Tissue-specific autoantibodies have been detected in higher frequency in the sera of people living with HIV (PLHIV) compared with matched controls, a phenomenon generally attributed to the immune system’s imbalances associated with the retroviral infection (1). However, recent results in patients showing suppression of viral replication and associated immune reconstitution due to combination antiretroviral therapy (cART) indicate that the prevalence of neutrophil cytoplasmic antibodies (ANCAs), cardiolipin antibodies and various cutaneous autoantibodies in PLHIV is nowadays lower than in the pre-cART era (2–5).
Given the complexity of the structures involved in epithelial cell-cell and cell-matrix attachment, a number of pathogenic autoantibodies are known to elicit clinically heterogeneous autoimmune blistering skin diseases by targeting distinct cutaneous antigens (6, 7). For instance, patients with paraneoplastic pemphigus, a rare, often fatal, autoimmune blistering skin disease associated with neoplasms and usually presenting with a severe, intractable stomatitis and capricious cutaneous signs, often develop autoantibodies against multiple antigens of the plakin and desmoglein family, with anti-envoplakin antibodies being the most specific (8). The binding of these autoantibodies to transitional epithelium (e.g. rat bladder epithelium) is diagnostically important, although newly commercially available enzyme-linked immunosorbent assay (ELISA) to envoplakin may still further increase the diagnostic sensitivity and specificity (9). Another pertinent antigen is type VII collagen, the major component of anchoring fibrils connecting the basement membrane zone with the dermis. Autoantibodies against type VII collagen cause epidermolysis bullosa acquisita, a rare, debilitating, highly variable, and difficult-to-treat condition and the prototypical dermolytic autoimmune skin-blistering disease occurring mainly in elderly individuals (10). Circulating antibodies directed against type VII collagen can be detected with high sensitivity using recombinant antigens in commercially available ELISA, and diagnosis can be confirmed by indirect immunofluorescence studies on sodium chloride-split skin showing linear IgG deposits at the dermal side of an artificially induced split (11).
To date, the frequency and titres of autoantibodies directed against envoplakin and type VII collagen in PLHIV lacking clinical signs of autoimmune blistering diseases compared with HIV- negative control patients are not known and therefore investigated in this study.
METHODS and RESULTS
The presence and titres of type VII collagen and envoplakin autoantibodies in sera from 592 HIV-infected patients and 247 uninfected control patients lacking clinical signs or symptoms reminiscent of any autoimmune blistering skin disease were analysed for the presence of anti- envoplakin and anti-type VII collagen autoantibodies using commercially available ELISAs (Euroimmun Medizinische Labordiagnostika AG, Lübeck, Germany for envoplakin and Medical Biologicals Laboratories Co. Ltd, Nagoya, Japan for type VII collagen, BP180/230 and desmoglein 1/3). Indirect immunofluorescence studies of patients sera were performed by using salt-split human skin or rat bladder epithelium as a substrate, as described previously (12).
The study was conducted according to the principles of the Declaration of Helsinki, approved by the local ethics committee of the Medical University of Vienna (ECS1103/2017) and registered at Clinicaltrials.gov (NCT 03129308), including the outcomes presented here. The study design, patients’ baseline characteristics, and the primary, as well as some secondary, outcomes, except the ones described here were published previously (4).
Detailed baseline characteristics of the patients have been presented earlier (4). Autoantibodies directed against type VII collagen exceeding the upper normal range of 6 U/ml were found in 2.87% (17/592) of HIV-infected patients compared with 2.02% (5/247) of controls (p = 0.48; Fig. S1a, Table I). With the exception of 2 HIV-infected patients, most patients with positive ELISA results had only slightly or moderately elevated titres. However, indirect immunofluorescence studies on human salt-split skin were all negative, irrespective of autoantibody titres. In addition, no significant difference in mean titres was observed between HIV-infected and control patients (1.13 vs 0.98 U/ml; p = 0.34; Table I).
