ORIGINAL REPORT
Time to Disease Control with Dupilumab for Bullous Pemphigoid: A Systematic Review and Meta-analysis
Laurence MAINVILLE1-3 , Lily XU4, Vincent PIGUET1,2, Aaron M. DRUCKER1,2# and David O. CROITORU1,2,5#
, Lily XU4, Vincent PIGUET1,2, Aaron M. DRUCKER1,2# and David O. CROITORU1,2,5#
1Division of Dermatology, Department of Medicine, University of Toronto, Toronto, 2Division of Dermatology, Department of Medicine, Women’s College Hospital, Toronto, 3Division of Dermatology, Department of Medicine, CHU de Québec-Université Laval, Québec, 4Toronto, Ontario, and 5Division of Dermatology, Department of Medicine, University Health Network, Toronto, Ontario, Canada
#These authors contributed equally.
Abstract
Bullous pemphigoid (BP) is a chronic autoimmune blistering disease primarily affecting the elderly population. While awaiting the results from randomized clinical trials to assess the effect of dupilumab in patients with BP, clinicians have begun to introduce dupilumab into their therapeutic arsenal, with few data supporting their clinical decisions. The objectives were to assess time to disease control, predictors of response, achievement of disease control, disease recurrence, and occurrence of adverse events. Randomized and non-randomized studies of interventions (NRSIs) from Medline and Embase were reviewed. A total of 315 studies were identified and 5 NRSIs (167 participants with moderate-to-severe BP) meeting our inclusion criteria were found. Dupilumab was significantly associated with shorter time to disease control compared with the control group (HR 2.71 [95% CI, 1.85–3.96; I2 = 35%; 127 participants; 4 studies]). The overall strength of the evidence was graded as very low due to serious risk of bias and imprecision of effect measures. There were insufficient data to inform conclusions regarding BP recurrence and adverse events. Evidence was found that dupilumab reduces time to disease control in BP. It was not possible to assess predictors of response using pre-planned meta-regression. Randomized controlled trials are needed to determine dupilumab’s place in therapeutic algorithms for BP.
PROSPERO number: CRD42024599235
SIGNIFICANCE
Dupilumab is an injectable medication known to reduce the severity of Th2-driven diseases such as atopic dermatitis. While awaiting for the final results from a randomized clinical trial (LIBERTY-BP ADEPT) assessing the effect of dupilumab in bullous pemphigoid, clinicians have begun to introduce dupilumab into their therapeutic arsenal, with few data supporting their clinical decisions. Using pooled data from previous comparative studies, we found evidence that dupilumab reduces time to disease control in bullous pemphigoid compared with control (hazard ratio 2.71 [95% CI, 1.85–3.96; I2 = 35%; 127 participants; 4 studies; very low quality of the evidence]).
Key words: skin diseases; vesiculobullous; bullous pemphigoid; alpha subunit of interleukin-4 receptor; meta-analysis.
Citation: Acta Derm Venereol 2025; 105: adv43667. DOI: https://doi.org/10.2340/actadv.v105.43667.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 20, 2025. Accepted after revision: May 13, 2025. Published: May 27, 2025.
Corr: Laurence Mainville, MD, MSc, FRCPC, 76 Greenville St, Toronto, Ontario, Canada, M5S 1B2. E-mail: Laurence.mainville.1@ulaval.ca
Competing interests and funding: VP has received grants from AbbVie, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Incyte, Janssen, LEO Pharma, L’Oréal, Novartis, Organon, Pfizer, Sandoz, and Sanofi; received payment or honoraria for speaking engagement from Sanofi; participated on an advisory board for LEO Pharma, Novartis, Sanofi, Union Therapeutics, AbbVie, and UCB; and received equipment donation from L’Oréal. AMD has received compensation from the British Journal of Dermatology (reviewer and editor), American Academy of Dermatology (guidelines writer), Canadian Dermatology Today (manuscript writer), and National Eczema Association (consultant) and Canada’s Drug Agency (consultant). AMD has received research grants to his institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes for Health Research, US National Institutes of Health, and Physicians Services Incorporated Foundation. DOC has worked as a consultant for UCB, Bausch, Novartis, AbbVie, and Sanofi.
