SHORT COMMUNICATION
Accuracy of Optical Coherence Tomography for Subtyping Basal Cell Carcinoma: Using Histopathology of Biopsy and Entire Lesion as Reference Standard
Tom WOLSWIJK1,2, Patty J. NELEMANS3, Fieke ADAN1,2 and Klara MOSTERD1,2
1Department of Dermatology, Maastricht University Medical Center+, P. Debyelaan 25, PO Box 5800, NL-6202 AZ Maastricht, 2GROW Research Institute for Oncology and Reproduction and 3Department of Epidemiology, Maastricht University, Maastricht, The Netherlands. E-mail: tom.wolswijk@mumc.nl
Citation: Acta Derm Venereol 2023; 103: adv00889. DOI: https://doi.org/10.2340/actadv.v103.4383.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Dec 6, 2022; Published: Mar 14, 2023
INTRODUCTION
The increasing incidence of basal cell carcinoma (BCC) combined with the disadvantages of invasive diagnostic punch biopsy increase the need for non-invasive diagnostic alternatives, such as optical coherence tomography (OCT) (1, 2). OCT is a non-invasive diagnostic tool that can be used to detect and subtype BCC (Fig. 1) (3). OCT may replace punch biopsy (gold standard) only if OCT assessors can detect and subtype BCC with a high level of confidence (2). However, Sinx et al. (2) reported that subtyping BCCs using OCT remains challenging after evaluating the diagnostic accuracy of BCC subtyping using OCT. They used histopathological examination of a punch biopsy as reference standard. However, a single OCT scan always visualizes an area with a diameter of 6 mm. Hence, the question arises as to whether part of the tumor detected on OCT may be missed by punch biopsy, and thus may be misclassified as false-positive if this part contains other histopathological subtypes (4–6). This could lead to biased estimation of the diagnostic accuracy of OCT.
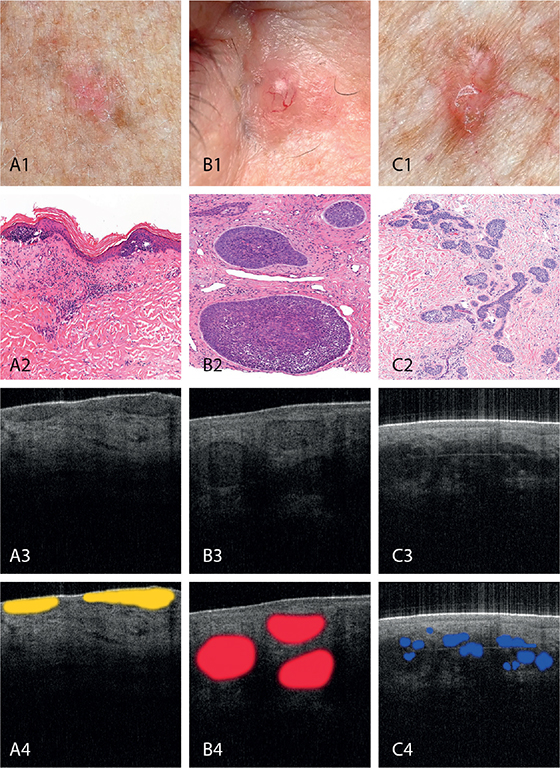
Fig. 1. Clinical (1), histopathological (2), optical coherence tomography (OCT) (3) and highlighted OCT presentation (4) of: (A) superficial, (B) nodular and (C) infiltrative basal cell carcinoma (BCC). All histopathological images have been stained by hematoxylin and eosin and are magnified 10x.
In this study, we aimed to assess the diagnostic accuracy for BCC subtyping on OCT when using two different standards of reference. Diagnostic accuracy using histopathology of a diagnostic punch biopsy as reference standard was compared to that with use of histopathology of the subsequent therapeutic excision specimen.