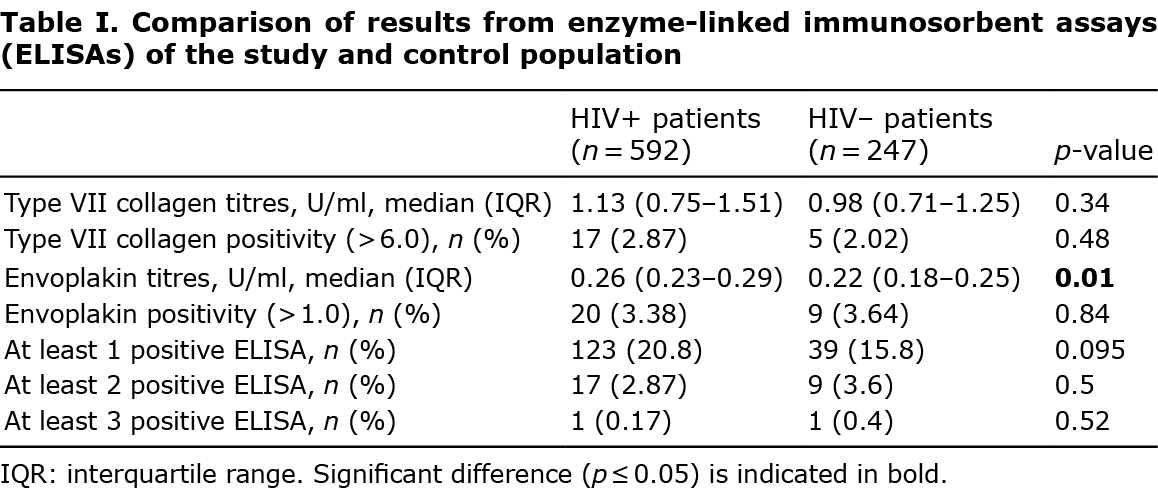
Likewise, the proportion of patients showing positive results for envoplakin autoantibodies was comparable between the groups (3.38% (20/592) vs 3.64% (9/247); p = 0.84; Table I), even though HIV-infected patients displayed significantly higher mean titres (p = 0.01; Fig. S1b, Table I). Indirect immunofluorescence testing on rat bladder transitional epithelium of all sera, including those patients with above-normal levels of anti-envoplakin autoantibodies, was consistently negative.
Graphical analysis of the combinational positivity of the autoantibodies revealed no clear pattern in both HIV-infected and control patients (Fig. S1c). While the majority of patients with a positive ELISA outcome had only one positive ELISA result, 2.9% and 3.6% of HIV-infected and control patients, respectively, had a minimum of 2 positive readings. One patient in each group had 3 or more positive results. The highest frequency of indeterminate results was observed in desmoglein 1 and 3 reactivity, mostly representing borderline results in patients with no otherwise conspicuous findings or with no discernible pattern.
DISCUSSION
This study found a low prevalence of autoantibodies directed against type VII collagen and envoplakin in both PLHIV and uninfected controls lacking signs of autoimmune blistering skin disease. In addition, with the vast majority of patients with positive results showing only (usually modest) reactivity to 1 cutaneous antigen, no specific combination of the studied skin-specific autoantibodies was observed in either group.
In PLHIV as well as uninfected controls single positivity to either type VII collagen or envoplakin was present in 2.0% and 3.6%, respectively, and, thus, within the range of the frequency of the previously studied autoantibodies directed at cutaneous antigens (4). Similar to what has also been observed in rheumatic and haematological autoimmune diseases in PLHIV, these autoantibodies are generally present at low titres and may have little, if any, clinical relevance, given that they were detectable in cohorts lacking symptoms or signs of autoimmune blistering diseases (3). Interestingly, neither a single demographic, nor any biomarker of HIV or systemic infections previously reported (4) predicted the magnitude of, or positivity for, type VII collagen or envoplakin autoantibodies in PLHIV using multivariate statistical modelling (data not shown). Moreover, the positive results in type VII collagen or envoplakin ELISA did not translate into the expected staining patterns in indirect immunofluorescence studies on monkey oesophagus (data not shown), rat bladder epithelium and salt-split human skin, further questioning the clinical relevance of positive results and highlighting the need of correlating positive results of immunoserological testing with the clinical presentation and microscopic studies.
