sex and Hurley stage at baseline. In addition to presenting changes in endpoints, a responder analysis was performed every fourth week for each endpoint using the following definitions:
- IHS4-55-responder: patients achieving at least 55% reduction in IHS4;
- Pain-responder: patients starting with at least 3 points in NRS Pain and achieving at least 30% reduction of the value and a minimum of 1 point;
- DLQI-responder: patients achieving the minimal clinically important difference of 4 points.
Responder rates were based on observed values; however, missing values were imputed using the estimation obtained from the mixed model. In addition, absolute and relative changes in typical classifications were calculated for all endpoints and the occurrence of adverse events was assessed using descriptive methods.
RESULTS
Patient characteristics
Overall, 96 adolescent patients with a mean age of 15.91 years were included in the study, with a preponderance of female patients (65.63%). Patients presented a typical risk factor profile for paediatric HS, with 38.54% of patients being overweight and obese and 12.99% being active smokers. In terms of disease severity, 87.5% of patients presented with mild to moderate disease (Hurley 1–2 stages), with a mean of 3.39 (± 2.37) body regions affected. The baseline IHS4 score was 10.17 ± 15.48 points and the PROs (NRS Pain and DLQI) were consistent with mild-moderate HS (see Table II). Overall, the patients enrolled in the study were representative of a paediatric HS outpatient population. During the 36-week period, 786 LAight therapy sessions were conducted, with an average mean of 8.26 ± 4.89 sessions per person.
Effects on inflammatory lesions (IHS4)
Unlike for the PROs, collection of the IHS4 is not mandatory in the routine care documentation of LAight therapy. In the analysed population, a valid IHS4 score was documented for 46 patients during the first 5 treatments and these patients were therefore included in the analysis. Of these, 28 (60.87%) had at least 3 inflammatory lesions at baseline and were therefore assigned to group A. The remaining 18 patients (39.13%) were assigned to group B. Table III shows the model estimates for group A with respect to IHS4 under LAight therapy. Hurley stage and gender were not associated with disease activity at baseline. A significant reduction in IHS4 was observed during the 36 weeks of treatment (β = –0.007, 95% CI: –0.009, –0.005, p < 0.001), regardless of disease severity or gender. Derived from the model, patients had 5.7 points at baseline and 4.3 points after 36 weeks of treatment, giving a mean predicted reduction in IHS4 of 1.4 points (24.56%) over the study period (see Fig. 1, panel A). These results are consistent with the responder scores. At week 36, 19.4% of patients from group A achieved IHS4-55 (see Fig. 2, panel A). Patients belonging to group B with low baseline disease burden stabilized during the treatment period with no worsening of disease activity (see Fig. 1, panel A).
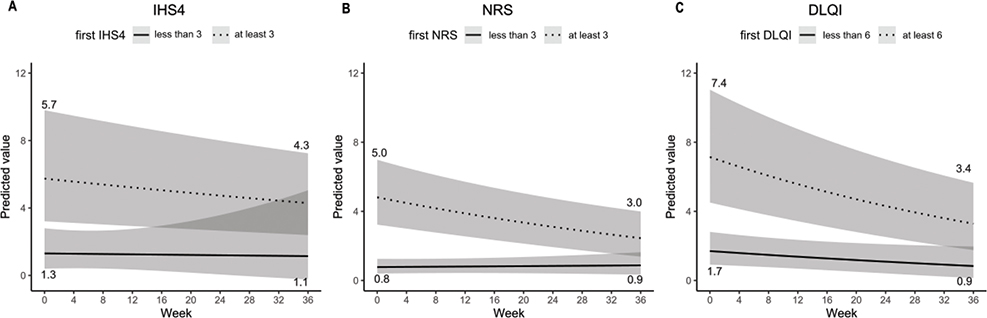
Fig. 1. Predicted values from MMRM for disease activity (IHS4, panel A) and patient-reported outcomes (NRS Pain: panel B, DLQI: panel C). Patients were stratified by baseline disease activity and burden: group A (dotted line) and group B (solid line).
