RESEARCH LETTER
Burden of Inflammatory Skin Diseases Based on GBD Data: China vs USA
Yulin ZOU1,2, Kexin LIAO1, Stephan TRAIDL3 and Timo BUHL1
1Department of Dermatology, Venereology and Allergology, University Medical Center Göttingen, Robert-Koch-Str. 40, DE-37075 Göttingen, Germany, 2Department of Dermatology, The First Affiliated Hospital of Jinzhou Medical University, Jinzhou, China, and 3Department of Dermatology and Allergy, Hannover Medical School, Hannover, Germany. E-mail: yulin.zouyulin@med.uni-goettingen.de
Citation: Acta Derm Venereol 2025; 105: adv43753. DOI: https://doi.org/10.2340/actadv.v105.43753.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: May 1, 2025. Accepted after revision: May 20, 2025. Published: Jun 4, 2025.
Competing interests and funding: TB has been a speaker/investigator/adviser for AbbVie, ALK, Almirall, AstraZeneca, Bencard, Eli Lilly, Incyte, Galderma, Janssen, Kiniksa, LEO Pharma, Novartis, R-Biopharm, Sanofi, and ThermoFisher. ST has been a speaker/investigator/adviser for AbbVie, ALK, Almirall, Eli Lilly, Incyte, Galderma, Janssen, LEO Pharma, Novartis, and Sanofi and received research grants from Sanofi and the Novartis Foundation. The other authors declare that they have no competing interests.
Yulin Zou and Kexin Liao are funded by the Chinese Scholarship Council (YZ: CSC no. 202308210137; KL: CSC no. 202308210104). Yulin Zou received funding from the Jinzhou Medical University Teacher Reserve Program. We acknowledge support by the Open Access Publication Funds of the Göttingen University.
INTRODUCTION
To the Editor,
Inflammatory skin diseases such as psoriasis and atopic dermatitis (AD) pose significant health and economic challenges (1, 2). Using Global Burden of Disease (GBD) data (3), this study examines trends in these conditions in the USA and China from 1990 to 2021, highlighting differences and similarities in prevalence, burden, and public health needs (4). The USA and China were chosen for comparison due to their distinct healthcare systems, population sizes, and socioeconomic factors, providing insights into future challenges in disease management across diverse settings.
Data from the GBD (https://vizhub.healthdata.org/gbd-results/) from 1990 to 2021 were analysed for psoriasis and AD in the USA and China. We investigated incidence, prevalence, and Disability-Adjusted Life Years (DALYs) presenting age-standardized rates (rate per 100,000 patient-years). Estimated Annual Percentage Change (EAPC) was calculated to assess trends over time. We employed the Bayesian Age–Period–Cohort (BAPC) model (5), a statistical approach leveraging age, period, and cohort effects to predict epidemiological trends, specifically predicting the incidence of psoriasis and AD by sex in the USA and China. Statistical analyses were conducted with R (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria).
From 1990 to 2021, the psoriasis burden grew significantly in China compared with moderate growth in the USA (Table I). In China, age-standardized prevalence rose from 362.04 to 474.02 per 100,000 patient-years (EAPC: 0.87%) and in the USA from 946.53 to 983.5 per 100,000 patient-years (EAPC: 0.12%). In China, DALYs increased from 31.45 to 41.23 per 100,000 patient-years (EAPC: 0.88%), while in the USA, they rose slightly from 81.44 to 83.61 per 100,000 patient-years (EAPC: 0.09%). This contrast highlights faster growth in China.
The burden of AD remained relatively stable in both China and the USA from 1990 to 2021 (see Table I). In China, age-standardized prevalence decreased slightly from 1357.93 to 1347.11 per 100,000 patient-years (EAPC: –0.03%), and from 3169.60 to 3161.54 per 100,000 patient-years in the USA (EAPC: –0.01%). In China, DALYs decreased marginally from 59.85 to 59.53 per 100,000 patient-years (EAPC: –0.02%), while in the USA, they declined from 156.71 to 136.56 per 100,000 patient-years (EAPC: –0.02%). This comparison suggests minimal changes in disease burden for both countries.
The projected trends for the next 19 years (2022–2040) were calculated by BAPC modelling for psoriasis (Fig. 1A–B) and AD (Fig. 1C–D) incidence in China and the USA. Psoriasis shows an increasing trend in China but remains stable in the USA. AD exhibits stable trends in both countries, with slightly wider uncertainty intervals over time. Interestingly, male and female sex leads to different projections in both diseases and countries, with most prominent differences for AD in China, where female rates are suspected to stay vastly the same, and male cases are projected to increase significantly.