INTRODUCTION
Bullous pemphigoid (BP) is a chronic autoimmune blistering disease targeting specific subepithelial antigens BP180 and BP230 (1). Persson et al. estimated the cumulative incidence of BP over a 1-year period at 8.2 (95% 4.8 to 13.7) per 1,000,000 people (2). As demonstrated by Teraki et al. (3), skin-homing T-cells are responsible for the synthesis of interleukin-4 and interleukin-13 found in the peripheral blood and skin blisters of BP patients.
Dupilumab is a monoclonal antibody targeting interleukin-4 receptor alpha, thereby inhibiting signalling of interleukin-4/13, and reducing the severity of Th2-driven diseases (4). It was first approved for the treatment of atopic dermatitis by the US Food and Drug Administration in April 2017, and by Health Canada in November 2017. In 2018, Kaye et al. published the first case report of BP treated with dupilumab: after 12 weeks of treatment, an 80-year-old male achieved complete clinical (resolution of blisters) and biologic response (undetectable BP180 and BP230) (5). The first multicentre randomized clinical trial to assess the effect of dupilumab in BP patients is currently underway (LIBERTY-BP ADEPT) (6, 7). While awaiting the final results of that definitive trial, clinicians have begun to introduce dupilumab into their therapeutic arsenal for BP, with few data supporting their clinical decisions, including patient selection. To aggregate and synthesize the available data for all patients with bullous pemphigoid treated with dupilumab, we performed a systematic review and meta-analysis of randomized and non-randomized studies of interventions (NSRIs) to assess: (1) time to disease control and predictors of response, and (2) achievement of disease control, disease recurrence, and occurrence of adverse events.
Methods
The study protocol followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) recommendations (8). The protocol was pre-registered CRD42024599235. The methodology complies with the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5, 2024) (9). This report follows the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement and recommendations for meta-analysis of observational studies (10, 11).
Eligibility criteria
Explicit study design features were chosen to decide which types of non-randomized studies of interventions (NRSIs) should be included in this systematic review (12). Justifications to include NRSIs included the lack of randomized trials and the need to inform the design of future studies. Included NRSIs needed to assess, prospectively or retrospectively, the effect of dupilumab in comparison with placebo, no treatment, standard of care, or any other neutral or not very active treatment. The diagnosis of bullous pemphigoid had to be confirmed by histology and direct immunofluorescence +/– detection of autoantibodies (BP180, BP230) by enzyme-linked immunosorbent assay (ELISA). Studies were included without restriction based on age, BP subtype, doses, indication, and duration of dupilumab treatment. There was no restriction based on the language of publication.
Research sources and strategies
The literature search was conducted using Medline and Embase databases from their inception until 10 October 2024 (Table SI). Bibliographies of included studies and previous reviews on the subject were screened for studies that met our eligibility criteria. We used online translator software for eligible studies published in languages other than French or English.
Review of studies
Two independent reviewers (LM and LX) screened the titles and abstracts of citations regarding their population, intervention, and study design. The full texts of screened citations were searched by the same reviewers to retain those that met eligibility criteria. These steps were carried out using Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia). Disagreements were resolved by consensus or by consulting senior investigators (AD and DC).
Study data
Data extraction was done independently in duplicate by 2 reviewers (LM and LX) using a standardized collection form. Authors were contacted up to twice in the event of missing information related to the primary endpoint. Collected data documented the following items:
- Studies’ features and data on risk of bias (study design label, retrospective or prospective, language of publication, country of origin, number of study centre(s), sponsorship, duration);
- Population in individual studies (inclusion and exclusion criteria, recruitment methods, total number of participants, number of participants per group, baseline differences between groups, withdrawals and exclusions);
- Intervention group (co-intervention(s), intervention description, number of participants, duration, administration);
- Control group (control description, number of participants, duration);
- Outcomes of interest (time to disease control, number of participants with disease control and number of participants with disease recurrence, number of grade 3+ adverse events [13]);
- Planned explanatory variables regarding patients (sex, age, comorbidities [neurological disease, neoplasia]), disease’s characteristics (bullous pemphigoid subtype [bullous or non-bullous], mucosal involvement, acral involvement, disease duration, disease severity scores at baseline (Bullous Pemphigoid Disease Area Index [BPDAI], Numerical rating scale [NRS] to evaluate pruritus, body surface area [BSA]), baseline indirect immunofluorescence titres, IgE, and eosinophil levels.
