ORIGINAL REPORT
Application of T-SPOT.TB in the Diagnosis of Cutaneous Mycobacterium marinum Infections and Evaluation of Treatment Efficacy
Chen CEN1, Bibo XIE1, Rui ZENG2, Wenyue ZHANG2, Hongsheng WANG2 and Xudong SANG1
1Department of Dermatology, Zhejiang Provincial Dermatology Hospital, Huzhou, China, and 2Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, China
This study evaluated the diagnostic value and therapeutic efficacy assessment potential of the interferon-γ release assay T-SPOT.TB in cutaneous Mycobacterium marinum infections. A total of 145 patients diagnosed at the Institute of Dermatology, Chinese Academy of Medical Sciences (2020–2024), excluding tuberculosis cases, were retrospectively analysed. Clinical data including demographics, underlying diseases, pathology, microbiological culture, molecular identification, T-SPOT.TB results, treatment regimens, and outcomes were collected. T-SPOT.TB results before treatment, and at 3 and 6 months post-treatment, were compared to assess its diagnostic and monitoring utility. The baseline T-SPOT.TB positivity rate was 71% (95% CI: 63.2–77.8%). Among 17 patients retested at 3 months, positivity was 64.7% (p = 0.125), with median spot-forming cells (SFCs) significantly decreasing from 20.0 (IQR 8.5–41.0) to 8.0 (IQR 2.5–28.0) (p = 0.0007). Among 27 patients retested at 6 months, positivity was 59.3% (p = 0.344), with median SFCs decreasing from 12.0 (IQR 5.0–30.0) to 8.0 (IQR 3.0–13.0) (p = 0.0006). No significant difference in positivity rates was observed between 3 and 6 months post-treatment. The T-SPOT.TB assay shows significant diagnostic value for cutaneous M. marinum infections and facilitates early diagnosis. Declining SFC counts post-treatment provide useful reference for evaluating therapeutic response.
SIGNIFICANCE
This study demonstrates that T-SPOT.TB, a standardized interferon-γ release assay (IGRA), can serve as an adjunctive tool for rapid diagnosis and treatment monitoring of cutaneous infections caused by M. marinum. Monitoring dynamic changes in T-SPOT.TB reactivity during treatment provides clinicians with objective immunological data to supplement clinical evaluation of treatment efficacy. This approach may facilitate earlier and more precise diagnosis, enabling optimized treatment strategies that reduce therapeutic delays and improve clinical outcomes – particularly in high-risk populations with aquatic exposures, such as aquaculture workers.
Key words: T-SPOT; TB; cutaneous Mycobacterium marinuminfections; diagnostic value.
Citation: Acta Derm Venereol 2025; 105: adv44119. DOI: https://doi.org/10.2340/actadv.v105.44119.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 11, 2025. Accepted after revision: Oct 9, 2025. Published: Oct 28, 2025.
Corr: Prof. Hongsheng Wang, Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, Jiangsu 210042, China and Dr. Xudong Sang, Department of Dermatology, Zhejiang Provincial Dermatology Hospital, Huzhou 313200, China. E-mails: whs33@vip.sina.com; 358606498@qq.com
Competing interests and funding: This work was supported by the Zhejiang Province Medical and Health Science and Technology Program (2022KY731).
The authors have no conflicts of interest to declare.
INTRODUCTION
Cutaneous Mycobacterium marinum infection is caused by a slow-growing non-tuberculous mycobacterium (NTM) widely present in freshwater and marine environments. It infects humans opportunistically through minor skin abrasions, causing chronic granulomatous skin and soft tissue infections (1, 2). First isolated from fish in 1926, its zoonotic potential was confirmed by the first human case reported in 1951 (3, 4). Epidemiological data remain limited, especially in China, with reported incidence rates varying globally: 0.04/100,000 annually in France (1996–1998) (5), 0.05–0.13 in Denmark (2010–2016) (5), and 0.27 in the United States (6). Recent increases in aquaculture, aquarium ownership, and immunocompromised populations have contributed to rising case numbers (7), suggesting underdiagnosis and underscoring the need for improved surveillance.
Clinical manifestations vary with host immunity, necessitating laboratory confirmation. Traditional diagnostics include acid-fast staining, histopathology, culture, and biochemical identification, each with limitations: low sensitivity and lack of species specificity for staining and histology; prolonged culture times (weeks to months) and susceptibility to prior antibiotics; and molecular methods (PCR, sequencing) offering improved specificity but limited sensitivity on direct specimens and dependence on culture (8, 9). These challenges highlight the need for rapid, sensitive, and specific diagnostic tools.
