ORIGINAL REPORT
Adverse Events and Immune Response in Psoriasis Patients Receiving Interleukin-17 Inhibitors
Christopher Willy SCHWARZ1,2  , Charlotte NÄSLUND-KOCH1 , Claus ZACHARIAE1,2 , Jakob Benedict SEIDELIN2,3 , Susanne Dam NIELSEN2,4 , Sisse Rye OSTROWSKI2,5, Karen Marie THYSSEN ASTVAD6 , Inger BROCK7, Lars IVERSEN8 , Mads Kirchheiner RASMUSSEN8 , Nikolai LOFT1 , and Lone SKOV1,2
, Charlotte NÄSLUND-KOCH1 , Claus ZACHARIAE1,2 , Jakob Benedict SEIDELIN2,3 , Susanne Dam NIELSEN2,4 , Sisse Rye OSTROWSKI2,5, Karen Marie THYSSEN ASTVAD6 , Inger BROCK7, Lars IVERSEN8 , Mads Kirchheiner RASMUSSEN8 , Nikolai LOFT1 , and Lone SKOV1,2
1Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte, Copenhagen, 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, 3Department of Digestive Diseases, Copenhagen University Hospital – Rigshospitalet, Copenhagen, 4Department of Infectious Diseases, Copenhagen University Hospital – Rigshospitalet, Copenhagen, 5Department of Clinical Immunology, Copenhagen University Hospital – Rigshospitalet, Copenhagen, 6Unit of Mycology, Statens Serum Institut, Copenhagen, 7Department of Clinical Microbiology, Copenhagen University Hospital – Herlev and Gentofte, Copenhagen, and 8Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
Interleukin-17 inhibitors are effective in psoriasis; however, they are associated with an increased risk of infections, particularly oral candidiasis, and new-onset/flares of inflammatory bowel disease. This study aimed to identify predictive markers for these adverse events and to describe the functional immune response in patients treated with interleukin-17 inhibitors using a whole-blood stimulation system (TruCulture®). Patients with psoriasis initiating an interleukin-17 inhibitor (n = 36) or adalimumab (n = 24) were enrolled. Patients attended visits at baseline, week 12, and week 52, during which skin and mucosal swabs, and faecal and blood samples were collected. Baseline oral Candida albicans colonization with no clinical symptoms was associated with an increased risk of oral candidiasis during the first year of interleukin-17 inhibitor therapy, with no cases of oral candidiasis observed in the adalimumab group. Gut inflammation, measured by faecal calprotectin, remained stable in both the adalimumab and interleukin-17 inhibitor group. Colonization with Staphylococcus aureus did not change during treatment. It was found that interleukin-17 inhibitors induced an anti-inflammatory state and potentially more active toll-like receptor 3-mediated antiviral responses compared with adalimumab. In conclusion, screening for oral Candida albicans colonization prior to initiation of interleukin-17 inhibitor therapy may be a useful strategy for risk stratification and early intervention.
SIGNIFICANCE
We evaluated how psoriasis treatments that block interleukin-17 affect the immune system and investigated potential markers that could help identify patients with psoriasis at risk of certain infections and gut problems when treated. We found that interleukin-17 inhibitors had a global effect on several of the cytokine levels measured beyond interleukin-17. Furthermore, patients where we were able to measure the fungus Candida albicans in the mouth prior to initiating treatment were more likely to develop oral infection during treatment. This could help physicians identify patients at higher risk of this adverse event, leading to early intervention.
Key words: adalimumab; candidiasis; immunity; inflammatory bowel diseases; interleukin-17; S100 proteins.
Citation: Acta Derm Venereol 2025; 105: adv43685. DOI: https://doi.org/10.2340/actadv.v105.43685.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 24, 2025. Accepted after revision: Jul 7, 2025. Published: Aug 18, 2025.