Measures and prioritization
The primary endpoint was time to disease control. Secondary outcomes were achievement of disease control, disease recurrence, and occurrence of adverse events. The definitions used were those of the authors, and if not specified, disease control was defined as “the time at which new lesions cease to form and established lesions begin to heal” (14).
Risk of bias
Risk of bias for each study was independently assessed by 2 reviewers (LX and LM) using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool (15). The risk of bias was judged low, moderate, serious, or “no information”. The sources of funding for each study and their potential influence were assessed. We planned to assess the presence of publication bias with funnel plots.
Data synthesis
Methods from Wan et al. and Hozo et al. were used to transform median to mean values when required to present descriptive data (16, 17). We planned to express time to disease control using hazard ratios (HR), with 95% CI (time-to-event data). Summary time-to-event data were incorporated into the meta-analysis using methods from Tierney et al. (18). Achievement of disease control, disease recurrence, and occurrence of adverse events (dichotomous data) were expressed using odds ratio (OR), with 95% CI. A forest plot was created for each endpoint.
We planned to conduct a meta-analysis using random-effects models if there were at least 3 included studies for each outcome. The analyses were completed using Review Manager (RevMan, version 5.4.1, the Cochrane Collaboration). Weighting of studies was achieved using the inverse variance method (dichotomous variables) and the DerSimonian and Laird method (time-to-event data) (19). Statistical heterogeneity between studies was verified with the I2 test, based on the Cochrane Q (20). Subgroup analyses were planned a priori to explain heterogeneity, if present. They focused on: (1) co-interventions (absence or presence), and (2) risk of bias (low, moderate, serious, or “no information”). We planned to conduct a meta-regression to identify covariates with potential modifier effect on time to disease control (if > 10 included studies).
Certainty of evidence assessment
We used the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) to assess the certainty of the evidence (21, 22).
Results
We identified 315 studies from electronic and hand-searches. We included 5 NRSIs with a total of 167 participants (range 24 to 40) with moderate-to-severe BP (Table I and Fig. 1). Publication year ranged from 2021 to 2023. The mean age of patients ranged from 61 to 75 years. One of the 5 included studies was multicentre, the rest were single centre (4). All included studies were cohort studies conducted in China and published in the English language. Four of 5 studies were conducted retrospectively (4, 23–25). One of the studies did not declare receiving funding (24), and 4/5 were supported by public or academic grants (4, 23, 25, 26).
| Trial | Total (n), Dupi:Ctrl | BPDAI scorea Dupi:Ctrl | Dupilumab | Co-intervention | Control | Methylprednisolone (median cumulative dose) Dupi:Control | Topical steroid (n) | Follow-up duration |
| Zhang 2021 (25) | 8:16 | 34 (19–75): 36 (21–71) |
- Week 0: 600 mg s/c - Week 2: 300 mg s/c q 2 weeks - Until minimal dose of steroidb |
Methylprednisolone 0.6 mg/kg/day* and azathioprine 2 mg/kg/day - Tapered from day 14 post disease controlb |
Same as co-intervention | 1.9 g:2.3 g | Yesd (if relapse; n = 4) |
32 weeks |
| Yang 2022 (23) | 20:20 | 38 ± 12: 40 ± 10 |
- Week 0: 600 mg s/c - Week 2: 300 mg s/c every other week |
Methylprednisolone (< 0.4 mg/kg/day) or equivalent* | Methylprednisolone c - Moderate disease: 0.4 mg/kg/day - Extensive disease: 0.6–0.8 mg/kg/day |
0.4 g:1.0 g | Yes (n = 40) |
12 weeks |
