QUIZ SECTION
A 9-month-old Child with Diffuse Cutaneous Bullous Erythema: A Quiz
Shengyuan HUA1#, Jing CHEN2, Qiufang QIAN1#* and Jia ZHANG3,4#*
1Department of Dermatology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 2Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 3Department of Dermatology, Xinhua Hospital affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, and 4Institute of Dermatology, Shanghai Jiaotong University School of Medicine, Shanghai, China. *E-mails: qianqf@shchildren.com.cn; zhangjia@xinhuamed.com.cn
#These authors contributed equally to this work.
Citation: Acta Derm Venereol 2025; 105: adv43939. DOI: https://doi.org/10.2340/actadv.v105.43939.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Aug 21, 2025
A 9-month-old boy presented to our outpatient clinic for a recurrent diffuse cutaneous transparent bullous rash accompanied by itching 4 months earlier. Erythema with erosion formed after the blisters ruptured, and gradually became dry and scabby. On physical examination of the involuting phase, there was generalized thickening of the skin and dark, geographic erythema with erosion or scabbing was present on the trunk (Fig. 1). Vital signs were normal. There was no evidence of systemic involvement (bone marrow, spleen, liver, gastrointestinal tract, etc.). Laboratory test results, including complete blood cell count, liver and renal function tests were within the normal range.
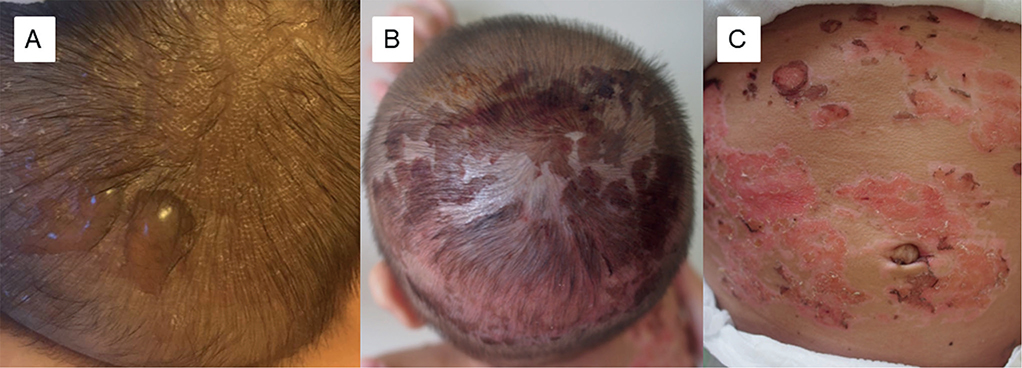
Fig. 1. Physical examination findings. (A) Bullous eruption on the scalp (acute-outbreak phase, photo from the parents. (B) Erythema, erosion, and scabbing (involuting phase) on the scalp and (C) trunk, with generalized thickened and dark skin.
What is your diagnosis?
1: Bullous diffuse cutaneous mastocytosis
2: Scalded skin
3: Toxic epidermal necrolysis (TEN)
4: Pemphigoid
See next page for answer.
ANSWERS TO QUIZ
A 9-month-old Child with Diffuse Cutaneous Bullous Erythema over Generalized Thickened and Dark Skin: A Commentary
Diagnosis: Bullous diffuse cutaneous mastocytosis
Darier’s sign was positive (after stroking the lesion, transitory reactions of erythema, and wheal formation). Skin biopsy and histopathological examination were undertaken. Haematoxylin-eosin staining showed a diffuse mononuclear cell infiltration in the upper dermis; moreover, the results of Giemsa and toluidine blue staining were positive (Fig. 2). A diagnosis of bullous diffuse cutaneous mastocytosis (DCM) was based on the presence of bullous cutaneous features, a positive Darier’s sign, and the pathological findings. After topical use of mometasone furoate cream, the lesions significantly improved. During 4-year-follow up, blister recurrence gradually subsided, leaving residual pigmentation.
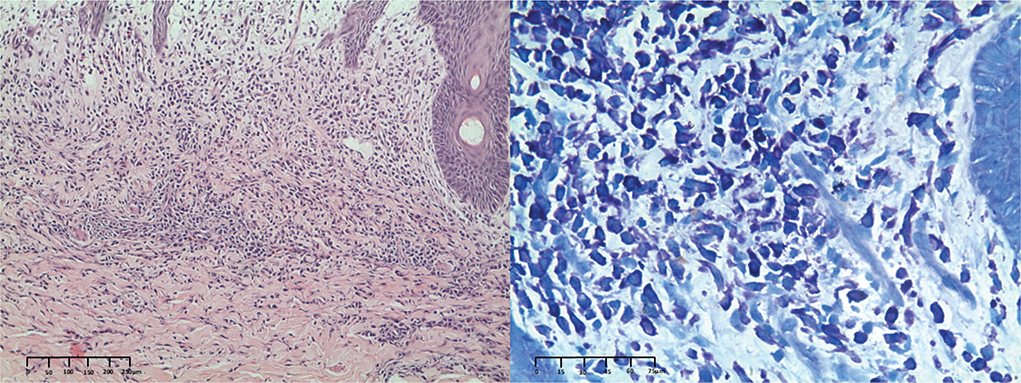
Fig 2. Haematoxylin-eosin (a,×100) and Giemsa (b,×400) staining showed mast cell infiltration and degranulation.
Mastocytosis occurs in 2 forms, cutaneous mastocytosis (CM) affecting only the skin, and systemic mastocytosis, affecting various internal organs, mainly the bone marrow and gastrointestinal tract (1). DCM is the most severe subtype of CM, applying only to patients with generalized thickened and dark skin. Infants with DCM often present initially with large blisters, generalized erythema, and pruritus. Other signs include flushing, urticaria, and a reddish-brown tinge to the skin, which appears thickened (2). Darier’s sign as an initial clue of mast-cell infiltration was a consequence of elevated histamine release by the proliferated mast cells after mechanical irritation. The tendency to blister in children with DCM usually improves within 3 to 4 years, and most cutaneous lesions spontaneously resolve by adolescence. However, a small number of DCM patients with a family history may have systemic organ involvement and a chronic course. We also need to consider the extra-cutaneous complications that may occur in children with DCM, such as lymphadenopathy, hepatomegaly, splenomegaly, diarrhoea, hypotension, and vasodilatory shock (2). The mainstay of medication treatment of DCM is antihistamines. External stimuli such as friction, heat, physical activity, certain foods, emotional stress, and certain medications should be avoided in daily life.
This report highlights that DCM should be considered in children with diffuse bullous eruption over generalized thickened and dark skin, especially with wheal formation after mechanical irritation. However, by adolescence, regression of the lesions is frequent in childhood-onset DCM.
ACKNOWLEDGEMENTS
This work was supported by grants from the National Natural Science Foundation of China (81903197).
REFERENCES
- Hartmann K, Escribano L, Grattan C, Brockow K, Carter MC, Alvarez-Twose I, et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J Allergy Clin Immunol 2016; 137: 35–45. https://doi.org/10.1016/j.jaci.2015.08.034
- Hudson A, Finlayson L. Diffuse cutaneous bullous mastocytosis and disseminated intravascular coagulation postvaccination: a case report. J Cutan Med Surg 2016; 20: 596–599. https://doi.org/10.1177/1203475416661312