Corr: Christopher Willy Schwarz, Department of Dermatology and Allergy, Gentofte Hospitalsvej 15, 1st Floor, DK-2900 Hellerup, Denmark. E-mail: christopher.willy.schwarz.01@regionh.dk
Competing interests and funding: SRO, KAAS, and IB have no conflicts of interest to declare. CWS has received a travel grant from JNJ. CNK has received research funding from the Danish National Psoriasis Foundation, the LEO Foundation, the Kgl. Hofbundtmager Aage Bang Foundation, Copenhagen University Hospital – Herlev and Gentofte Hospital, Krista and Viggo Petersen’s Foundation, the Ellab Foundation, and Siemens Healthcare. She has received honoraria as speaker and travel grant from LEO Pharma. CNK has served as an investigator for Galderma, AbbVie, LEO Pharma, Novartis, and CSL Behring. CZ has been a paid speaker or consultant for UCB, LEO Pharma, AbbVie, Janssen Cilag, Novartis, Takeda, and Galderma. JS has been national coordinator for RCTs from AbbVie, Arena Pharmaceuticals, Ely Lilly, and Boehringer Ingelheim and has received research and educational grants from Takeda, J&J, Pyrinome, and AbbVie. SDN has received research and educational grants from the Novo Nordisk Foundation, the Independent Research Fund Denmark, and the Svend Andersen Fonden, has served on Advisory Boards with Gilead, Takeda, and GSK, and has received honoraria from Gilead, Takeda, and GSK. LI is also an employee at MC2 Therapeutics A/S. MKR has been a paid speaker for AbbVie, Eli Lilly, and LEO Pharma, and has been a consultant or has served on Advisory Boards with AbbVie, Janssen Cilag, Eli Lilly, UCB, Almirall, and Bristol-Myers Squibb. MKR has served as an investigator for UCB, Novartis, AbbVie, and Bristol-Myers Squibb. NL has been a paid speaker for Eli Lilly, Janssen-Cilag, and Sandoz, and has received a research grant from the LEO Foundation. LS has been a paid speaker for AbbVie, Eli Lilly, Takeda, Sanofi, Pfizer, and LEO Pharma, and has been a consultant or has served on Advisory Boards with AbbVie, Janssen Cilag, Eli Lilly, LEO Pharma, UCB, Almirall, Bristol-Myers Squibb, Takeda, Stada, and Sanofi, and has received research and educational grants from Novartis, Sanofi, Bristol-Myers Squibb, Almirall, and Janssen-Cilag.
This study received funding from the Aage Bang Foundation.
INTRODUCTION
Psoriasis is a common chronic inflammatory skin disease driven by T helper (Th)-17 cells. Moderate-to-severe cases are often treated with biologics targeting cytokines in this pathway. Interleukin-17 (IL-17) is one of the main drivers of the disease, and four IL-17 inhibitors (IL-17i) are currently approved for treating moderate-to-severe psoriasis (secukinumab, ixekizumab, brodalumab, and bimekizumab).
IL-17i are among the biologics with the highest efficacy while also demonstrating an overall good safety profile (1). However, as with other biologics used to treat psoriasis, upper respiratory tract infections are common (2). IL-17i may also specifically impair immunity against cutaneous Staphylococcus aureus (S. aureus) and Candida albicans in the oral mucosa and cause flares of inflammatory bowel diseases (IBD). Indeed, IL-17 appear to promote recruitment of neutrophils, which has been shown to be important for host defence against S. aureus and some Gram-negative bacteria such as Klebsiella pneumoniae and Bordetella pertussis (3, 4). Furthermore, patients with rare inborn mutations in the IL-17RA and IL-17F gene have impaired mucocutaneous immunity to Candida albicans (5). Consistent with this, oral candidiasis has frequently been reported in clinical trials of IL-17i, particularly bimekizumab, with 19.3% developing oral candidiasis in a phase III clinical trial (2, 6). IL-17 does not appear to be as important for immunity against vulvovaginal candidiasis. Instead, it is thought that vulvovaginal candidiasis is caused by neutrophil dysfunction (7). Indeed, the incidence of genital candidiasis is much lower than that of oral candidiasis in clinical trials of IL-17i (2). Furthermore, IL-17 is important for immunity against other fungi such as Malassezia and dermatophytes (8).
Upstream inhibition of the Th17 pathway with IL-12/23p40 and IL-23p19 inhibitors is effective in both psoriasis and IBD (9); however, patients had no improvement and some experienced worsening of Crohn’s disease in phase II trials of secukinumab and brodalumab (10, 11). New-onset IBD has also been observed in psoriasis trials of IL-17i (12). This contradictory finding has been explained by the importance of IL-17A for intestinal barrier integrity. In contrast, inhibition of upstream IL-23 does not affect IL-17A production from innate lymphocytes. The activation of pathogenic Th17 cells is also inhibited by blocking IL-23 (13).
While the risk of cutaneous S. aureus infection, oral candidiasis, and new-onset/flare of IBD appears to be directly related to the specific inhibition of IL-17, secondary effects on the immune system are likely. For example, reduced IL-10 has been reported in psoriasis patients treated with IL-17i who experienced Candida infections during therapy (14). Investigating the overall effect on the immune system of specific IL-17 inhibition may help explain why the overall infection risk appears to be unchanged in patients treated with IL-17i versus adalimumab (15). Adalimumab functions by inhibiting tumour necrosis factor (TNF) and is associated with an increased risk of infections including reactivation of latent tuberculosis. However, the immunological mechanisms are not fully understood (16, 17). Adalimumab is commonly used as first-line biologic therapy for patients with psoriasis in Denmark. It therefore serves as a relevant reference when evaluating differences in the safety profile of biologics used to treat psoriasis.
Identifying patients at risk of adverse events is crucial, as it allows for implementation of preventive measures or selection of biologics targeting alternative pathways. This study aimed to identify markers that predict an increased risk of cutaneous S. aureus infections, oral candidiasis, or IBD in psoriasis patients treated with IL-17i versus those treated with adalimumab, while also assessing the impact of IL-17i on the functional immune response.