| Huang 2023 (26) | 16:20 | 51 (45–57): 57 (46–62) |
- Week 0: 600 mg s/c; - Week 2: 300 mg s/c every other week |
Methylprednisolonec - Week 0: 0.4 to 0.8 mg/kg/day - Tapered from day 14 post disease control down to 0 mg/day |
Methylprednisolonec - Week 0: 0.4 to 0.8 mg/kg/day - Tapered from day 14 post disease control down to < 0.08 mg/kg/day |
No information | No | 52 weeksà |
| Qi 2023 (24) | 9:18e | 53 ± 13: 56 ± 12 |
- Week 0: 600 mg s/c - Week 2: 300 mg s/c q 2 weeks - Tapering based on disease control |
IV Methylprednisolone - Week 0: 40 mg/day - Week 1: 40 mg/dayc - Disease controlled: Tapered to 10 mg/day (maintenance) |
IV Methylprednisolone - Week 0: 40 mg/day - Week 1: 60 mg/dayc - Week 2: adjuvant therapy added (IVIG [n = 2], CsA [n = 1], AZA [n = 1], Doxycycline+thalidomide [n = 1]) - Disease controlled: Tapered to 16 mg/day (maintenance) |
2.7 g:4.1 g | Yes (if relapse; n = 5) |
12 weeksf |
| Yan 2023 (4) | 12+8:20g | 121 ± 22: 139 ± 6 |
- Week 0: 600 mg s/c to no loading dose - Week 1: 300 to 600 mg q 1-4 weeks for 1-10 injections |
Methylprednisolonec or prednisolone - Week 0: 0.05 to 2 mg/kg |
Methylprednisolonec or prednisolone - Week 0: 0.2mg/kg to 1mg/kg - Tapered by 2.5–10 mg q 1–8 weeks |
1.8 gh:2.8 g | No | 24 weeks |
| AZA: azathioprine; CsA: cyclosporine A; IVIG: intravenous immune globulin; IV: intravenous; q: repeat every; Mg: milligram; s/c: subcutaneous. aBullous pemphigoid disease activity score (BPDAI), presented as median (range), or mean ± standard deviation. Definition of disease severity: mild < 15; moderate 15–34; severe > 34. bMedian duration of treatment was: 4 months and 121.5 days (dupilumab and methylprednisolone, respectively; treatment group); 148.5 days (methylprednisolone; control group). cRoute of administration not specified. dTopical steroids used in patients who relapsed during the study period (dupilumab group, n = 1; control group, n = 3), along with increased methylprednisolone to the previous level. eStudy results reported with discrepancy between text (9:18) and Kaplan–Meier curves (8:19). We used results based on the Kaplan–Meier curves. fFollow-up duration after disease control was achieved. gIntervention group (n = 20) included 12 participants treated with dupilumab alone, and 8 participants with dupilumab and systemic steroids. hExcluding patients treated with dupilumab alone. |
||||||||
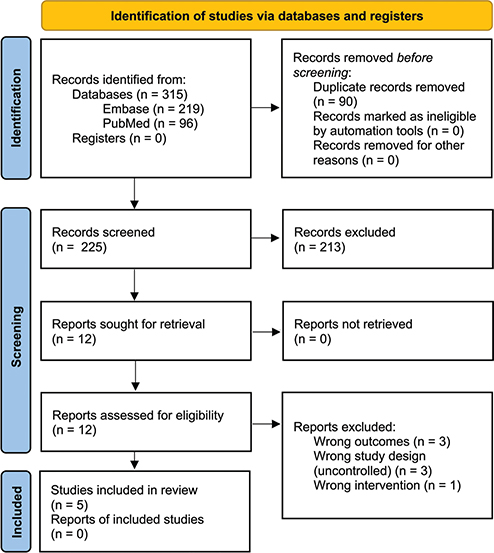
Fig. 1. PRISMA 2020 flow diagram.
Dupilumab was administered with ≥ 1 co-intervention (systemic steroid +/– azathioprine, high-potency topical steroid) in all included studies, except for 12 participants within a multi-arm study who were administered dupilumab as monotherapy (4). Participants allocated to control groups received ≥ 1 active comparator, all considered standard care for bullous pemphigoid (systemic steroid (4, 23–26), azathioprine (24, 25), cyclosporine (24), intravenous immune globulins (24), thalidomide and doxycycline (24), and high-potency topical steroid (23–25).
Primary outcome
Dupilumab was significantly associated with shorter time to disease control compared with control (HR 2.71 [95% CI, 1.85–3.96; I2 = 35%; 127 participants; 4 studies]; Fig. 2). One of the 5 included studies reports absolute number of participants achieving disease control without time-to-event data; it could therefore not be included in the pooled effect measure for time to disease control (4).

Fig. 2. Forest plot: time to disease control.
Fig. 3 illustrates pooled Kaplan–Meier curves comparing time to disease control between groups. Median (Q1–Q3) time to disease control (days) in dupilumab vs control groups is 9.5 (6.8–14.0) vs 14.0 (10.5–19.0), respectively. Mean time to disease control (days) ± SD in dupilumab vs control groups is 10.6 ± 6.1 vs 14.9 ± 6.1, respectively.
