SHORT COMMUNICATION
JAK Inhibitors in Down Syndrome: Alopecia Areata Resolution and Vitiligo Improvement with Baricitinib
Federica LI POMI1, Mario VACCARO2, Marta VITALE2, Roberta ALAIMO3 and Francesco BORGIA2*
1Department of Precision Medicine in Medical, Surgical and Critical Care (Me.Pre.C.C.), University of Palermo, Palermo, Italy, 2Section of Dermatology, Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy, and 3Fondazione Istituto G. Giglio, Cefalù, Italy. E-mail: fborgia@unime.it
Citation: Acta Derm Venereol 2025; 105: adv44081. DOI: https://doi.org/10.2340/actadv.v105.44081.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 5, 2025. Accepted after revision: Aug 26, 2025. Published: Sep 10, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Down syndrome (DS), most frequently caused by trisomy of chromosome 21, is one of the most common genetic disorders associated with intellectual disability and widespread immune dysregulation. Patients with DS exhibit heightened interferon (IFN) signalling and altered cytokine milieu, predisposing them to several autoimmune and autoinflammatory conditions, including alopecia areata (AA) and vitiligo (1). This enhanced IFN-driven activation provides a compelling mechanistic rationale for targeting Janus kinase (JAK) in DS-associated autoimmunity (2, 3).
AA is characterized by T cell-mediated destruction of anagen hair follicles following loss of immune privilege (4). AA affects approximately 7.4% of individuals with DS, with a mean age of onset of 7 years, an average disease duration of 2.7 years, and a recurrence rate of 27.7% (5). In comparison, the lifetime risk of AA in the general population without DS is 2.1% (1).
Despite the theoretical suitability of JAK inhibition, clinical data on systemic therapies for AA in DS are limited. Baricitinib, a selective JAK1/2 inhibitor approved for severe AA, has demonstrated efficacy in non-DS populations and emerging benefit in vitiligo (6, 7).
Herein, we report the case of 2 patients with DS affected by recalcitrant, severe AA who achieved excellent hair regrowth – and, in 1 case, concomitant vitiligo repigmentation – under treatment with oral baricitinib.
CASE REPORTS
Case 1: A 20-year-old male with DS presented with rapidly progressive, patchy hair loss and a baseline Severity of Alopecia Tool (SALT) score of 70. Previous treatment with high-potency topical and intralesional corticosteroids yielded no significant response. Routine haematological and biochemical tests, viral serologies, and the T-spot test were all within normal limits; therefore, oral baricitinib was initiated at a dose of 4 mg once daily. SALT assessments, standardized clinical photography, and laboratory investigations were performed every 12 weeks. By month 6, the patient’s SALT score had improved to 25, and by month 12, near-complete regrowth was observed (SALT 6) (Fig. 1A–C). The regimen was well tolerated, with no laboratory abnormalities or infections detected. The patient is still taking oral baricitinib.

Fig. 1. Alopecia areata resolution. Alopecia areata patches in the occipital region of a 20-year-old DS male, (A) before treatment; (B) amelioration of the alopecia patches after 9 months of treatment with oral baricitinib; (C) almost complete resolution of alopecia after 12 months of treatment with oral baricitinib; (D) alopecia areata patches in the temporal, parietal, and occipital region of a 18 years-old DS female, before treatment; (E) resolution of the alopecia patches after 9 months of treatment with oral baricitinib; (F) persistence of alopecia resolution after 12 months of treatment with oral baricitinib.
Case 2: An 18-year-old female with DS presented with multiple patches of hair loss in the temporal, occipital, and parietal regions (SALT score of 78). The patient had already undergone treatment with topical and oral corticosteroids, with no improvement. Physical examination revealed a coexisting diffuse non-segmental vitiligo affecting the neck, abdomen, and lower limbs. Wood’s lamp examination accentuated these patches. Routine haematological and biochemical tests, virus serology, and T-spot test were normal. Given the shared IFN-γ-driven pathogenesis of AA and vitiligo, baricitinib 4 mg daily was prescribed. Clinical follow-up revealed rapid hair regrowth, achieving a SALT score of 0 by month 9 (Fig. 1D–F). Simultaneously, significant repigmentation of vitiligo lesions was observed, especially in the neck and pretibial regions. (Fig. 2) The treatment was well tolerated, with no adverse events or laboratory alterations from baseline bloodwork. The patient is still under therapy (Fig. 3).