Only approximately 3% of all patients exhibited at least 2 positive ELISA and no particular pattern of the combinational appearance of specific autoantibodies was identified, even when indeterminate results were included (Fig. S1c1). Yet, even though some studies suggest that polyclonal hypergammaglobulinaemia, a common phenomenon in HIV-infected patients, per se does not account for the observed higher likelihood of autoantibody production, it remains to be investigated whether an association of polyclonal hypergammaglobulinaemia with the presence of various cutaneous and/or tissue-specific autoantibodies exists (3).
Now that effective and tolerable antiretroviral treatment is available, many PLHIV can expect to have a more-or-less normal life expectancy, and thus in this ageing population the incidence of autoimmune blistering diseases may be destined to increase (13). Thus, the results of this study may potentially support clinicians in their decision-taking when considering autoimmune blistering diseases as potential differential diagnoses and provide guidance and help when analysing and interpreting results of antibodies tests required for the diagnosis of various autoimmune blistering skin diseases in PLHIV.
ACKNOWLEDGEMENTS
The authors thank Tina Holper for her invaluable technical assistance and Regina Aichwalder, Renate Eder, Manuel Kleinrath, Silvia Kovar, Manuela Lenk and Helmut Stranzl for their continuous help.
This work was supported by a research grant of the Austrian Science Fund (KLI716-B30) and the Austrian AIDS Society to C.S.
The authors have no conflicts of interest to declare.
REFERENCES
- Roszkiewicz J, Smolewska E. Kaleidoscope of autoimmune diseases in HIV infection. Rheumatol Int 2016; 36: 1481–1491.
- Savige JA, Chang L, Horn S, Crowe SM. Anti-nuclear, anti-neutrophil cytoplasmic and anti-glomerular basement membrane antibodies in HIV-infected individuals. Autoimmunity 1994; 18: 205–211.
- Iordache L, Bengoufa D, Taulera O, Rami A, Lascoux-Combe C, Day N, et al. Nonorgan- specific autoantibodies in HIV-infected patients in the HAART era. Medicine (Baltimore) 2017; 96: e6230.
- Touzeau-Roemer V, Skoll M, Tajpara P, Kienzl P, Wesinger A, Saluzzo S, et al. Prevalence of skin-specific autoantibodies in HIV-infected patients and uninfected controls. Acta Derm Venereol 2019; 99: 978–983.
- Rusnak JM, Butzin C, Mc Glasson D, Blatt SP. False-positive rapid plasma reagin tests in human immunodeficiency virus infection and relationship to anti-cardiolipin antibody and serum immunoglobulin levels. J Infect Dis 1994; 169: 1356–1359.
- Baum S, Sakka N, Artsi O, Trau H, Barzilai A. Diagnosis and classification of autoimmune blistering diseases. Autoimmun Rev 2014; 13: 482–489.
- Hammers CM, Stanley JR. Mechanisms of disease: pemphigus and bullous pemphigoid. Annu Rev Pathol Mech Dis 2016; 11: 175–197.
- Huang Y, Li J, Zhu X. Detection of anti-envoplakin and anti-periplakin autoantibodies by ELISA in patients with paraneoplastic pemphigus. Arch Dermatol Res 2009; 301: 703–709.
- Hashimoto T. Production of numerous autoantibodies in paraneoplastic pemphigus. Br J Dermatol 2015; 172: 849–850.
- Vorobyev A, Ludwig RJ, Schmidt E. Clinical features and diagnosis of epidermolysis bullosa acquisita. Expert Rev Clin Immunol 2017; 13: 157–169.
- Schmidt T, Hoch M, Lotfi Jad SS, Solimani F, Di Zenzo G, Marzano AV, et al. Serological diagnostics in the detection of IgG autoantibodies against human collagen VII in epidermolysis bullosa acquisita: a multicentre analysis. Br J Dermatol 2017; 177: 1683–1692.
- Zillikens D, Kawahara Y, Ishiko A, Shimizu H, Mayer J, Rank CV, et al. A novel subepidermal blistering disease with autoantibodies to a 200-kDa antigen of the basement membrane zone. J Invest Dermatol 1996; 106: 1333–1338.
- Wing EJ. HIV and aging. Int J Infect Dis 2016; 53: 61–68.