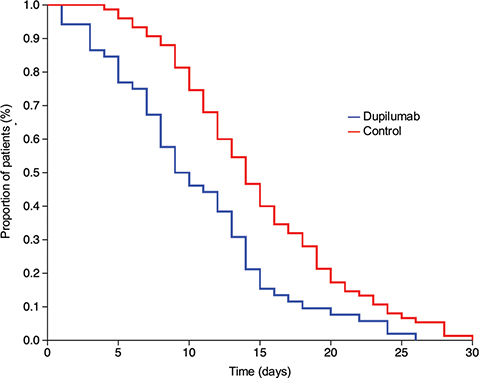
Fig. 3. Pooled Kaplan–Meier curves: time to disease control.
Three studies were judged at moderate risk of bias and 1/4 at serious risk of bias: none provided information on methods used to control for confounding (ROBINS-I, domain 1); outcome measures could have been influenced by the knowledge of the intervention received, given unblinded assessors and retrospective designs in 3/4 studies (ROBINS-I, domain 2 and 6). In 1/4 study, the choice of intervention was decided with the patient’s intention and physician’s experience; the choice of intervention could have been influenced by the knowledge or risk of the outcome (ROBINS-I, domain 3) (23). The overall strength of the evidence was graded as very low due to serious risk of bias, and imprecision (Table II).
| No. of studies (no. of participants) | Quality assessment | Summary of findings | ||||||
| Risk of bias | Consistency | Directness | Precision | Publication bias | Relative effect (95% CI) | Absolute effect (95% CI) | Quality (GRADE) | |
| Time to disease control: 4 (109) |
Seriousa (–2) |
No important inconsistencyb | Direct | Imprecisionc (–1) |
Not estimabled | Hazard ratio = 2.71 (1.85 to 3.96) |
Median survival time = –8.83 days (–10.47 to –6.43)e |
⊕⊖⊖⊖, very low |
| Recurrence: 3 (87) |
Moderateb (–1) |
No inconsistency | Direct | Imprecisionc (–1) |
Not estimabled | Odds ratio = 0.47 (0.14 to 1.62) |
Risk difference = 0.13 (–0.21 to 0.20)f |
⊕⊕⊖⊖, low |
| Adverse events: 3 (104) |
Seriousg (–2) |
No inconsistency | Direct | Imprecisionc (–1) |
Not estimabled | Odds ratio = 0.41 (0.11 to 1.51) |
Risk difference = 0.09 (–0.10 to 0.13)f |
⊕⊖⊖⊖, very low |
| aSerious risk of bias limitations. Studies (3/4) were conducted retrospectively; the selection of participants was based on patients’ characteristics observed after the start of intervention (bias in selection of participants). In 1 study, the intervention was decided based on patient’s intention and physician’s experience; classification of intervention status could have been affected by knowledge or risk of the outcome (bias in classification of interventions). In 1 study, adjunct immunosuppressive therapy was added in control group participants with uncontrolled disease at week 2 (unbalanced deviation from intended intervention). In 4/4 studies, outcome assessors were unblinded (bias in measurement of outcomes). bModerate risk of bias limitations. Studies (2/3) were conducted retrospectively; the selection of participants was based on patients’ characteristics observed after the start of intervention (bias in selection of participants). In 1 study, adjuvant immunosuppressive therapy was added in control group participants with uncontrolled disease at week 2 (unbalanced deviation from intended intervention). In 3/3 studies, outcome assessors were unblinded (bias in measurement of outcomes). cImprecision observed from 95% confidence intervals > 0.25. dPublication bias not estimable considering insufficient number of studies (< 10 studies). eAbsolute difference in median event-free time calculated as per Tierney et al. 2007 (18). fAssumed comparator risk (ACR) calculated from median comparator group risk across studies. gSerious risk of bias limitations. Studies (3/3) were conducted retrospectively; the selection of participants was based on patients’ characteristics observed after the start of intervention (bias in selection of participants). In 1 study, the intervention was decided based on patient’s intention and physician’s experience; classification of intervention status could have been affected by knowledge or risk of the outcome (bias in classification of interventions). In 3/3 studies, outcome assessors were unblinded (bias in measurement of outcomes). | ||||||||
We observed moderate heterogeneity between studies evaluating time to disease control (global I2 = 35%). It could best be explained by subgroup analyses based on risk of bias (I2 for subgroup differences = 51.1%). In moderate risk of bias studies, the hazard ratio for time to disease control was 3.35 (95% IC, 2.08–5.41; I2 = 21%; 87 patients; 3 NRSIs); in 1 study with serious concerns, the hazard ratio was 1.89 (95% IC, 1.02–3.52; I2 = not applicable; 40 patients; 1 NRSI). Publication bias and subgroup analysis based on the presence of co-intervention could not be assessed. Covariates with potential modifier effect on time to disease control could not be identified using meta-regression considering the low number of included studies.