MATERIALS AND METHODS
Included were consecutive patients (age 18 years or older) undergoing a punch biopsy and subsequent excision for BCC. The patient’s treating physician marked the clinically most aggressive part of the tumour for punch biopsy. Subsequently, the lesion was scanned with OCT (Vivosight, Michelson Diagnostics, Kent, UK; resolution < 7.5 mm lateral, <5 mm axial; depth of focus 1.0 mm; scan area 6x6 mm²) by one expert OCT assessor. The BCC subtype was based on established morphological BCC subtype features (7, 8).
Histopathological examination of punch biopsy and excision specimen was performed by dermato-pathologists blinded to the OCT scan and OCT diagnosis made. Histopathological BCC subtypes were classified as superficial, nodular or infiltrative (9). Mixed histopathological subtypes were classified as the most aggressive subtype present (superficial BCC (sBCC) least aggressive, infiltrative BCC (iBCC) most aggressive).
The diagnostic performance of OCT in BCC subtyping was established using 2 different reference standards: (i) histopathology of the diagnostic punch biopsy (ii) histopathology of the subsequent therapeutic excision. If no residual tumour was found in the excision specimen, or if the biopsy revealed a more aggressive subtype than found in the excision specimen, we used the histopathology of the punch biopsy as the reference standard, as biopsy could have removed the most aggressive subtype. In this case biopsy is the most representative to determine the subtype.
The diagnostic performance of OCT for BCC subtyping was evaluated in cases with a high confidence BCC diagnosis. The OCT assessor was blinded to clinical and visual information about the lesion and histopathology. The diagnostic performance of OCT was expressed as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic odds ratio (DOR). Differences in diagnostic parameters were tested for statistical significance using a Chi square test for unpaired proportions. A p-value ≤0.05 was considered to indicate statistical significance.
RESULTS
The cohort comprised 131 patients with histopathologically verified BCCs (mean age 70 years, range 28–95 years). Of those, 13 cases (9.9%) were sBCC, 81 (61.8%) were nBCC and 37 (28.2%) were iBCC. In 110 cases (82.7%) the OCT assessor could determine a BCC subtype with high confidence and these cases were used for further analyses.
Among the 110 included cases, no remaining tumour was found in 17 excision specimens (15.5%) in which the subtype on the punch biopsy was considered the true subtype. By using the excision specimen as reference standard instead of the punch biopsy, 7 (6.4%) BCC subtypes were classified differently. Four BCC subtypes classified as sBCCs on punch biopsy were classified as 3 nBCCs and 1 iBCC on excision, whereas 3 BCC subtypes classified as nBCCs on punch biopsy were classified as iBCCs on excision (Table I). The ability to discriminate each BCC subtype from the other 2 subtypes on OCT scans was evaluated (Table II). Slight, but non-significant, reductions were observed in almost all diagnostic parameters, including sensitivity and specificity, when using excision specimen as the reference standard instead of punch biopsy.
DISCUSSION
The use of the excision specimen as reference standard resulted in the identification of 3 extra histopathological nBCCs and 4 extra histopathological iBCCs compared to punch biopsy. OCT (the diagnostic test under study) classified only part of these lesions correctly, and this resulted in an increased number of false-negative and false-positive results on OCT and a net decrease in sensitivity and specificity of OCT for discrimination between subtypes.
There are several explanations why more aggressive BCC subtypes are not always recognized on OCT. One case had an infiltrative subtype, but was classified as sBCC on OCT. The superficial component was clearly visible, but squamae caused shading making deeper layers of the scan difficult to analyse. Furthermore, aggressive subtypes tend to grow deeper into the dermis (10), but the resolution of OCT decreases as the penetration depth increases (11). This may also explain why the other 3 iBCCs were misclassified as nBCC on OCT.
Three cases misclassified on OCT and punch biopsy had both superficial and nodular subtypes. On OCT, the superficial component was evident. The nodular component was less evident, as the demarcation between epidermis and ovoid nests, which is an important differentiator between sBCC and nBCC, was unclear. The nodular component was also missed on punch biopsy, which could be the result of sampling error (12). The marked punch biopsy site and subsequent OCT probe placement is important, particularly in larger lesions, as the most aggressive subtype may be present outside the biopsied area. Hence, it is advisable to scan the entire lesion, which is quick and may reveal additional information on the BCC subtype.