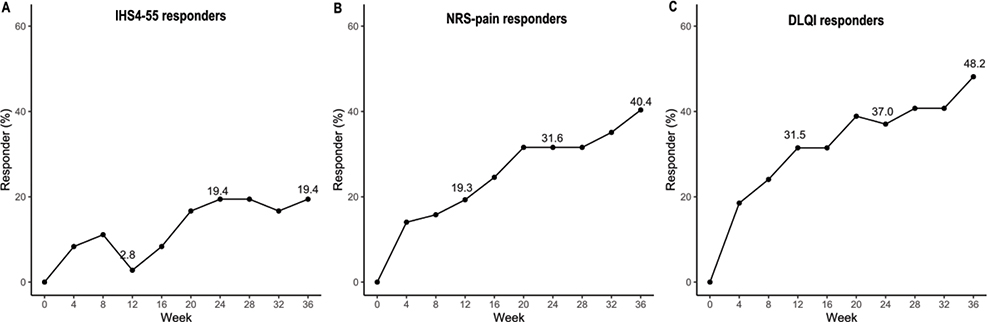
Fig. 2. Responder analysis during 36 weeks of LAight treatment: percentage of patients achieving responder status for outcomes. Panel A: IHS4 (at least 55% improvement of baseline IHS4 score; panel B: NRS Pain (at least 30% improvement of baseline pain numerical rating scale; panel :C DLQI (at least 4-point improvement of baseline Dermatology Life-Quality Index scoring.
Looking at the distribution of disease severity across all patients, there is a noticeable increase in the proportion of patients with mild HS at week 36 (63.0%) compared with baseline (39.1%), indicating an overall positive change in severity distribution (see Fig. 3, panel A).

Fig. 3. Sankey plot showing changes in typical classifications of disease activity and burden for outcomes. Panel A: IHS4 (mild HS: IHS4 <4, moderate HS: IHS4 4–10, severe HS: IHS4>10; panel B: pain (no pain: NRS: 0, mild pain: NRS 1–3, moderate pain: NRS 4–6, severe pain: NRS 7–10; and panel C: quality of life (no effect: DLQI <2, small effect: DLQI 2–5, moderate effect: DLQI 6–10, very large effect: DLQI 11–20; extremely large effect DLQI 21–30).
Effects on pain (NRS)
Of the 96 patients, 57 (59.38%) reported a pain level of at least 3 points at baseline, whereas 39 (40.62%) had a lower score at the initial visit. Table III shows the model estimates for patients with higher starting values (namely, patients from group A) and predicted values of the model are shown in Fig. 1 (panel B). Hurley stage and gender were not associated with the level of pain at baseline; however, a significant mean reduction of 2 points on NRS Pain (40.0%) during 36 weeks of care was observed. Response rates gradually increased over time, reaching 40.4% after 36 weeks (Fig. 2, panel B). In line with the observations from IHS4, patients from group B maintained their low baseline level of pain. Across the whole cohort, a relevant shift in pain categories was observed leaving just 2.1% of patients with severe pain in contrast to 24.0% at baseline (see Fig. 3, panel B).
Effects on quality of life (DLQI)
Table III shows the log-linear model for DLQI, including 54 (56.25%) patients with high initial disease burden (group A). In contrast to NRS Pain and IHS4, higher initial Hurley stages were associated with higher initial DLQI scores with Hurley II scoring 0.15 points higher and Hurley III patients scoring 0.6 points higher than those with Hurley I. The predicted values for both low and high baseline burden groups are shown in Fig. 1 (panel C). While patients in group A experienced a significant mean DLQI reduction of 4 points (54.05%) during 36 weeks of LAight therapy (β = –0.018, 95% CI: –0.024, –0.012, p < 0.001), the treatment also stabilized disease burden in patients starting with less than 6 DLQI points (n = 42, 43.75%). In line with these findings, the response rates for patients from group A gradually rise under therapy, resulting in a proportion of 48.2% at week 36 (see Fig. 2, panel C). Finally, Fig. 3 (panel C) shows the shift within the DLQI score categories for all 96 patients. At week 36, 73.0% reported a DLQI score of less than 6 points (43.8% at baseline) and, of these, 29.2% experienced “no effect” at all of HS on their quality of life (11.5% at baseline).
