RESEARCH LETTER
Baricitinib 2 mg/day as a Cost-conscious Entry Point to Systemic Therapy in Moderate-to-severe Atopic Dermatitis: Real-world Data from a Japanese Clinic

1Rifu Dermatology Allergy Clinic, Miyagi, Japan, and 2Tohoku University Graduate School of Medicine, Department of Dermatology, Sendai, Japan. E-mail: mizuashi@derma.med.tohoku.ac.jp
Citation: Acta Derm Venereol 2025; 105: adv43616. DOI: https://doi.org/10.2340/actadv.v105.43616.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 13, 2025; Accepted after revision: Aug 19, 2025. Published: Sep 10, 2025.
To the Editor,
Pruritus is the most burdensome symptom of atopic dermatitis (AD), affecting over 85% of patients daily and severely impairing quality of life (QOL) (1). Although Janus kinase (JAK) inhibitors, including baricitinib, reduce pruritus by targeting interleukin-31 and other type 2 cytokines, baricitinib 2 mg/day has shown only modest efficacy in prior post-hoc analyses, raising concerns about its standalone utility (2, 3). However, in Japan and other countries with limited reimbursement, the high cost of biologics and JAK inhibitors remains a significant barrier to systemic therapy (4–7). In the United States, for example, the 5-year budget impact of initiating dupilumab has been estimated at $22,348 per treated patient (6). In response, several countries have implemented cost-containment measures, such as drug price regulation and cost-effectiveness evaluation (4–7). Nevertheless, Japan’s national high-cost medical reimbursement programme often fails to fully mitigate out-of-pocket burdens, particularly among working-age adults.
To address these clinical and financial barriers, our clinic adopted a cost-conscious strategy offering baricitinib 2 mg/day as an accessible entry point to systemic therapy for JAK inhibitor-naïve patients with moderate-to-severe AD and severe pruritus.
This retrospective study included 46 Japanese patients (mean age 37.1 years; range 12–78; 34 females) treated with baricitinib 2 mg/day between October 2023 and February 2025. All patients were JAK inhibitor-naïve and met the inclusion criteria of the baseline Itch Numerical Rating Scale (NRS) ≥ 7 and Eczema Area and Severity Index (EASI) ≥ 16. Two patients had previously discontinued biologics due to dissatisfaction with their delayed onset of action (see Table SI). We evaluated Itch NRS, EASI, and Atopic Dermatitis Control Tool (ADCT) scores before and 1–2 weeks after treatment initiation, along with data on treatment duration, switching, and adverse events (Tables SI and SII).
All 46 patients demonstrated reductions in Itch NRS scores ranging from 2 to 10 points within 1–2 weeks, with most reporting relief within hours of the first dose (p < 0.001; Fig. 1A). A ≥4-point reduction was observed in 93% of patients, far exceeding the 15.1% response rate reported in previous post-hoc analyses after 2 weeks of treatment with baricitinib 2 mg/day (3). Parallel improvements were noted in ADCT subdomains related to itch and sleep disturbance (see Tables SI and SII). In addition, EASI scores decreased within 1–2 weeks except in one case (p < 0.001; Fig. 1B), mainly due to reduced erythema and excoriations, while nodules and lichenification improved after more than 1 month.
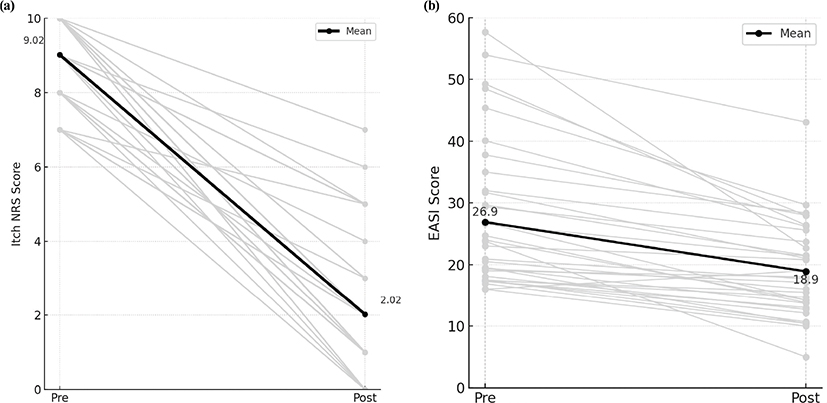
Fig. 1. (A) Itch Numerical Rating Scale (NRS) scores before and after 1–2 weeks of baricitinib 2 mg/day treatment. (B) Eczema Area and Severity Index (EASI) scores before and after 1–2 weeks of baricitinib 2 mg/day treatment.