MATERIALS AND METHODS
This cohort study was conducted in accordance with the Declaration of Helsinki and was approved by the Danish Data Protection Agency (P-2021-363) and a scientific ethics committee for the Capital Region of Denmark (H-21022377). All included patients gave written informed consent and did not receive any compensation. The study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cohort studies (18).
Setting and patients
We recruited patients with plaque-type psoriasis from the outpatient clinic at the Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte between March 2022 and March 2024. Eligible participants were patients with psoriasis initiating an IL-17i without prior exposure to any IL-17i and, as controls, patients initiating treatment with adalimumab. Patients were excluded if they were pregnant, breast-feeding, or under 18 years of age.
Measurements and outcomes
Patients enrolled in the study attended visits at baseline (treatment initiation), week 12, and week 52 in conjunction with regular outpatient visits. At each visit, enrolled patients were asked about adverse events and a fixed set of gastrointestinal questions, some of which were adapted from the Harvey-Bradshaw index for Crohn’s disease (Table SI). At each visit, we also collected skin and mucosal swabs (eSwab Collection and Transport System, Copan Italia, Brescia, Italy), and faecal and blood samples.
A detailed description of the analyses of the collected samples is provided in Appendix S1.
In short, oral mucosal and perianal skin swabs were collected to identify Candida species colonization. Swabs were collected from the nasal vestibule, retroauricular skin, umbilicus, and perineum to identify S. aureus colonization. Of note, we updated the study protocol mid-study, therefore we collected samples for S. aureus colonization only from a subset of patients. Colonization was defined as being culture positive without having clinical symptoms. Oral candidiasis was diagnosed clinically without culture confirmation.
Faecal samples were tested for faecal calprotectin (FCP) and used as a surrogate marker of gut inflammation (19). We used a method with a reference change value of 150%, meaning that variation between samples below this threshold may be due to test variation. An FCP ≥ 50 µg/g was considered elevated.
Blood was transferred to TruCulture® tubes to mimic the immune response to various stimuli. In each tube, concentrations of TNF-α, interferon (IFN)-α, IFN-γ, IL-1β, IL-6, IL-8, IL-10, IL-12p40, and IL-17A were measured.
Statistical methods
The association between oral Candida colonization and oral candidiasis the first year was tested using Fisher’s exact test. Cytokine concentrations measured by the TruCulture® assay at baseline and at week 12 were compared using the Wilcoxon signed-rank test. P-values < 0.05 were considered significant. R statistical software version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria) was used for data analysis (20).
RESULTS
A total of 58 patients were included in the study. Two patients never started treatment and four patients initially enrolled in the adalimumab group and, after failing treatment, were subsequently enrolled in the IL-17i group. Thus, the study population comprised 56 patients and 60 treatment series, 24 in the adalimumab group and 36 in the IL-17i group (18 ixekizumab and 18 bimekizumab). Baseline characteristics are presented in Table I and responses to fixed questions at each visit are summarized in Table SI. None of the patients had a family history of IBD.
In the adalimumab group, 21 (87.5%) had a 12-week visit and 16 (66.7%) had a 52-week visit. In the IL-17i group, 30 (83.3%) had a 12-week visit and 24 (66.7%) had a 52-week visit. Reasons for dropout were primary ineffectiveness (n = 5), adverse events (n = 3), paused treatment (n = 2), administrative loss (n = 1), withdrawal of consent (n = 4), and missed follow-up (n = 5).
Colonization with Candida species
At baseline, 9/24 (37.5%) in the adalimumab group and 13/36 (36.1%) in the IL-17i group were colonized with Candida species in the oral cavity. None in the adalimumab group developed oral candidiasis during the first year of treatment. In the IL-17i group, 6/36 (16.7%) developed oral candidiasis: 2/23 (8.7%) of non-colonized and 4/13 (30.8%) of colonized patients (Table II). However, this was not statistically significant (p-value: 0.16). Patients who developed oral candidiasis in the colonized group were all colonized with Candida albicans at baseline, while none colonized with Candida glabrata (n = 2) or Candida dubliniensis (n = 1) developed oral candidiasis. Thus, when restricting the analysis to patients colonized with Candida albicans at baseline, 4/10 (40%) developed oral candidiasis, which was statistically significant from the non-Candida albicans colonized group at baseline where 2/26 (7.7%) developed oral candidiasis (p-value = 0.04). As previously mentioned, oral candidiasis was diagnosed clinically without culture confirmation and none led to treatment discontinuation.
| Group | Colonized at 12 weeks | Colonized at 52 weeks | Oral candidiasis |
| Adalimumab group | |||
| Not colonized at baseline | 3/13 (23.1) | 2/10 (20.0) | 0/15 (0.0) |
| Colonized at baseline | 8/8 (100.0) | 3/6 (50.0) | 0/9 (0.0) |
| IL-17i group | |||
| Not colonized at baseline | 5/18 (27.8) | 6/14 (42.9) | 2/23 (8.7) |
| Colonized at baseline | 7/11 (63.6) | 5/10 (50.0) | 4/13 (30.8)a |
| aAll 4 cases were colonized with Candida albicans at baseline. In total, 10 were colonized with Candida albicans at baseline, meaning 40% (4/10) of the patients colonized at baseline developed oral candidiasis. This table shows the prevalence of oral Candida colonization at baseline. Data are presented as no. (%) of patients with positive colonization at week 12 or week 52 or oral candidiasis in the first year. |
|||
Table II indicates the association between oral colonization at baseline and colonization at follow-up visits. Colonization status varied between visits, with many patients switching between being culture positive and negative during follow-ups (Table II). Because only 1/33 were colonized with Candida species on the perianal skin, we did not proceed with further analysis.