Secondary outcomes
Disease control. We were not able to evaluate the achievement of disease control (dichotomous data) due to insufficient number of studies (OR 1.50 [95% CI, 0.43–5.25]; I2 = not applicable; 40 patients; 1 NRSI). Forest plot for achievement of disease control is presented in the Supplementary data (Fig. S1).
Disease recurrence. Based on data from 3 studies (24–26), disease recurrence was less common with dupilumab compared with controls, but the effect estimate was imprecise and overlapped the null (OR 0.47 [95% CI, 0.14–1.62]; I2 = 0%; 87 patients; 3 NRSIs). Forest plot for disease recurrence is presented in the Supplementary data (Fig. S2). Two of 3 studies had unblinded retrospective designs, and assessors could have been influenced by the knowledge of the intervention (ROBINS-I, domains 2 and 6). In one study (24), immunosuppressive therapy was added to uncontrolled BP participants within the control group only, leading to unbalanced deviation from intended intervention (ROBINS-I, domain 4). Publication bias could not be assessed. The overall strength of the evidence was graded as low due to moderate risk of bias, and imprecision (see Table II). Subgroup analyses could not be conducted based on risk of bias and co-intervention.
Adverse events. Patients in the dupilumab group were at lesser risk of experiencing grade 3+ adverse events compared with those in the control group, but the effect estimate was imprecise and overlapped the null (OR 0.41 [95% CI, 0.11–1.51]; I2 = 0%; 104 patients; 3 NRSIs) (4, 23, 25). Two of 5 studies reported no events in both arms, and were excluded from the meta-analysis as per standard practice. Forest plot for adverse events is presented in Fig. S3. Included studies (3/3) were conducted retrospectively by unblinded assessors who could have been influenced by knowledge of the intervention (ROBINS-I, domains 2 and 6). In 1/3 studies (23), the choice of intervention could have been influenced by knowledge or risk of the outcome (ROBINS-I, domain 3) (23). Publication bias could not be assessed. The overall strength of the evidence was graded as very low considering serious risk of bias and imprecision (see Table II). Subgroup analyses could not be conducted based on risk of bias and co-intervention.
DISCUSSION
In this systematic review and meta-analysis of NRSIs, dupilumab was associated with a significant reduction in time to disease control in patients with moderate-to-severe BP compared with heterogeneous controls, including placebo and standard of care. There were insufficient data to inform conclusions regarding BP recurrence and adverse events.
A recent Cochrane review of interventions in bullous pemphigoid found limited evidence to support the use of dupilumab, citing case reports and cohort studies (25, 27, 28). European guidelines endorse the management of BP with dupilumab based on case reports (29–31). In a recent systematic review from Ye et al., dupilumab led to complete remission in 66.7% of patients with BP (n = 96) (32). Their methods included uncontrolled retrospective studies and case reports, more likely prone to potential bias compared with controlled studies. Cao et al. conducted a systemic review evaluating the effect of 3 advanced therapies (dupilumab, rituximab, and omalizumab) in the treatment of BP. They did not proceed to quantitative analysis of the results, and they did not extract time-to-event data. Using descriptive methods, their results included an average time to remission of 4.5 months (range 1.0–15.0 months) with dupilumab, with 2/36 (5.6%) patients experiencing recurrence of BP (33). Velin et al. published in 2023 a meta-analysis of biological agents for the treatment of bullous pemphigoid. Their pooled effect measure to assess dupilumab efficacy was derived from subgroup analyses and should consequently be interpreted with caution (RR 1.19 [95% CI, 0.89–1.61]) (34). In June 2020, Murrell et al. initiated a phase 2/3 multicentre placebo-controlled RCT evaluating the efficacy of dupilumab in bullous pemphigoid (LIBERTY-BP ADEPT) (6). A press release issued in September 2024 by the industry sponsor announced promising results, including statistically significant improvement of disease remission at 36 weeks in the dupilumab arm vs placebo (20% vs 4%, respectively; p = 0.0114) (35). While awaiting the results from this RCT, we present the highest level of evidence available to support the use of dupilumab in the treatment of BP.