The T-SPOT.TB assay, an interferon-γ release assay (IGRA), detects T-cell responses to M. tuberculosis-specific antigens ESAT-6 and CFP-10 in peripheral blood mononuclear cells (10). While established for tuberculosis diagnosis and monitoring (11), its role in NTM infections is unclear. Notably, M. marinum shares >85% genomic similarity with M. tuberculosis (12) and expresses the same antigens, explaining frequent false-positive T-SPOT.TB results in cutaneous M. marinum infections (13). This study aims to rigorously evaluate the clinical utility of T-SPOT.TB for diagnosing and monitoring cutaneous M. marinum infections.
MATERIALS AND METHODS
Data collection
We retrospectively reviewed patients diagnosed with cutaneous M. marinum infections at the Dermatology Hospital of the Chinese Academy of Medical Sciences (January 2020–December 2024). Data collected included demographics, underlying diseases, pathology, culture, molecular identification, T-SPOT.TB results, treatment, and outcomes. Inclusion criteria: (i) cutaneous lesions (erythema, nodules, ulcers, abscesses); (ii) histopathology consistent with infectious granulomas or atypical mycobacterial infection; (iii) positive tissue culture with molecular confirmation of M. marinum; (iv) T-SPOT.TB performed before antimycobacterial therapy; (v) no history or evidence of tuberculosis (negative M. tuberculosis qPCR on skin). Exclusion criteria: (i) positive M. tuberculosis qPCR; (ii) history of visceral tuberculosis; (iii) uncertain clinical diagnosis; (iv) prior antimycobacterial treatment. Ethical approval was obtained (Approval No. 2021-KY-013).
T-SPOT.TB assay
T-SPOT.TB was performed at baseline (pre-treatment), 3 months, and 6 months post-treatment, measuring spot-forming cells (SFCs) responding to ESAT-6 (Antigen A) and CFP-10 (Antigen B). Assays and supplementary mycobacteriological tests were conducted in an accredited laboratory. For the interpretation criteria, a result was classified as positive when either the negative control had 0–5 SFCs and the SFC count in Antigen A or Antigen B exceeded the negative control by ≥ 6, or the negative control had 6–10 SFCs and the SFC count in Antigen A or Antigen B was at least twice that of the negative control.
Statistical analysis
SPSS 22.0 (IBM Corp, Armonk, NY, USA) and GraphPad Prism 10.1 (https://www.graphpad.com/features) were used. Categorical variables were frequencies/percentages; continuous variables were mean ± SD or median (IQR). McNemar test compared paired positive rates; Mann–Whitney U test compared independent groups; Wilcoxon signed-rank test compared paired SFCs. P < 0.05 was significant.
RESULTS
Baseline clinical characteristics
Among 372 culture-positive cutaneous M. marinum cases, 145 met the inclusion criteria (44 males [30.3%], 101 females [69.7%]; age 21–78 years, mean 56.23 ± 11.42). Lesions were localized mainly to the hands/upper limbs (95.9%). Rare sites included lower limbs (n = 2), face (n = 2), gluteal region (n = 1), and 1 disseminated case.
T-SPOT.TB assay results
Baseline T-SPOT.TB was positive in 103/145 (71.0%; 95% CI: 63.2–77.8%). All patients received clarithromycin, moxifloxacin, and rifampin combination therapy. Follow-up T-SPOT.TB was performed in 17 patients at 3 months and 27 at 6 months.
T-SPOT.TB at 3 months post-treatment
Among 17 retested, baseline positivity was 88.2% (15/17), decreasing to 64.7% (11/17) at 3 months (p = 0.125). Median SFCs dropped significantly from 20.0 (IQR 8.5–41.0) to 8.0 (IQR 2.5–28.0) (p = 0.0007) (Fig. 1).