Colonization with S. aureus
At baseline, 5/12 (41.7%) in the adalimumab group and 8/15 (53.3%) in the IL-17i group were colonized with S. aureus at any of the 4 body sites (nasal vestibule, retroauricular skin, umbilicus, and perineum). We did not observe any cases of infection suspected to be caused by S. aureus. Table SII shows the association between baseline S. aureus colonization and colonization at follow-up visits. S. aureus colonization was highly variable between visits and colonization was assessed in a very limited number of patients.
Subclinical gut inflammation
In the adalimumab group, 8/21 (38.1%) sent a faecal sample at both baseline and week 12, while 7/16 (43.8%) provided a faecal sample at both baseline and week 52 (Table III). None experienced significantly increased FCP during treatment.
| Baseline → Week 12 | ||
| F-calprotectin | Adalimumab (n = 8) n (%) | IL-17 (n = 18) n (%) |
| Baseline | ||
| < 50 µg/g | 6 (75.0) | 16 (88.9) |
| ≥ 50 µg/g | 2 (25.0) | 2 (11.1) |
| Week 12 | ||
| < 50 µg/g | 8 (100.0) | 16 (88.9) |
| ≥ 50 µg/g | 0 (0.0) | 2 (11.1) |
| Change in f-calprotectina | ||
| Significant decrease | 1 (12.5) | 0 (0.0) |
| No significant change | 7 (87.5) | 17 (94.4) |
| Significant increase | 0 (0.0) | 1 (5.6) |
| Baseline → Week 52 | ||
| F-calprotectin | Adalimumab (n = 7) n (%) | IL-17 (n = 16) n (%) |
| Baseline | ||
| < 50 µg/g | 7 (100.0) | 14 (87.5) |
| ≥ 50 µg/g | 0 (0.0) | 2 (12.5) |
| Week 52 | ||
| < 50 µg/g | 7 (100.0) | 14 (87.5) |
| ≥ 50 µg/g | 0 (0.0) | 2 (12.5) |
| Change in f-calprotectina | ||
| Significant decrease | 1 (14.3) | 1 (6.3) |
| No significant change | 6 (85.7) | 14 (87.5) |
| Significant increase | 0 (0.0) | 1 (6.3) |
| aThe test has a reference change value of 150%. Thus, a significant decrease corresponds to ≤ 40% of the original value, and a significant increase corresponds to ≥ 250% of the original value. | ||
In the IL-17i group, 18/30 (60.0%) sent a faecal sample at both baseline and week 12, while 16/24 (66.7%) provided a faecal sample at both baseline and week 52 (Table III). One patient had a significant increase in FCP after 12 weeks (from < 15 µg/g to 64 µg/g), which decreased to < 15 µg/g after 52 weeks. Another patient’s FCP level increased from 66 µg/g at baseline to 398 µg/g at 52 weeks. The patient was asymptomatic and a subsequent FCP test 4 weeks later was normal (45 µg/g). In general, most patients maintained a low FCP during both treatments (< 50 µg/g).
Functional immune response
Blood samples from a subset of 11 patients were used to examine the functional innate immune response. All 11 patients initiated ixekizumab; 10 switched from adalimumab to ixekizumab, of whom 9 had no washout period and 1 had a short washout period (6 weeks). The last patient switched from ustekinumab to ixekizumab without a washout period. Absolute Psoriasis Area and Severity Index (PASI) < 4 was achieved by 8/11 (72.7%) patients at week 12.
The induced cytokine release at baseline and week 12 are visualized in Fig. 1. LPS-induced (TLR4) IFN-γ, IL-12 and IL-6 decreased, while IL-10 increased (Fig. 1A). R848-induced (TLR7/8) IL-12 and IL-6 decreased (Fig. 1B). Poly I:C-induced (TLR3) IFN-α, IL-1β, and TNF-α increased (Fig. 1C). Anti-CD3/CD28-induced (T-cell stimulation) IL-17A and IL-6 decreased (Fig. 1D). Lastly, the cytokines of the unstimulated samples did not change (Fig. 1E).