Strengths and limitations
The strengths of this study include our use of pooled data from survival analysis on time to disease control. We used a peer-reviewed search strategy without restriction for language or year of publication to include all potentially eligible studies. Limitations include overall very low quality of the evidence due to the risk of bias inherent to unblinded retrospective trials, imprecision of the effect measures for secondary outcomes, and a single country of origin for all included studies, which may limit generalizability of data to global populations. The heterogeneity of co-interventions and control groups makes interpretation of the results more challenging.
Conclusion
In conclusion, we found evidence that dupilumab reduces time to disease control in bullous pemphigoid. We were unable to assess predictors of response using meta-regression as planned, so further evidence is needed to guide appropriate patient selection for this novel therapy. Further randomized controlled trials are needed to determine dupilumab’s role in therapeutic algorithms for bullous pemphigoid.
ACKNOWLEDGEMENTS
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Montagnon CM, Tolkachjov SN, Murrell DF, Camilleri MJ, Lehman JS. Subepithelial autoimmune blistering dermatoses: clinical features and diagnosis. J Am Acad Dermatol 2021; 85: 1–14. https://doi.org.com/10.1016/j.jaad.2020.11.076
- Persson MSM, Begum N, Grainge MJ, Harman KE, Grindlay D, Gran S. The global incidence of bullous pemphigoid: a systematic review and meta-analysis. Br J Dermatol 2022; 186: 414–425. https://doi.org.com/10.1111/bjd.20743
- Teraki Y, Hotta T, Shiohara T. Skin-homing interleukin-4 and -13-producing cells contribute to bullous pemphigoid: remission of disease is associated with increased frequency of interleukin-10-producing cells. J Invest Dermatol 2001; 117: 1097–1102. https://doi.org.com/10.1046/j.0022-202x.2001.01505.x
- Yan T, Xie Y, Liu Y, Shan Y, Wu X, Wang J, et al. Dupilumab effectively and rapidly treats bullous pemphigoid by inhibiting the activities of multiple cell types. Front Immunol 2023; 14: 1194088. https://doi.org.com/10.3389/fimmu.2023.1194088
- Kaye A, Gordon SC, Deverapalli SC, Her MJ, Rosmarin D. Dupilumab for the treatment of recalcitrant bullous pemphigoid. JAMA Dermatol 2018; 154: 1225–1226. https://doi.org.com/10.1001/jamadermatol.2018.2526
- Murrell DF, Joly P, Werth VP, Ujiie H, Worm M, Mangold AR, et al. Study design of a phase 2/3 randomized controlled trial of dupilumab in adults with bullous pemphigoid: LIBERTY-BP ADEPT. Adv Ther 2024; 41: 2991–3002. https://doi.org.com/10.1007/s12325-024-02810-3
- Dupixent late-breaking positive pivotal data in bullous pemphigoid presented at AAD [press release]. Paris and Tarrytown, NY, March 8, 2025.