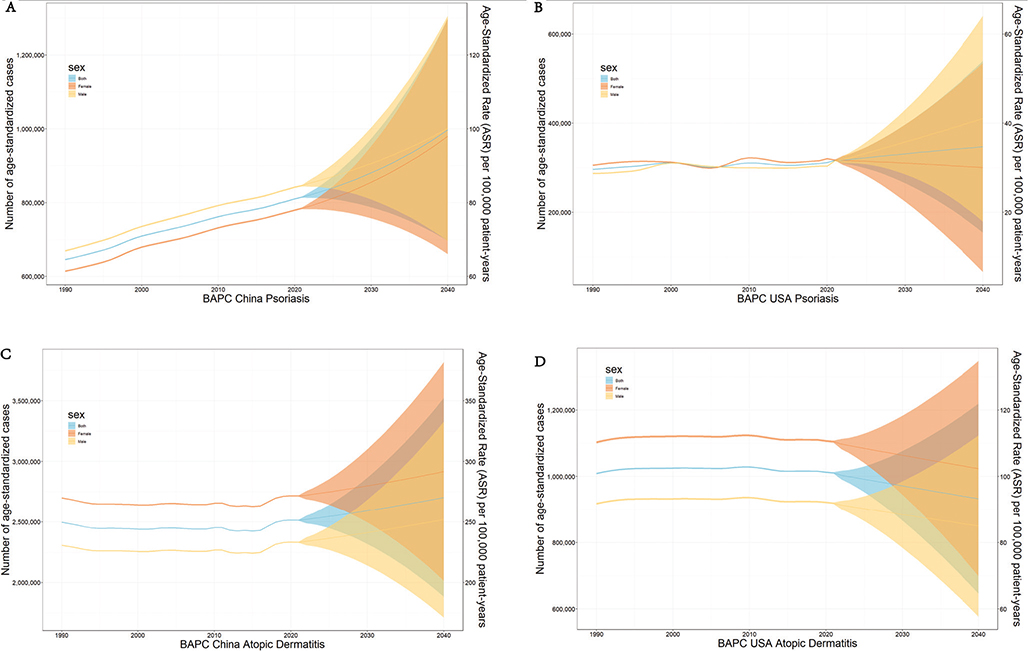
Fig. 1. Observed (1990–2021) and projected (2022–2040) trends in the burden of psoriasis and atopic dermatitis in China and the USA. Solid lines illustrate historical and forecast prevalence as age-standardized rates (per 100,000 patient-years), and shaded areas denote the 95% uncertainty intervals (UIs). Red curves correspond to female rates, yellow curves represent male rates, and blue curves depict combined rates for both sexes.
This comparative analysis highlights distinct epidemiological patterns of inflammatory skin diseases in China and the USA, offering actionable insights for global public health strategies. Efforts may focus on nationwide screening and prevention programmes to address rising prevalence and public health challenges (5). Currently, inflammatory skin diseases are not included in chronic disease subsidies in China, and pilot inclusion in such programmes could help alleviate the financial burden on patients. Expansion of chronic disease subsidies to include inflammatory skin diseases and evaluation of existing drug reimbursement policies (e.g., secukinumab, dupilumab) could alleviate patient burdens (6). In contrast, the USA’s moderate burden growth highlights the need for innovative interventions to address rising prevalence, especially in underserved populations. Globally, these findings echo broader trends of increasing inflammatory skin disease prevalence, necessitating collaborative research and policy efforts. Future efforts should prioritize equitable access to emerging treatments, robust surveillance systems, and interdisciplinary approaches to reduce disease burden worldwide.
ACKNOWLEDGEMENTS
REFERENCES
- Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet 2021; 397: 1301–1315. https://doi.org/10.1016/S0140-6736(20)32549-6
- Ständer S. Atopic dermatitis. N Engl J Med 2021; 384: 1136–1143. https://doi.org/10.1056/NEJMra2023911
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024; 403: 2133–2161. https://doi.org/10.1016/S0140-6736(24)00757-8
- Schuler CF, Billi AC, Maverakis E, Tsoi LC, Gudjonsson JE. Novel insights into atopic dermatitis. J Allergy Clin Immunol 2023; 151: 1145–1154. https://doi.org/10.1016/j.jaci.2022.10.023
- Knoll M, Furkel J, Debus J, Abdollahi A, Karch A, Stock C. An R package for an integrated evaluation of statistical approaches to cancer incidence projection. BMC Med Res Methodol 2020; 20: 257. https://doi.org/10.1186/s12874-020-01133-5
- Liu L, Lan X, Yang Y, et al. The development and application of a two-step surveillance process for Healthy China Initiative based on wide coverage interagency data. Glob Health Res Policy 2023; 8: 42. https://doi.org/10.1186/s41256-023-00326-x