On analysis, 21 patients (46%) continued baricitinib either intermittently or long-term. Paediatric patients often transitioned to biologics due to long-term safety considerations, while some adults switched to alternative JAK inhibitors seeking greater efficacy (see Table SII). Treatment was discontinued in 4 patients due to mild, transient adverse events (dizziness, fatigue), all of which resolved after cessation. Three patients developed acne, which was manageable with topical agents. Temporary interruptions due to influenza or COVID-19 were well tolerated and without clinical consequence (see Table SII).
Several patients who had initially declined systemic therapy for financial reasons perceived baricitinib 2 mg/day as both effective and affordable. Patients who had previously failed to achieve control with antihistamines and potent topical corticosteroids expressed a willingness to resume baricitinib during flares, even without full insurance coverage. These findings emphasize the treatment’s real-world accessibility and acceptability in socioeconomically constrained settings.
Cost-effectiveness is a critical factor in shared decision-making for AD management. A recent review by Heinz et al. (7) ranked baricitinib as the second most cost-effective systemic agent after dupilumab, having been deemed cost-effective in all available analyses. Additionally, a head-to-head comparison by Liu et al. (8) reported comparable long-term efficacy between baricitinib 2 mg/day and dupilumab, with faster early itch relief in the baricitinib group. Furthermore, patients with ≥ 50% BSA involvement or body weight ≥ 60 kg (mean: 70.7 kg) showed no marked deviation in Itch NRS reduction compared with the overall population in our clinic (Figs S1 and S2). Although less potent than its 4 mg counterpart, the 2 mg/day dose may provide an optimal balance of efficacy, affordability, and tolerability.
To our knowledge, this study represents the second real-world analysis of baricitinib 2 mg/day in moderate-to-severe AD, with the first having been reported by Liu et al. (8). While limited by its retrospective design and modest sample size, the consistent early symptomatic improvement in this cohort supports its utility as an initial systemic option. In countries lacking flat pricing systems or robust subsidy frameworks – such as Japan, the United States, and parts of Asia – this low-dose regimen may help bridge the access gap in systemic AD care.
ACKNOWLEDGEMENTS
IRB approval status: This study was approved by the institutional review board and ethics committee of the Medical Corporation Kōjinkai. The study was conducted in accordance with the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences, 2002), ICH Guidelines for Good Clinical Practice, and Declaration of Helsinki. As this study was retrospective and did not involve personally identifiable data, such as clinical photographs, an opt-out document was posted at the clinic from January to March 2025.
REFERENCES
- Simpson EL, Bieber T, Eckert L, Wu R, Ardeleanu M, Graham NMH, et al. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol 2016; 74: 491–498. https://doi.org/10.1016/j.jaad.2015.10.043
- Simpson E, Armstrong A, Boguniewicz M, Fuxench ZCC, Feely M, Pierce E, et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: long-term efficacy and patient-reported outcomes. Dermatol Ther 2022; 35: e15954. https://doi.org/10.1111/dth.15954
- Silverberg JI, Boguniewicz M, Waibel J, Weisman J, Strowd L, Sun L, et al. Clinical tailoring of baricitinib 2 mg in atopic dermatitis: baseline body surface area and rapid onset of action identifies response at week 16. Dermatol Ther 2022; 12: 137–148. https://doi.org/10.1007/s13555-021-00640-7
- Pourali SP, Nscuti L, Dusetzina SB. Out-of-pocket costs of specialty medications for psoriasis and psoriatic arthritis treatment in the Medicare population. JAMA Dermatol 2021; 157: 1239–1241. https://doi.org/10.1001/jamadermatol.2021.3616
- Schaefer CP, Cappelleri JC, Cheng R, Cole JC, Guenthner S, Fowler J, et al. Health care resource use, productivity, and costs among patients with moderate to severe plaque psoriasis in the United States. J Am Acad Dermatol 2015; 73: 585–593. https://doi.org/10.1016/j.jaad.2015.06.049
- Feldman SR, Cox LS, Strowd LC, Gerber RA, Faulkner S, Sierka D, et al. The challenge of managing atopic dermatitis in the United States. Am Health Drug Benefits 2019; 12: 83–93.
- Heinz KC, Beaudart C, Willems D, Wiethoff I, Hiligsmann M. Cost-effectiveness of emerging treatments for atopic dermatitis: a systematic review. PharmacoEcon 2023; 41: 1415–1435. https://doi.org/10.1007/s40273-023-01293-4
- Liu B, Song X, Liao S, Luan T, Zhao Z. Comparison of efficacy of baricitinib and dupilumab in the treatment of Chinese moderate-to severe atopic dermatitis: a retrospective study. Int Arch Allergy Immunol 2023; 184: 966–974. https://doi.org/10.1159/000530394