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4: 1. https://doi.org.com/10.1186/2046-4053-4-1
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
- Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000; 283: 2008–2012. https://doi.org.com/10.1001/jama.283.15.2008
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 2009; 62: 1006–1012. https://doi.org.com/10.1016/j.jclinepi.2009.06.005
- Higgins JP, Ramsay C, Reeves BC, Deeks JJ, Shea B, Valentine JC, et al. Issues relating to study design and risk of bias when including non-randomized studies in systematic reviews on the effects of interventions. Res Synth Methods 2013; 4: 12–25. https://doi.org.com/10.1002/jrsm.1056
- Institute NC. Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. 2017. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf
- Murrell DF, Daniel BS, Joly P, Borradori L, Amagai M, Hashimoto T, et al. Definitions and outcome measures for bullous pemphigoid: recommendations by an international panel of experts. J Am Acad Dermatol 2012; 66: 479–485. https://doi.org.com/10.1016/j.jaad.2011.06.032
- Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355: i4919. https://doi.org.com/10.1136/bmj.i4919
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014; 14: 135. https://doi.org.com/10.1186/1471-2288-14-135
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005; 5: 13. https://doi.org.com/10.1186/1471-2288-5-13
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007; 8: 16. https://doi.org.com/10.1186/1745-6215-8-16
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7: 177–188. https://doi.org.com/10.1016/0197-2456(86)90046-2
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539–1558. https://doi.org.com/10.1002/sim.1186
- Atkins D, Briss PA, Eccles M, Flottorp S, Guyatt GH, Harbour RT, et al. Systems for grading the quality of evidence and the strength of recommendations II: pilot study of a new system. BMC Health Serv Res 2005; 5: 25. https://doi.org.com/10.1186/1472-6963-5-25
- Iorio A, Spencer FA, Falavigna M, Alba C, Lang E, Burnand B, et al. Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ 2015; 350: h870. https://doi.org.com/10.1136/bmj.h870
- Yang J, Gao H, Zhang Z, Tang C, Chen Z, Wang L, et al. Dupilumab combined with low-dose systemic steroid therapy improves efficacy and safety for bullous pemphigoid. Dermatol Ther 2022; 35: e15648. https://doi.org.com/10.1111/dth.15648
- Qi W, Rushan X. The efficacy and safety of dupilumab combined with methylprednisolone in the treatment of bullous pemphigoid in China. Int Immunopharmacol 2023; 118: 110050. https://doi.org.com/10.1016/j.intimp.2023.110050
- Zhang Y, Xu Q, Chen L, Chen J, Zhang J, Zou Y, et al. Efficacy and safety of dupilumab in moderate-to-severe bullous pemphigoid. Front Immunol 2021; 12: 738907. https://doi.org.com/10.3389/fimmu.2021.738907
- Huang D, Zhang Y, Yu Y, Jiang Y, Kong L, Ding Y, et al. Long-term efficacy and safety of dupilumab for severe bullous pemphigoid: a prospective cohort study. Int Immunopharmacol 2023; 125(Pt A): 111157. https://doi.org.com/10.1016/j.intimp.2023.111157
- Singh S, Kirtschig G, Anchan VN, Chi CC, Taghipour K, Boyle RJ, et al. Interventions for bullous pemphigoid. Cochrane Database Syst Rev 2023; 8: CD002292. https://doi.org.com/10.1002/14651858.CD002292.pub4
- Liang J, Abulikemu K, Maolidan, Hu F, Zhao J, Qiu Y, et al. Nine cases of refractory bullous pemphigoid treated with dupilumab and literature review. Int Immunopharmacol 2023; 116: 109788. https://doi.org.com/10.1016/j.intimp.2023.109788
- Seyed Jafari SM, Feldmeyer L, Bossart S, Simon D, Schlapbach C, Borradori L. Case report: combination of omalizumab and dupilumab for recalcitrant bullous pemphigoid. Front Immunol 2020; 11: 611549. https://doi.org.com/10.3389/fimmu.2020.611549
- Abdat R, Waldman RA, de Bedout V, Czernik A, McLeod M, King B, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol 2020; 83: 46–52. https://doi.org.com/10.1016/j.jaad.2020.01.089
- Borradori L, Van Beek N, Feliciani C, Tedbirt B, Antiga E, Bergman R, et al. Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 2022; 36: 1689–1704. https://doi.org.com/10.1111/jdv.18220
- Ye S, Ling G, Chen M. A Systematic evaluation of dupilumab for bullous pemphigoid treatment. Dermatologic Therapy 2024; 2024: 1171779. https://doi.org/10.1155/2024/1171779
- Cao P, Xu W, Zhang L. Rituximab, omalizumab, and dupilumab treatment outcomes in bullous pemphigoid: a systematic review. Front Immunol 2022; 13: 928621. https://doi.org.com/10.3389/fimmu.2022.928621
- Velin M, Dugourd PM, Sanchez A, Bahadoran P, Montaudie H, Passeron T. Efficacy and safety of methotrexate, omalizumab and dupilumab for bullous pemphigoid in patients resistant or contraindicated to oral steroids: a monocentric real-life study. J Eur Acad Dermatol Venereol 2022; 36: e539–e42. https://doi.org.com/10.1111/jdv.17999
- Dupixent is the first and only biologic to achieve significant improvements in disease remission and symptoms in bullous pemphigoid positive pivotal study [press release]. Paris and Tarrytown, NY, Sept 11, 2024.