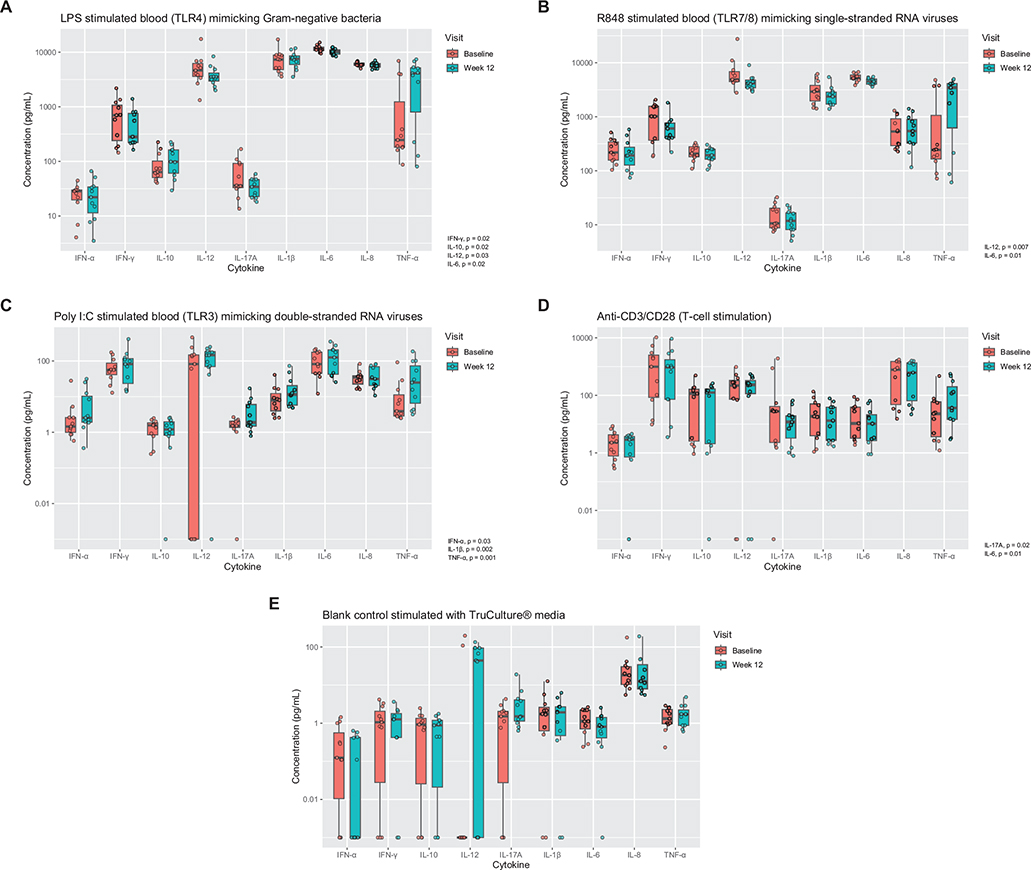
Fig. 1. Functional immune response. Box plots of induced cytokine concentrations in 11 patients treated with ixekizumab following stimulations that mimic activation of (A) toll-like receptor (TLR)4, (B) TLR7/8, (C) TLR3 as well as a tube with (D) T-cell stimulation, and (E) a blank control. Cytokine concentrations were measured before and 3 months after treatment initiation using whole-blood stimulation.
A sub-analysis conducted on the 6 patients who switched from adalimumab to ixekizumab without a washout period and with an acceptable treatment effect (absolute PASI < 4) was consistent with the main analysis.
DISCUSSION
In this clinical cohort study, we investigated markers in patients with psoriasis that may predict who is at risk of adverse events with IL-17i. We also described the effect of IL-17i on the functional immune system. Our main finding was that oral Candida albicans colonization prior to treatment initiation with IL-17i increased the risk of oral candidiasis in the first year (40.0% vs 7.7%). We also found an altered innate immune response 3 months after initiation of an IL-17i beyond the expected reduction in IL-17 levels.
Candida colonization is common in psoriasis. We found that 37% were colonized with Candida species in the oral mucosa. This is consistent with a study by Elsner et al., who found 47% of patients with psoriasis to be colonized compared with 20% of healthy controls but found no association between colonization and disease severity (21). Others have shown an association between oral candidiasis and disease severity, emphasizing the need to distinguish between colonization and infection (22). Although oral candidiasis is not life-threatening, it can cause discomfort and affect well-being, and, if associated with exacerbation of psoriasis, the identification of those patients at risk of oral candidiasis may have important clinical significance. Our study suggests that oral Candida albicans colonization, as determined by a simple oral swab, was associated with a much higher risk of oral candidiasis (40.0% vs 7.7%) in patients treated with IL-17i. This easy-to-perform test could be helpful in the clinic to help stratify biologic treatment or antifungal prophylaxis could be considered in the early stages of treatment, when the risk of oral candidiasis is highest (23). Of note, Candida albicans are diverse, and different strains exhibit varying virulence (24). Testing for specific strains could provide additional insight but would require extensive testing.
