SHORT COMMUNICATION
Pitting Oedema in Morbihan Disease: An Overlooked Feature?
Hannah KAISER1 and Jesper ELBERLING1,2
1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Gentofte Hospitalsvej 15, DK-2900 Hellerup, Denmark, and 2Department of Clinical Medicine, University of Copenhagen, Medicine, Copenhagen. E-mail: lilian.hannah.kaiser@regionh.dk
Citation: Acta Derm Venereol 2025; 105: adv43599. DOI: https://doi.org/10.2340/actadv.v105.43599.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 11, 2025; Accepted after revision: Apr 25, 2025; Published: May 27, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Morbihan disease, also known as Morbihan syndrome, is a rare cutaneous condition associated with rosacea and characterized by erythema and oedematous swelling of the upper face, particularly the periorbital region, including the eyelids. The name, Morbihan disease, originates from the first documented case in 1957 who came from the Morbihan region in north-western France (1). While Morbihan disease can present without other classical features of rosacea, patients typically do not report symptoms such as pruritus or pain. Notably, most cases described in the literature feature non-pitting oedema in the periorbital region (2). In this case report, we present a patient diagnosed with Morbihan disease exhibiting clear signs of pitting oedema in the periorbital region, a finding that contrasts with previous descriptions.
A 75-year-old Caucasian man presented with 6 months’ history of bilateral periorbital oedema worsening in the mornings, without pruritus, pain, or skin rash. He had no history of skin diseases including classical rosacea. Initial treatment steps, including discontinuation of statins, ezetimibe, and losartan, and treatment with steroid and antihistamine eyedrops, systemic corticosteroids, spironolactone, and tranexamic acid yielded no improvement.
Physical examination showed bilateral pale moderate pitting oedema of the upper and lower eyelids (Fig. 1). Laboratory tests were normal, and CT angiography revealed no venous obstruction. A biopsy revealed pronounced oedema with perifolliculitis and inflammation with some plasma cells and increased mast cells, consistent with Morbihan disease. Treatment with 1 g/day tetracycline led to significant improvement within 4 weeks and complete resolution after 3 months.
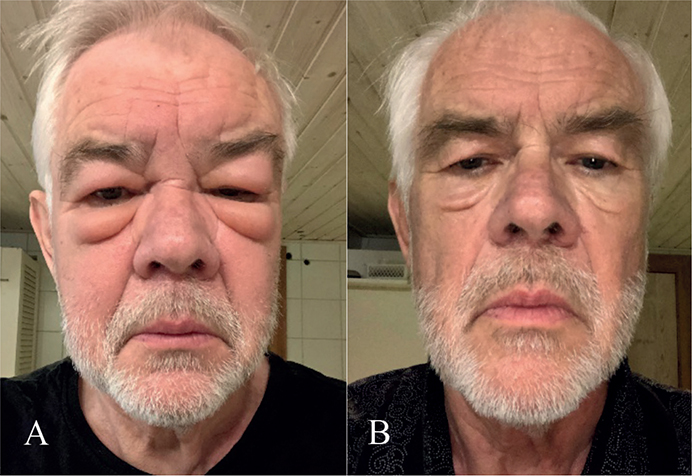
Fig. 1. Features (A) before and (B) after tetracycline. The patient has given permission for publication.
DISCUSSION
Morbihan disease is characterized by impaired lymphatic vessels permeability, leading to insufficient lymph drainage and fluid accumulation in affected skin. While the exact aetiology remains unknown, proposed mechanisms include chronic inflammation from underlying conditions such as rosacea that impact the tissue surrounding the dermal lymphatic vessels, as well as obstruction of the lymphatic vessels by granulomas and immune cells such as histiocytes (3, 4).
The condition typically manifests in individuals in their mid-50s, with male predominance (2). Although considered a rare form of rosacea, it is likely underrecognized, and its true prevalence is unknown. The disease shares some clinical features with angioedema and other facial conditions, contributing to diagnostic delay. Biopsy is often necessary to differentiate the disease (5). A recent study observed that these patients suffer from the disease for an average of 923 days before they are diagnosed (2). To date, there are mostly case reports, and larger observational studies examining clinical and histopathological characteristics are warranted, especially as many authors report difficulties in successfully treating the disease (1, 2, 6). Moreover, there are no guidelines for standard treatment of the disease with tetracycline antibiotics and isotretinoin, with variable success and frequent recurrence after discontinuation (2).
This case highlights a clear presentation of pitting oedema of the eyelids, an uncommon but documented feature occurring during the disease course (7). This underscores the importance of pitting oedema as a potential feature of Morbihan disease.
REFERENCES
- Yvon C, Mudhar HS, Fayers T, Siah WF, Malhotra R, Currie Z, et al. Morbihan syndrome, a UK case series. Ophthal Plast Reconstr Surg 2020; 36: 438–443. https://doi.org/10.1097/IOP.0000000000001589
- Mayur O, Martinez R, McNichol MC, McGee JS. Clinical and histological features and treatment outcomes of patients with Morbihan disease: a systematic review. Arch Dermatol 2023; 315: 2427–2429. https://doi.org/10.1007/s00403-023-02621-6
- Wohlrab J, Lueftl M, Marsch WC. Persistent erythema and edema of the midthird and upper aspect of the face (morbus morbihan): evidence of hidden immunologic contact urticaria and impaired lymphatic drainage. J Am Acad Dermatol 2005 52: 595–602. https://doi.org/10.1016/j.jaad.2004.08.061
- Nagasaka T, Koyama T, Matsumura K, Chen KR. Persistent lymphoedema in Morbihan disease: formation of perilymphatic epithelioid cell granulomas as a possible pathogenesis. Clin Exp Dermatol 2008; 33: 764–767. https://doi.org/10.1111/j.1365-2230.2008.02892.x
- Donthi D, Nenow J, Samia A, Phillips C, Papalas J, Prenshaw K. Morbihan disease: a diagnostic dilemma: two cases with successful resolution. SAGE Open Med Case Reports 2021; 9: 10–13. https://doi.org/10.1177/2050313X211023655
- Cabral F, Lubbe LC, Nóbrega MM, Obadia DL, Souto R, Gripp AC. Morbihan disease: a therapeutic challenge. An Bras Dermatol 2017; 92: 847–850. https://doi.org/10.1590/abd1806-4841.20174485
- Smith LA, Cohen DE. Successful long-term use of oral isotretinoin for the management of Morbihan disease: a case series report and review of the literature. Arch Dermatol 2012; 148: 1395–1398. https://doi.org/10.1001/archdermatol.2012.3109