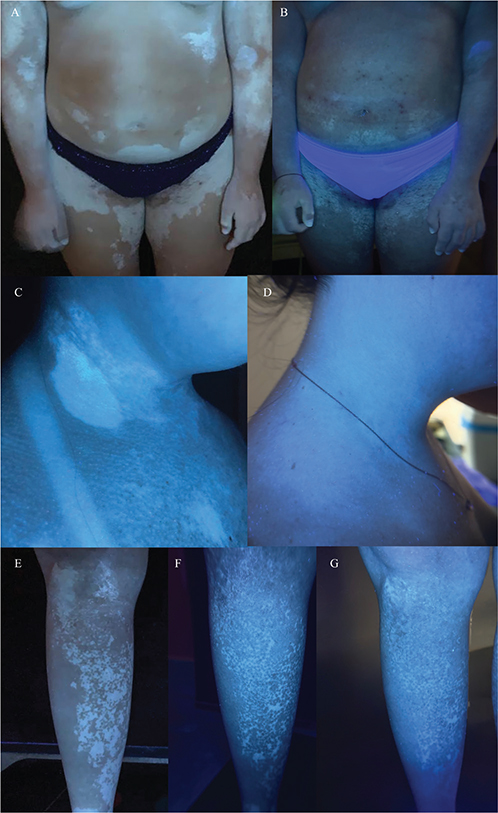
Fig. 2. Vitiligo repigmentation. (A) Several patches of vitiligo before starting the treatment; (B) significant repigmentation of vitiligo patches after 9 months of treatment with oral baricitinib; (C) vitiligo of the neck and décolleté before beginning the treatment; (D) significant repigmentation of neck and décolleté vitiligo patches after 9 months of treatment with oral baricitinib; (E) several nummular patches of vitiligo in the pretibial region before starting the treatment; (F) perifollicular repigmentation pattern in the pretibial region after 6 months of baricitinib therapy; (G) significant perifollicular repigmentation of pretibial vitiligo patches after 9 months of baricitinib.
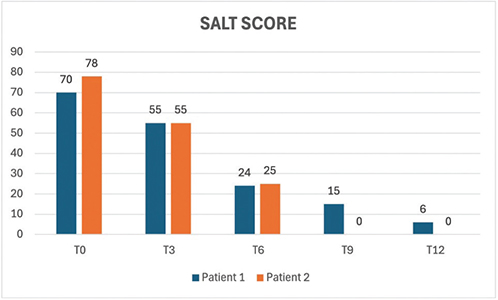
Fig. 3. Severity of Alopecia Tool (SALT) scores in 2 patients.
DISCUSSION
To the best of our knowledge, these are the first reports of baricitinib successfully treating AA – and, in 1 case, associated vitiligo – in patients with DS, a disease characterized by hyperactivation of IFN/JAK/STAT signalling. By inhibiting JAK1/2, baricitinib appears to effectively interrupt disease processes in both hair follicles and melanocytes (8, 9).
AA and vitiligo share a common pathogenesis driven by IFN-γ-mediated Th1 immune responses and cytotoxic CD8+ T cell activity. Both diseases involve the collapse of tissue-specific immune privilege, at the hair follicle in AA and the melanocyte niche in vitiligo, promoted by elevated levels of the chemokines CXCL9 and CXCL10, 2 chemokines elevated in DS and reduced upon JAK inhibition (9, 10). Plasmacytoid dendritic cells initiate IFN signalling, promoting the recruitment and activation of autoreactive CD8+ T cells that target melanocytes and follicular structures. Another key amplifying mechanism in both disorders is the IL-15 axis: produced by keratinocytes, IL-15 supports tissue-resident memory CD8+ T cells and boosts their cytotoxicity through granzyme B and IFN-γ production via JAK1/3 signalling, creating a positive feedback loop (10).
Additionally, both diseases are characterized by oxidative stress and impaired autophagy, which contribute to initial melanocyte and follicular damage and promote antigen presentation. Dysregulation of the Wnt/β-catenin signalling pathway – especially through overexpression of the Wnt inhibitor DKK1 – further impairs tissue homeostasis, affecting melanocyte function in vitiligo and hair follicle regeneration in AA (10).