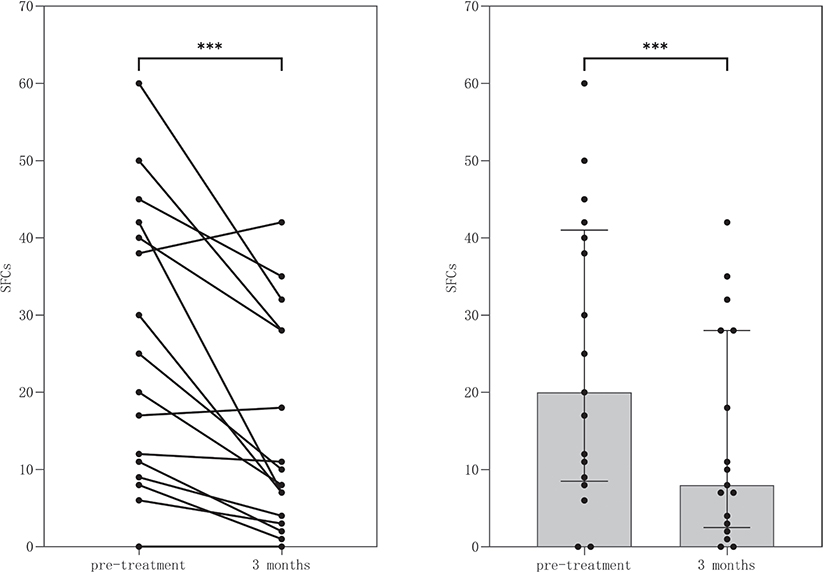
Fig. 1. Changes in SFCs before treatment and at 3 months post-treatment.
T-SPOT.TB at 6 months post-treatment
Among 27 retested, baseline positivity was 74.1% (20/27), decreasing to 59.3% (16/27) at 6 months (p = 0.344). There was no significant difference in positivity between 3 and 6 months (p = 0.645). Median SFCs decreased from 12.0 (IQR 5.0–30.0) to 8.0 (IQR 3.0–13.0) (p = 0.0006) (Fig. 2).
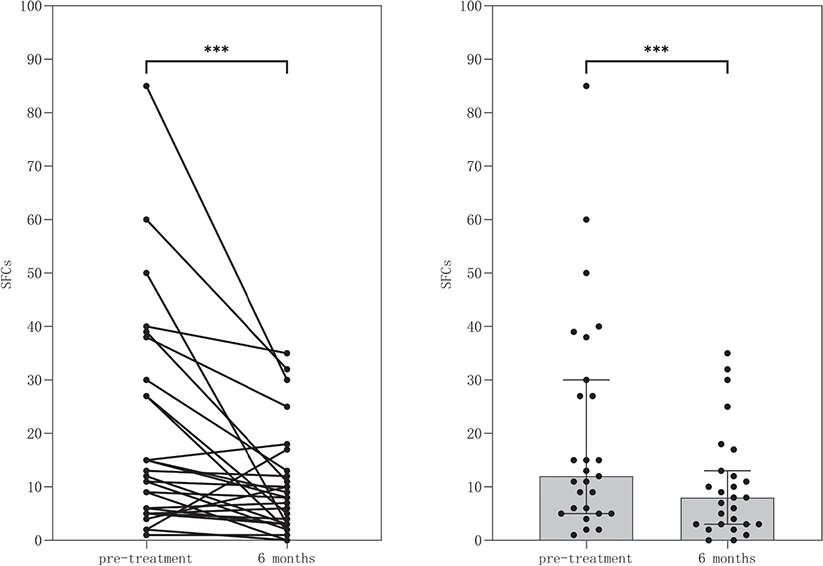
Fig. 2. Changes in SFCs before treatment and at 6 months post-treatment.
DISCUSSION
Cutaneous M. marinum is the leading cause of cutaneous NTM infections, accounting for 50–80% of cases (14, 15), with higher incidence in coastal/lakeside areas and increasing reports worldwide (7, 14, 16). Ageing populations, rising immunocompromised individuals (e.g., diabetes, HIV/AIDS), and expanded immunosuppressive therapies have increased the susceptibility to and severity of infections (17). Aquaculture growth and aquatic recreational activities elevate exposure risk via skin microabrasions. Molecular diagnostics and heightened clinical awareness have improved detection, yet public knowledge and preventive measures remain inadequate, contributing to infection risk.
Misdiagnosis is common; fewer than 60% receive timely diagnosis and treatment within 3 months of symptom onset (5, 18), leading to prolonged disease and resource waste. Diagnosis requires comprehensive assessment including exposure history, lesion morphology, histology, microbiology, molecular tests, and treatment response (19). Culture remains the gold standard but is limited by variable positivity (2.9–96.8%) and long incubation times (19). Molecular methods offer rapid, sensitive species identification but are costly and require specialized facilities, limiting widespread use (8, 20).