The study also investigated whether FCP, as a marker of subclinical gut inflammation, increased during IL-17i treatment as new-onset/flare of IBD is a potential IL-17i specific adverse event. Although the number of samples analysed was small, we did not find any signal to suggest that FCP increased during therapy. This result contrasts with that of an Italian study, in which 2/83 patients with psoriasis treated with IL-17i had a significant increase in FCP over 24 weeks leading to a diagnosis of ulcerative proctitis and Crohn’s disease. In the same study, no increase was seen in the 39 patients treated with IL-23i (25). Psoriasis and IBD share the IL-23/Th17 axis, and psoriasis patients have an increased prevalence of IBD (26). Therefore, it is not known whether these patients would have developed the disease even if they had not been treated with an IL-17i. Indeed, it is unclear whether IL-17i cause incident IBD, as they do not appear to confer an increased risk of incident IBD compared with placebo (27).
We investigated the functional immune response in 11 patients treated with the IL-17 inhibitor ixekizumab before and 3 months after treatment initiation using whole-blood stimulation, which has the advantage over stimulation of peripheral blood mononuclear cells (PBMCs) as it is more reproducible and better reflects the natural immune response (28). All but 1 patient switched from adalimumab to ixekizumab (the last patient switched from ustekinumab) without sufficient washout periods and, accordingly, TNF-α increased after discontinuing adalimumab. We found that IL-17A decreased after T-cell stimulation, which is consistent with the mechanism of action of ixekizumab.
A previously published study recruiting patients with psoriasis from the same department as the present study also investigated the functional immune response by TruCulture® in patients initiating adalimumab and, as expected, TNF-α decreased with all stimuli (16). We found notable differences between patients treated with adalimumab and those treated with ixekizumab, which varied depending on the specific TLR pathway activated.
Following TLR4 stimulation, the proinflammatory cytokines IL-6, IL-12, and IFN-γ decreased, whereas the anti-inflammatory cytokine IL-10 increased in the ixekizumab group, suggesting a shift towards a more anti-inflammatory state. In contrast, both the proinflammatory cytokine IL-1β and the anti-inflammatory cytokine IL-10 decreased in the adalimumab group, indicating a more generalized suppression of the innate immune system compared with ixekizumab (16).
Following TLR7/8 stimulation, IL-6 and IL-12 levels decreased in the ixekizumab group, whereas the adalimumab group showed a decrease in IL-8 and an increase in IL-1β and IL-12 (16). This suggests that adalimumab reduces acute inflammation while maintaining Th1 induction by IL-1β and IL-12, whereas ixekizumab broadly attenuates innate immune activation not only by IL-17A but also by upstream IL-12 and IL-6, which induce Th1 and Th17 differentiation, respectively (29, 30). IL-6 inhibition is ineffective in the treatment of plaque psoriasis, which has been speculated to be due to a compensatory increase in other proinflammatory cytokines (29). However, following short-term ixekizumab treatment, we found decreased IL-6 but no compensatory increase in measured proinflammatory cytokines.
The most striking difference was observed following TLR3 stimulation with poly I:C. In the ixekizumab group, IFN-α and IL-1β levels increased after initiation, whereas (non-significant) decreases in IFN-α and IFN-γ were observed in the adalimumab group (16). These results suggest that ixekizumab may enhance antiviral immunity compared with adalimumab. TLR3 recognizes double-stranded RNA viruses and therefore has the potential to recognize multiple viruses, as double-stranded RNA is an intermediate product in RNA and DNA virus replication (31). However, in the adalimumab vs ixekizumab clinical trial in psoriatic arthritis, the overall risk of (bacterial and viral) infections was numerically higher with ixekizumab (42% vs 39%) (15). In contrast, IL-17i has been associated with both a lower and higher risk of infectious disease compared with TNFi in observational studies (32, 33). No apparent difference in the overall risk of infection between IL-17i and TNFi may be explained by the fact that individuals with inborn defects of the TLR3 pathway only show increased susceptibility to herpes simplex type 1 (HSV-1) encephalitis (31). Interestingly, a previous Danish study showed a lower incidence of alphaherpesvirus infection (which includes HSV-1) in patients treated with IL-17i versus TNFi (34). Thus, IL-17i may enhance antiviral responses against HSV-1 via TLR3, potentially explaining the lower incidence of alphaherpesvirus infections observed compared with TNFi.
Our study is limited by the small sample size, and as IBD development is rare the findings on subclinical gut inflammation should be interpreted with caution. However, we found no evidence of increased subclinical gut inflammation in patients treated with IL-17i. Regarding the risk of oral candidiasis, we were limited by our reliance on a clinical diagnosis, which introduces the risk of confirmation bias, as IL-17i is known to be associated with an increased risk of oral candidiasis. Nevertheless, our findings of a much higher risk of oral candidiasis when colonized with Candida albicans in patients treated with IL-17i are interesting and warrant further investigation. Strengths of our study include the thorough characterization of the enrolled patients, the use of a comparison group, and the prospective design.