Safety profile
Adverse event data were available for 402 of the 786 (51.1%) analysed treatments. No side effects occurred in 337 (83.83%), 39 (9.7%) reported erythema, 19 (4.73%) reported oedema, 5 (1.24%) reported pigmentary changes, 5 (1.24%) reported crusting, and 15 (3.73%) reported other adverse events. All adverse events were localized, transient in nature and did not lead to discontinuation of treatment.
DISCUSSION
Paediatric HS is a challenging condition to manage due to the limited treatment options, which are predominantly derived from clinical practice guidelines (CPGs) developed for adult patients (1). Device-based therapy for adult HS is increasingly being used to treat active disease as well as to stabilize disease and prevent disease flares (2). Physical-procedural treatments with a good efficacy-safety profile may provide an initial, favourable therapeutic step for younger HS patients, bridging the gap to more aggressive treatment options (immunomodulators and surgery) (4).
LAight therapy is recommended by the German CPGs in combination with topical clindamycin for active HS and as monotherapy for disease stabilization (5, 6). A recent study involving a large patient cohort reported the “real-world” efficacy and safety of the LAight protocol across all severity stages of adult HS. The results demonstrated a significant reduction in IHS4, NRS Pain, and DLQI over 26 weeks of treatment, with only minor, temporary side effects observed (7).
In children and adolescents with HS, device-based treatments are still poorly studied, with 1 systematic review reporting only 81 patients treated with a variety of interventions (e.g., laser, photodynamic therapy) (8). Hence, our analysis is the largest study on paediatric HS, providing a useful insight on the efficacy and safety of this treatment approach in this special patient population.
Most notably, we found that 36 weeks of LAight treatment results in significant improvement across all evaluated endpoints in patients with initial high disease burden (group A) and successfully stabilizes the condition of those with low initial disease activity (group B). Compared with adult HS patients, the efficacy of LAight treatment in our cohort appears to be lower in terms of IHS4-55 responder rates (19.4% at week 36 vs 47.6–64.4% at week 26). The responder rates for pain and QoL improvements in our paediatric cohort show a similar trend to the clinical data in the adult HS cohort, with 40.4% pain responders vs 42.8–80.0% and 48.2% QoL responders vs 52.1–66.4%. The observed difference in efficacy of the LAight protocol between paediatric and adult patient cohorts may be attributed to differences in sample size and, most importantly, baseline disease activity as adults exhibiting higher initial IHS4 scores compared with adolescents, indicating more severe disease at the start of treatment. Furthermore, there are inherent challenges in measuring disease activity in mild HS of younger patients due to the fluctuating course of inflammatory NRS lesions (9, 10). The safety of the LAight protocol in our paediatric cohort is comparable to the adult HS study, with local, mild side effects limited to the application site (11).
At this point, it is important to emphasize that our data show a distribution of Hurley severity stages similar to that of adult cohorts, reflecting the progressive nature of the disease. Children and adolescents with HS are also at increased risk of depression and anxiety, irrespective of disease stage and activity (12, 13). Given that pain is frequently cited by patients as their primary treatment goal, we emphasize the notable shift in pain- and DLQI classifications observed in our study. Initially, a significant portion of patients reported severe pain and substantial QoL impairment. After 36 weeks of treatment, these numbers were markedly reduced, with only 2 patients reporting severe pain and a notable increase in patients experiencing little to no impact on QoL.
In conclusion, LAight therapy is a novel, gentle approach for managing paediatric HS, reporting promising preliminary efficacy and safety. Future controlled studies should further investigate its role, both as standalone treatment and in combination with conventional topical or systemic therapies.