The T-SPOT.TB assay, measuring interferon-γ release to ESAT-6 and CFP-10, is a sensitive and specific immunological tool for M. tuberculosis diagnosis and monitoring (11, 21, 22). Given the shared RD1 region encoding these antigens in M. marinum and other NTMs (23), T-SPOT.TB positivity is common in cutaneous M. marinum infections (24), consistent with our 71% positivity rate. Skin infections by other RD1-positive NTMs are rare clinically, making T-SPOT.TB a valuable early screening tool for M. marinum infection in patients presenting with granulomatous lesions, a history of aquatic exposure, distal upper limb involvement, and no evidence of pulmonary involvement. Positive results can guide early empirical therapy pending confirmatory tests (see Fig. 3). However, in tuberculosis (TB) endemic regions, the interpretation of T-SPOT.TB results for M. marinum diagnosis requires particular caution due to antigenic similarities between M. tuberculosis and M. marinum. Before considering T-SPOT.TB as an adjunctive test for M. marinum infection, clinicians must systematically rule out tuberculosis through detailed exposure history and chest CT imaging. This exclusion protocol is critical given the assay’s inability to differentiate between tuberculous and non-tuberculous mycobacterial infections due to shared RD1 antigens.
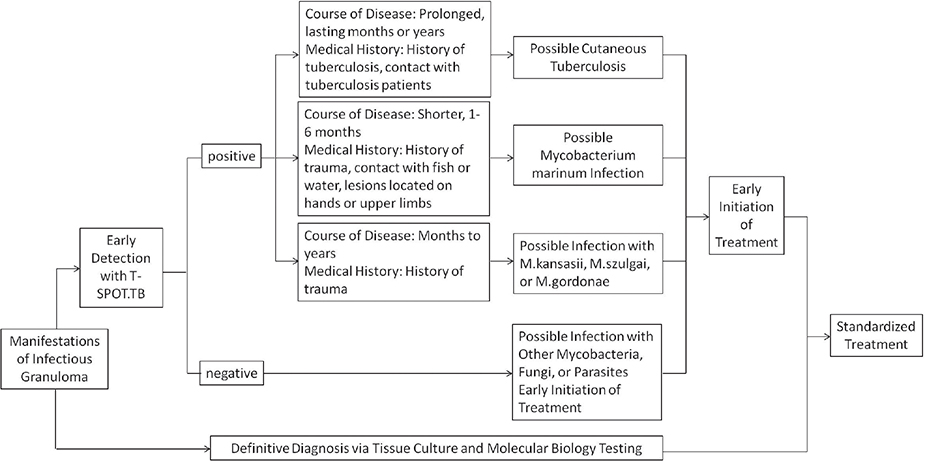
Fig. 3. Diagnostic flowchart for cutaneous M. marinum infections.
Standard treatment includes clarithromycin, moxifloxacin, and rifampin or ethambutol for 4–6 months, continuing 1–2 months after lesion resolution (25–28). While T-SPOT.TB positivity rates did not significantly change post-treatment, SFC counts declined significantly, especially in patients with higher baseline values, suggesting potential utility in monitoring therapeutic response. In clinical management, T-SPOT.TB assay can be performed every 3 months in patients with M. marinum infection undergoing standardized therapy. Monitoring SFCs alongside clinical symptom improvement provides a reliable assessment of therapeutic efficacy and informs the determination of the optimal treatment duration. Some patients showed paradoxical SFC increases despite clinical resolution, possibly due to immune reconstitution or residual antigen stimulation (29, 30), warranting further study. Prior research indicates that dynamic T-SPOT.TB changes do not consistently correlate with clinical improvement or pathogen clearance (31, 32), limiting its role as a definitive treatment marker. Our follow-up sample size was limited, and individual variability may bias results. Larger multicentre studies are needed to clarify T-SPOT.TB’s role in treatment monitoring.
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to the colleagues at the Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College for their work in sample processing and technical assistance.
IRB approval status: Approval for this study was received from the Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College (Approval No. [2021-KY-013]).
REFERENCES
- Tsiolakkis G, Liontos A, Filippas-Ntekouan S, Matzaras R, Theodorou E, Vardas M, et al. Mycobacterium marinum: a case-based narrative review of diagnosis and management. Microorganisms 2023; 11: 1799. http://doi.org/10.3390/microorganisms11071799
- Canetti D, Riccardi N, Antonello RM, Nozza S, Sotgiu G. Mycobacterium marinum: A brief update for clinical purposes. Eur J Intern Med 2022; 105: 15–19. http://doi.org/10.1016/j.ejim.2022.07.013
- Linell F, Norden A. Mycobacterium balnei, a new acid-fast bacillus occurring in swimming pools and capable of producing skin lesions in humans. Acta Tuberc Scand Suppl 1954; 33: 1–84.