In conclusion, we explored potential markers that could help identify patients at increased risk of adverse events during IL-17i therapy. We found that oral Candida albicans colonization prior to treatment initiation may serve as a predictor for risk of developing oral candidiasis within the first year. In addition, we observed that IL-17i induces a more anti-inflammatory state and a potentially more effective antiviral response via TLR3 compared with TNFi. However, it is important to note that the overall risk of infection does not appear to be lower with IL-17i compared with TNFi.
ACKNOWLEDGEMENTS
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
IRB approval status: This cohort study was conducted in accordance with the Declaration of Helsinki and was approved by the Danish Data Protection Agency (P-2021-363) and a scientific ethics committee for the Capital Region of Denmark (H-21022377).
REFERENCES
- Sbidian E, Chaimani A, Guelimi R, Garcia-Doval I, Hua C, Hughes C, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev 2023; 7: 6689. https://doi.org/10.1002/14651858.CD011535.pub6
- Reich K, Warren RB, Lebwohl M, Gooderham M, Strober B, Langley RG, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med 2021; 385: 142–152. https://doi.org/10.1056/NEJMoa2102383
- Cho JS, Pietras EM, Garcia NC, Ramos RI, Farzam DM, Monroe HR, et al. IL-17 is essential for host defense against cutaneous Staphylococcus aureus infection in mice. J Clin Invest 2010; 120: 1762–1773. https://doi.org/10.1172/JCI40891
- Mills KHG. IL-17 and IL-17-producing cells in protection versus pathology. Nat Rev Immunol 2023; 23: 38–54. https://doi.org/10.1038/s41577-022-00746-9
- Puel A, Cypowyj S, Bustamante J, Wright JF, Liu L, Lim HK, et al. Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin-17 immunity*. Science 2011; 332: 65–68. https://doi.org/10.1126/science.1200439
- Saunte DM, Mrowietz U, Puig L, Zachariae C. Candida infections in patients with psoriasis and psoriatic arthritis treated with interleukin-17 inhibitors and their practical management. Br J Dermatol 2017; 177: 47–62. https://doi.org/10.1111/bjd.15015
- D’Enfert C, Kaune AK, Alaban LR, Chakraborty S, Cole N, Delavy M, et al. The impact of the fungus-host-microbiota interplay upon Candida albicans infections: current knowledge and new perspectives. FEMS Microbiol Rev 2021; 45: 14. https://doi.org/10.1093/FEMSRE/FUAA060
- Sparber F, Leibundgut-Landmann S. Interleukin-17 in antifungal immunity. Pathogens 2019; 8: 54. https://doi.org/10.3390/PATHOGENS8020054
- Ferrante M, Panaccione R, Baert F, Bossuyt P, Colombel JF, Danese S, et al. Risankizumab as maintenance therapy for moderately to severely active Crohn’s disease: results from the multicentre, randomised, double-blind, placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial. Lancet 2022; 399: 2031–2046. https://doi.org/10.1016/S0140-6736(22)00466-4
- Hueber W, Sands BE, Lewitzky S, Vandemeulebroecke M, Reinisch W, Higgins PDR, et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double-blind placebo-controlled trial. Gut 2012; 61: 1693–1700. https://doi.org/10.1136/gutjnl-2011-301668
- Targan SR, Feagan B, Vermeire S, Panaccione R, Melmed GY, Landers C, et al. A randomized, double-blind, placebo-controlled phase 2 study of brodalumab in patients with moderate-to-severe Crohn’s disease. Am J Gastroenterol 2016; 111: 1599–1607. https://doi.org/10.1038/ajg.2016.298
- Loft ND, Vaengebjerg S, Halling AS, Skov L, Egeberg A. Adverse events with IL-17 and IL-23 inhibitors for psoriasis and psoriatic arthritis: a systematic review and meta-analysis of phase III studies. J Eur Acad Dermatol Venereol 2020; 34: 1151–1160. https://doi.org/10.1111/jdv.16073
- Whibley N, Gaffen SL. Gut-busters: IL-17 ain’t afraid of no IL-23. Immunity 2015; 43: 620. https://doi.org/10.1016/j.immuni.2015.10.001
- Bruno M, Davidson L, Koenen HJPM, van den Reek JMPA, van Cranenbroek B, de Jong EMGJ, et al. Immunological effects of anti‒IL-17/12/23 therapy in patients with psoriasis complicated by candida infections. J Invest Dermatol 2022; 142: 2929–2939.e8. https://doi.org/10.1016/j.jid.2022.05.1083
- Smolen JS, Mease P, Tahir H, Schulze-Koops H, De La Torre I, Li L, et al. Multicentre, randomised, open-label, parallel-group study evaluating the efficacy and safety of ixekizumab versus adalimumab in patients with psoriatic arthritis naive to biological disease-modifying antirheumatic drug: final results by week 52. Ann Rheum Dis 2020; 79: 1310–1319. https://doi.org/10.1136/annrheumdis-2020-217372