ACKNOWLEDGEMENTS
Conflict of interest disclosures: AS: Nothing to declare. MS: grants or contracts from any entity: LENICURA GmbH – auditor activity on the implementation of the contract “AOK-Priomed Akne inversa”; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: AbbVie – honoraria for lectures; support for attending meetings and/or travel: AbbVie, Pfizer – funding of travel, congress, and hotel fees. PS: grants or contracts from any entity: Novartis; Almirall; consulting fees: AbbVie, Allergika, Almirall-Hermal, Amgen, Beiersdorf, Biocryst, BMS, Boehringer-Ingelheim, Celgene, CSL-Behring, Eli Lilly, Falk, Galderma, Hexal, Janssen, Klinge, Klosterfrau, LEO-Pharma, LETI-Pharma, L’Oréal, Novartis, Octapharma, Pfizer, Pflüger,Pharming, Regeneron, Shire, Takeda, Sanofi-Genzyme, UCBPharma; leadership or fiduciary role in other board, society, 944 REAL-WORLD EFFECTIVENESS OF LAIGHT-THERAPY IN HS committee or advocacy group, paid or unpaid unrelated to current work presented here: Society of dermopharmazie. SG: grants or contracts from any entity: Novartis, Pierre Fabre; Consulting fees: AbbVie, BMS, MSD, Genzyme, Klinge Pharma, Sun Pharma, Kyowa-Kirin, Novartis, Pierre Fabre; participation on a Data Safety Monitoring Board or Advisory Board: Alcedis; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid unrelated to current work presented here: DeCOG, German dermatological cooperative oncology group – unrelated to current work presented here. KH: CEO and stakeholder of LENICURA GmbH. JSC: Advisory Board/Consultant for AbbVie, Leo Pharma, Novartis, Pfizer, Sanofi-Genzyme, Trevi, UC,B and Vifor; speaker for AbbVie, Almirall, Janssen-Cilag, Eli Lilly, Leo Pharma, Novartis, Pfizer, Sanofi-Genzyme; investigator for AbbVie, Almirall, Amgen, AnaptysBio, BMS, Boehringer Ingelheim, Celtrion, Galderma, Galapagos, Helm AG, Kliniksa, Incyte, InfraRX, Janssen-Cilag, Leo Pharma, Medimmune, Menlo Therapeutics, Merck, Novartis, Pfizer, Regeneron, UCB, Teva, Trevi. LM: Advisory Board/Consultant for AbbVie, Novartis; speaker for AbbVie, Aristo, Leo Pharma, Medac; investigator for AbbVie, Almirall, Amgen, Anaptys-Bio, BMS, Boehringer Ingelheim, Celtrion, Galderma, Galapagos, Helm AG, Kliniksa, Incyte, InfraRX, Janssen-Cilag, Leo Pharma, Medimmune, Menlo Therapeutics, Merck, Novartis, Pfizer, Regeneron, UCB, Teva, Trevi. EvS: consulting fees: Janssen, Novartis; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Janssen, Novartis, Infectopharm, Leo; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Deutsche Dermatologische Gesellschaft, Deutsche Forschungsgemeinschaft, Mediziner Fakultätentag. UK: consulting Fees: Novartis; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Novartis; participation on a data protection monitoring board or advisory board: Novartis, EsmAiL, EpiCAi; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Deutsche Gesellschaft für Wundheilung und Wundbehandlung. HB: nothing to declare. GN: consulting fees – Dessau Medical Center received a consulting fee from Mölnlycke HealthCare GmbH, for which GN served as a consulting physician; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: speaker for the EADV HS Course 28–30 November 2022, Porto, Portugal; support for attending meetings and/or travel: Elli Lilly Scholarship for attending EADV 2021; participation in a data protection monitoring board or advisory board – Dessau Medical Center received a consulting fee from Mölnlycke Health Care GmbH, for which GN served as a consulting physician; travel grants from AbbVie. SG: nothing to declare. MP: consulting fees: AbbVie, CSL, Galderma, Novartis, Janssen Cilag, UCB; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: AbbVie, Beiersdorf, BMS, Eli Lilly, Galderma, Janssen Cilag, Leo Pharma, L’Oréal, Novartis, MSD, UCB; support for attending meetings and/or travel: AbbVie, Beiersdorf, BMS, Eli Lilly, Galderma, Janssen-Cilag, Leo Pharma, L’Oréal, Novartis, MSD, UC; participation on a Data Safety Monitoring Board or Advisory Board: AbbVie, Boehringer Ingelheim, CSL, Galderma, Janssen-Cilag, MoonLake, Novartis, L’Oréal, UCB; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: HiSNet Rhein Maine.V., President.