This convergence of immunological pathways may explain the rationale for using a single JAK inhibitor to target both conditions simultaneously (10). On this topic, Rachubinski et al. have previously reported improvement of AA in patients with DS following treatment with tofacitinib (a JAK1/3 inhibitor), which, however, is not currently approved for the treatment of AA (11). Regarding vitiligo, as shown in previous studies, the vitiligo patches in our patient appeared to repigment more effectively when located in sun-exposed areas, highlighting the potential synergistic effect of sun exposure (12).
Baricitinib was well tolerated in both patients. Never-theless, controlled studies are necessary to define the safety profile, optimal dosing, and durability of response in patients with DS. Given the high burden of autoimmune disease and limited efficacy of conventional therapies in DS, JAK inhibition may represent a rational and promising therapeutic avenue.
In conclusion, oral baricitinib may offer a targeted, well-tolerated option for severe AA in DS, with the potential for dual benefit in IFN-mediated comorbidities such as vitiligo. Larger trials are needed to confirm these preliminary observations and to explore the broader applicability of JAK inhibitors in the DS population.
ACKNOWLEDGEMENTS
IRB approval status: Written informed consents were provided by both patients’ parents to publish the case details and any accompanying images. No IRB was needed.
REFERENCES
- Hom B, Boyd NK, Vogel BN, Nishimori N, Khoshnood MM, Jafarpour S, et al. Down syndrome and autoimmune disease. Clin Rev Allergy Immunol 2024; 66: 261–273.
- Waugh KA, Araya P, Pandey A, Jordan KR, Smith KP, Granrath RE, et al. Mass cytometry reveals global immune remodeling with multi-lineage hypersensitivity to type I interferon in Down syndrome. Cell Rep 2019; 29: 1893–1908.e4. https://doi.org/10.1016/j.celrep.2019.10.038
- Waugh KA, Minter R, Baxter J, Chi C, Galbraith MD, Tuttle KD, et al. Triplication of the interferon receptor locus contributes to hallmarks of Down syndrome in a mouse model. Nat Genet 2023; 55: 1034–1047. https://doi.org/10.1038/s41588-023-01399-7
- Zhou C, Li X, Wang C, Zhang J. Alopecia areata: an update on etiopathogenesis, diagnosis, and management. Clin Rev Allergy Immunol 2021; 61: 403–423.
- Rork JF, McCormack L, Lal K, Wiss K, Belazarian L. Dermatologic conditions in Down syndrome: a single-center retrospective chart review. Pediatr Dermatol 2020; 37: 811–816. https://doi.org/10.1111/pde.14214
- King B, Ohyama M, Kwon O, Zlotogorski A, Ko J, Mesinkovska NA, et al. Two phase 3 trials of baricitinib for alopecia areata. N Engl J Med 2022; 386: 1687–1699.
- Sáenz LM, Villarreal JDM. Unlocking the potential of baricitinib for vitiligo. Cutis 2024; 114: 95–96.
- Rachubinski AL, Wallace E, Gurnee E, Enriquez-Estrada BA, Worek KR, Smith KP, et al. JAK inhibition decreases the autoimmune burden in Down syndrome. eLife 2024; 13: RP99323. https://doi.org/10.7554/eLife.99323
- Galbraith MD, Rachubinski AL, Smith KP, Araya P, Waugh KA, Enriquez-Estrada B, et al. Multidimensional definition of the interferonopathy of Down syndrome and its response to JAK inhibition. Sci Adv 2023; 9: eadg6218. https://doi.org/10.1126/sciadv.adg6218
- Yamaguchi HL, Yamaguchi Y, Peeva E. Pathogenesis of alopecia areata and vitiligo: commonalities and differences. Int J Mol Sci 2024; 25: 4409.
- Rachubinski AL, Estrada BE, Norris D, Dunnick CA, Boldrick JC, Espinosa JM. Janus kinase inhibition in Down syndrome: 2 cases of therapeutic benefit for alopecia areata. JAAD Case Rep 2019; 5: 365–367.
- Liu LY, Strassner JP, Refat MA, Harris JE, King BA. Repigmentation in vitiligo using the Janus kinase inhibitor tofacitinib may require concomitant light exposure. J Am Acad Dermatol 2017; 77: 675–682.e1. https://doi.org/10.1016/j.jaad.2017.05.043