- Todberg T, Loft N, Møller DL, Ostrowski SR, Nielsen SD, Skov L. Impact of methotrexate and adalimumab on immune function of patients with psoriasis. Dermatol Ther 2022; 35: e15284. https://doi.org/10.1111/dth.15284
- Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther 2008; 117: 244–279. https://doi.org/10.1016/j.pharmthera.2007.10.001
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370: 1453–1457. https://doi.org/10.1016/S0140-6736(07)61602-X
- Østgård RD, Deleuran BW, Dam MY, Hansen IT, Jurik AG, Glerup H. Faecal calprotectin detects subclinical bowel inflammation and may predict treatment response in spondyloarthritis. Scand J Rheumatol 2018; 47: 48–55. https://doi.org/10.1080/03009742.2017.1299216
- R Core Team (2022). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. https://www.R-project.org/
- Elsner K, Holstein J, Hilke FJ, Blumenstock G, Walker B, Schmidt S, et al. Prevalence of Candida species in psoriasis. Mycoses 2022; 65: 247–254. https://doi.org/10.1111/myc.13399
- Picciani BLS, Michalski-Santos B, Carneiro S, Sampaio AL, Avelleira JCR, Azulay DR, et al. Oral candidiasis in patients with psoriasis: correlation of oral examination and cytopathological evaluation with psoriasis disease severity and treatment. J Am Acad Dermatol 2013; 68: 986–991. https://doi.org/10.1016/j.jaad.2012.11.033
- Gordon KB, Langley RG, Warren RB, Okubo Y, Stein Gold L, Merola JF, et al. Bimekizumab safety in patients with moderate to severe plaque psoriasis: pooled results from phase 2 and phase 3 randomized clinical trials. JAMA Dermatol 2022; 158: 735–744. https://doi.org/10.1001/jamadermatol.2022.1185
- Lemberg C, de San Vicente KM, Fróis-Martins R, Altmeier S, Tran VDT, Mertens S, et al. Candida albicans commensalism in the oral mucosa is favoured by limited virulence and metabolic adaptation. PLoS Pathog 2022; 18: e1010012. https://doi.org/10.1371/journal.ppat.1010012
- Brizzi D, Rocco EV, Veronica E, Rocco A, Babino G, Buononato D, et al. evaluation of the role of faecal calprotectin in the management of psoriatic patients under treatment with biologic drugs. Biomedicines 2022; 10: 2968. https://doi.org/10.3390/biomedicines10112968
- Fu Y, Lee CH, Chi CC. Association of psoriasis with inflammatory bowel disease: a systematic review and meta-analysis. JAMA Dermatol 2018; 154: 1417–1423. https://doi.org/10.1001/jamadermatol.2018.3631
- Burisch J, Eigner W, Schreiber S, Aletaha D, Weninger W, Trauner M, et al. Risk for development of inflammatory bowel disease under inhibition of interleukin 17: a systematic review and meta-analysis. PLoS One 2020; 15: e0233781. https://doi.org/10.1371/journal.pone.0233781
- Duffy D, Rouilly V, Libri V, Hasan M, Beitz B, David M, et al. Functional analysis via standardized whole-blood stimulation systems defines the boundaries of a healthy immune response to complex stimuli. Immunity 2014; 40: 436–450. https://doi.org/10.1016/j.immuni.2014.03.002
- Blauvelt A. IL-6 differs from TNF-α: unpredicted clinical effects caused by IL-6 blockade in psoriasis. J Invest Dermatol 2017; 137: 541–542. https://doi.org/10.1016/j.jid.2016.11.022
- Grän F, Kerstan A, Serfling E, Goebeler M, Muhammad K. Current developments in the immunology of psoriasis. Yale J Biol Med 2020; 93: 97.
- Perales-Linares R, Navas-Martin S. Toll-like receptor 3 in viral pathogenesis: friend or foe? Immunology 2013; 140: 153–167. https://doi.org/10.1111/imm.12143
- Kridin K, Zirpel H, Mruwat N, Ludwig RJ, Thaci D. Evaluating the risk of infections under interleukin 23 and interleukin 17 inhibitors relative to tumour necrosis factor inhibitors: a population-based study. J Eur Acad Dermatol Venereol 2023; 37: 2319–2326. https://doi.org/10.1111/jdv.19328
- Glintborg B, Di Giuseppe D, Wallman JK, Provan SA, Nordström D, Hokkanen AM, et al. Is the risk of infection higher during treatment with secukinumab than with TNF inhibitors? An observational study from the Nordic countries. Rheumatology 2023; 62: 647–658. https://doi.org/10.1093/rheumatology/keac358
- Rezahosseini O, Liljendahl MS, Loft N, Møller DL, Harboe ZB, Rasmussen MK, et al. Incidence, risk factors, and consequences of human alphaherpesvirus infections in patients with psoriasis who initiate methotrexate or biologic agents. J Infect Dis 2022; 226: 1510–1518. https://doi.org/10.1093/infdis/jiac367