REFERENCES
- Cotton CH, Chen SX, Hussain SH, Lara-Corrales I, Zaenglein AL. Hidradenitis suppurativa in pediatric patients. Pediatrics 2023; 151: e2022061049. https://doi.org/10.1542/peds.2022-061049
- Lyons AB, Townsend SM, Turk D, Narla S, Baah N, Hamzavi IH. Laser and light-based treatment modalities for the management of hidradenitis suppurativa. Am J Clin Dermatol 2019; 21: 237–243. https://doi.org/10.1007/s40257-019-00491-1
- Nikolakis G, von Stebut E. Lokale und neue apparative Therapien der milden Hidradenitis suppurativa. Hautarzt 2021; 72: 676–685. https://doi.org/10.1007/s00105-021-04849-7
- Willems D, Hinzpeter EL, Van der Zee HH, Sayed CJ, Ingram JR, Beaudart C, et al. Patient preferences in the management of hidradenitis suppurativa: results of a multinational discrete choice experiment in Europe. Patient 2023; 16: 153–164. https://doi.org/10.1007/s40271-022-00614-7
- Zouboulis CC, Bechara FG, Fritz K, Goebeler M, Hetzer FH, Just E, et al. S2k Guideline for the Treatment of Hidradenitis Suppurativa/Acne Inversa – Short Version. J Dtsch Dermatol Ges 2024; 22: 868–889. https://doi.org/10.1111/ddg.15412
- Zimmer S, Basien K, von Stebut E. Einfluss der LAight-Therapie auf die Versorgung der Acne inversa. Hautarzt 2021; 72: 586–594. https://doi.org/10.1007/s00105-021-04843-z
- Strobel A, Schultheis M, Staubach P, Grabbe S, Mann C, Hennig K, et al. Real-world effectiveness and safety of the LAight-therapy in patients with hidradenitis suppurativa. J Dtsch Dermatol Ges 2024; 22: 936–945. https://doi.org/10.1111/ddg.15403
- Masson R, Parvathala N, Ma E, Shih T, Atluri S, Sayed CJ, et al. Efficacy of procedural treatments for pediatric hidradenitis suppurativa: a systematic review. Pediatr Dermatol 2023; 40: 595–605. https://doi.org/10.1111/pde.15331
- Kittler NW, Williams JC, Kudlinski MV, Lester J, Hills N, Abuabara K, et al. Evaluation of hidradenitis suppurativa diagnostic criteria in pediatric patients. JAMA Dermatol 2022; 158: 1404–1408. https://doi.org/10.1001/jamadermatol.2022.4564
- van der Zee HH, van Huijstee JC, van Straalen KR, Jemec GBE, Zouboulis CC, Tzellos T, et al. Viewpoint on the evaluation of severity and treatment effects in mild hidradenitis suppurativa: the cumulative IHS4. Dermatology 2024; 240: 514–516. https://doi.org/10.1159/000535867
- Wilden S, Friis M, Tuettenberg A, Staubach-Renz P, Wegner J, Grabbe S, et al. Combined treatment of hidradenitis suppurativa with intense pulsed light (IPL) and radiofrequency (RF). J Dermatolog Treat 2021; 32: 530–537. https://doi.org/10.1080/09546634.2019.1677842
- Cohn E, Mastacouris N, Palma G, Strunk A, Garg A. New-onset anxiety in paediatric patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2024; 38: e926–e928. https://doi.org/10.1111/jdv.19994
- Paller AS, Rangel SM, Chamlin SL, Hajek A, Phan S, Hogeling M, et al. Stigmatization and mental health impact of chronic pediatric skin disorders. JAMA Dermatol 2024; 160: 621–630. https://doi.org/10.1001/jamadermatol.2024.0594