Subcutaneous thyroid tissue implantation after thyroidectomy is an extremely rare, but possible, event (1). There have been several reports of this condition after fine-needle aspiration biopsy, endoscopic surgery, and conventional thyroidectomy (2, 3). We report here a case of subcutaneous thyroid implantation that clinically mimicked a benign haemangioma.
CASE REPORT
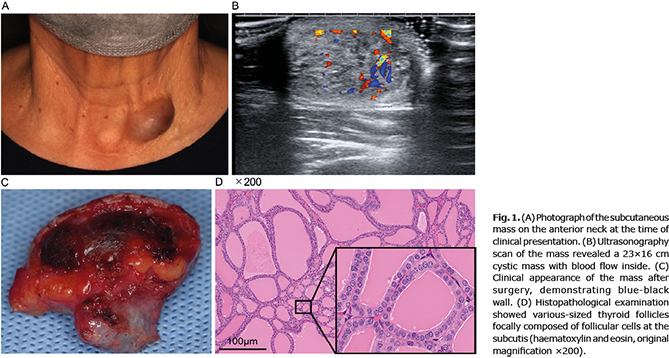
A 75-year-old Japanese woman visited our hospital for an enlarging painless mass on the left side of her anterior neck (Fig. 1A). She had undergone thyroidectomy for adenomatous goitre 11 years previously, and she had a surgical scar below the mass (Fig. 1A). The subcutaneous mass had no history of pain or infection. Ultrasonography revealed a 23×16 mm cystic mass and blood flow inside the mass (Fig. 1B). Haemangioma was suspected and the mass was removed under local anaesthesia. The mass had a blue-black wall, and was located in the subcutaneous tissue, partly attaching to the broad cervical muscle (Fig. 1C). There were many small vessels around the mass. The mass was successfully resected en bloc. Postoperative histopathological analysis revealed various-sized thyroid follicles focally composed of follicular cells at the subcutis (Fig. 1D). No lymphoid tissue was noted. On immunohistochemistry, follicular cells were positive for thyroglobulin (Fig. 2A), thyroid transcription factor 1 (Fig. 2B), CK19, and p53. The Ki-67 index was approximately 5%. No RAS gene mutation was detected. Based on these findings, a diagnosis of subcutaneous thyroid implantation was made. The patient had been taking levothyroxine sodium, and serum Thyroid-stimulating hormone (TSH) and Free thyroxine (F-T4) levels did not differ between before and after surgery.

DISCUSSION
The common differential diagnoses of subcutaneous masses vary, including epidermoid cyst, haemangioma, pilomatricoma, lipoma, and metastatic tumours. Thyroid implantation is extremely rare, but it should be considered in the differential diagnosis when cervical subcutaneous masses are detected. Ectopic thyroid tissue in the neck can be categorized into the following types: (i) true ectopic thyroid tissue, (ii) secondary or metastatic carcinoma, (iii) benign metastatic thyroidosis, (iv) detached nodule, and (v) thyroid implantation (1). In the current case, the superficial location (subcutis), past history of thyroid surgery, and absence of a history of true ectopic thyroid tissue before thyroid surgery led us to the diagnosis of thyroid implantation.
There have only been a few reported cases of thyroid implants (1, 4). The latent periods after surgery in these cases varied. Nodular goitre implants arise 10–20 years after surgery, whereas an implanted thyroid carcinoma and adenoma develop within 5 years (4). Most of those lesions presented as multiple nodules. In the current case, the timing of occurrence was consistent with previous findings, but the tumour was relatively large with a monogenic nature on histopathology. Close imaging examination of the cervical subcutaneous mass is preferable before surgery.
In summary, we report here a rare case of thyroid implantation. The surgical history of patients should be considered carefully in order to exclude neck thyroid implantation.
The authors have no conflicts of interest to declare.
REFERENCES
- Ying Liu, Zhi-Yu Li, Ya-Ping DU. Subcutaneous implantation of benign thyroid tissue: a rare complication after thyroidectomy. Chin Med J (Engl) 2011; 124: 1111–1113.
- Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K, et al. Needle tract implantation of papillary thyroid carcinoma after fine-needle aspiration biopsy. World J Surg 2005; 29: 1544–1549.
- Wille G, Miccoli P. Re: soft tissue implantation of thyroid adenomatous hyperplasia after endoscopic thyroid surgery. Thyroid 2009; 19: 313.
- Harach HR, Cabrera JA, Williams ED. Thyroid implants after surgery and blunt trauma. Ann Diagn Pathol 2004; 8: 61–68.