In this study population with a low prevalence of sBCC, negative predictive value is highest when OCT is used for discrimination between sBCC and nBCC/iBCC; hence, in this population OCT has high ability to exclude sBCC in case of a diagnosis of nBCC or iBCC. The ability to exclude nBCC or iBCC in case of OCT diagnosis of another BCC subtype is lower and in this respect, there is need for improvement. Misclassification of sBCC as a more aggressive BCC will deprive patients of the choice of non-invasive treatment options. The poor ability of OCT to exclude nBCC or iBCC is of greater clinical concern, because misclassification of nBCCs and iBCCs may lead to insufficient treatment.
In conclusion, the results do not confirm the hypothesis that with respect to discrimination between BCC subtypes, the diagnostic accuracy of OCT becomes higher when using the excision specimen as reference standard instead of punch biopsy. The diagnostic parameters for OCT were even slightly lower. However, the results of this study show that bias may be limited in diagnostic studies, wherein excision specimens are not available for all patients and the use of punch biopsy as the reference standard is the only option.
REFERENCES
- Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al. Diagnosis and treatment of basal cell carcinoma: European consensus–based interdisciplinary guidelines. Eur J Cancer 2019; 118: 10–34.
- Sinx KA, van Loo E, Tonk EH, Kelleners-Smeets NW, Winnepenninckx VJ, Nelemans PJ, et al. Optical coherence tomography for noninvasive diagnosis and subtyping of basal cell carcinoma: a prospective cohort study. J Invest Dermatol 2020; 140: 1962–1967.
- Adan F, Nelemans PJ, Essers, BAB, Brinkhuizen T, Dodemont SRP, Kessels JPHM et al. Optical coherence tomography versus punch biopsy for diagnosis of basal cell carcinoma: a multicentre, randomised, non-inferiority trial. The Lancet Oncology 2022; 23: 1087–1096.
- Roozeboom M, Mosterd K, Winnepenninckx V, Nelemans P, Kelleners-Smeets N. Agreement between histological subtype on punch biopsy and surgical excision in primary basal cell carcinoma. J Eur Acad Dermatol Venereol 2013; 27: 894–898.
- Roozeboom MH, Kreukels H, Nelemans PJ, Mosterd K, Winnepenninckx VJ, Abdul Hamid MA, et al. Subtyping basal cell carcinoma by clinical diagnosis versus punch biopsy. Acta Derm Venereol 2015; 95: 997–999.
- Russell EB, Carrington PR, Smoller BR. Basal cell carcinoma: a comparison of shave biopsy versus punch biopsy techniques in subtype diagnosis. J Am Acad Dermatol 1999; 41: 69–71.
- Hussain AA, Themstrup L, Jemec GBE. Optical coherence tomography in the diagnosis of basal cell carcinoma. Arch Dermatol Res 2015; 307: 1-10.
- Fuchs C, Ortner V, Mogensen M, Rossi A, Pellacani G, Welzel J, et al. 2021 international consensus statement on optical coherence tomography for basal cell carcinoma: image characteristics, terminology and educational needs. J Eur Acad Dermatol Venereol 2022; 36: 772–778.
- Fernández-Figueras M, Malvehi J, Tschandl P, Rutten A, Rongioletti F, Requena L, et al. Position paper on a simplified histopathological classification of basal cell carcinoma: results of the European Consensus Project. J Eur Acad Dermatol Venereol 2022; 36: 351–359.
- Hendrix JD, Parlette HL. Micronodular basal cell carcinoma: a deceptive histologic subtype with frequent clinically undetected tumor extension. Arch Dermatol 1996; 132: 295–298.
- Babalola O, Mamalis A, Lev-Tov H, Jagdeo J. Optical coherence tomography (OCT) of collagen in normal skin and skin fibrosis. Arch Dermatol Res 2014; 306: 1–9.
- Mudaliar K, Speiser J, Hutchens KA. Changing dermatopathology protocols for processing small skin biopsies: decreases in slide quantity does not affect patient care and allows for optimal efficiency. Am J Dermatopathol 2016; 38: 409–412.