- Norden A, Linell F. A new type of pathogenic Mycobacterium. Nature 1951; 168: 826. http://doi.org/10.1038/168826a0
- Holden IK, Kehrer M, Andersen AB, Wejse C, Svensson E, Johansen IS. Mycobacterium marinum infections in Denmark from 2004 to 2017: A retrospective study of incidence, patient characteristics, treatment regimens and outcome. Sci Rep 2018; 8: 6738. http://doi.org/10.1038/s41598-018-24702-7
- Aubry A, Mougari F, Reibel F, Cambau E. Mycobacterium marinum. Microbiol Spectr 2017; 5: 10.1128/microbiolspec.tnmi7-0038-2016. http://doi.org/10.1128/microbiolspec.TNMI7-0038-2016
- Mei Y, Zhang W, Shi Y, Jiang H, Chen Z, Chokkakula S, et al. Cutaneous tuberculosis and nontuberculous mycobacterial infections at a national specialized hospital in China. Acta Derm Venereol 2019; 99: 997–1003. http://doi.org/10.2340/00015555-3283
- Kunduracılar H. Identification of mycobacteria species by molecular methods. Int Wound J 2020; 17: 245–250. http://doi.org/10.1111/iwj.13238
- Lv Z, Zhang M, Zhang H, Lu X. Utility of real-time quantitative polymerase chain reaction in detecting mycobacterium tuberculosis. Biomed Res Int 2017; 2017: 1058579. http://doi.org/10.1155/2017/1058579
- Mori T, Sakatani M, Yamagishi F, Takashima T, Kawabe Y, Nagao K, et al. Specific detection of tuberculosis infection: an interferon-gamma-based assay using new antigens. Am J Respir Crit Care Med 2004; 170: 59–64. http://doi.org/10.1164/rccm.200402-179OC
- Liao CH, Chou CH, Lai CC, Huang YT, Tan CK, Hsu HL, et al. Diagnostic performance of an enzyme-linked immunospot assay for interferon-gamma in extrapulmonary tuberculosis varies between different sites of disease. J Infect 2009; 59: 402–408. http://doi.org/10.1016/j.jinf.2009.10.001
- Orgeur M, Brosch R. Evolution of virulence in the Mycobacterium tuberculosis complex. Curr Opin Microbiol 2018; 41: 68–75. http://doi.org/10.1016/j.mib.2017.11.021
- Nachimuthu N, Yatam Ganesh S. Diagnosis of mycobacterium marinum infection based on seroconversion of QuantiFERON-TB gold test. Cureus 2020; 12: e9208. http://doi.org/10.7759/cureus.9208
- Wentworth AB, Drage LA, Wengenack NL, Wilson JW, Lohse CM. Increased incidence of cutaneous nontuberculous mycobacterial infection, 1980 to 2009: a population-based study. Mayo Clin Proc 2013; 88: 38–45. http://doi.org/10.1016/j.mayocp.2012.06.029
- Bouceiro-Mendes R, Ortins-Pina A, Fraga A, Marques T, Viveiros M, Machado D, et al. Mycobacterium marinum lymphocutaneous infection. Dermatol Online J 2019; 25: 13030/qt5bb78905.
- Wang XY, Jia QN, Li J, Zheng HY. Investigating cutaneous tuberculosis and nontuberculous mycobacterial infections a Department of Dermatology, Beijing, China: a comprehensive clinicopathological analysis. Front Cell Infect Microbiol 2024; 14: 1451602. http://doi.org/10.3389/fcimb.2024.1451602
- Franco-Paredes C, Marcos LA, Henao-Martínez AF, Rodríguez-Morales AJ, Villamil-Gómez WE, Gotuzzo E, et al. Cutaneous Mycobacterial Infections. Clin Microbiol Rev 2018; 32: e00069-18. http://doi.org/10.1128/cmr.00069-18
- Johnson MG, Stout JE. Twenty-eight cases of Mycobacterium marinum infection: retrospective case series and literature review. Infection 2015; 43: 655–662. http://doi.org/10.1007/s15010-015-0776-8
- Feng Y, Xu H, Wang H, Zhang C, Zong W, Wu Q. Outbreak of a cutaneous Mycobacterium marinum infection in Jiangsu Haian, China. Diagn Microbiol Infect Dis 2011; 71: 267–272. http://doi.org/10.1016/j.diagmicrobio.2011.07.003
- Delghandi MR, El-Matbouli M, Menanteau-Ledouble S. Mycobacteriosis and infections with non-tuberculous mycobacteria in aquatic organisms: a review. Microorganisms 2020; 8: 1368. http://doi.org/10.3390/microorganisms8091368
- Chen Y, Jiang H, Zhang W, Chen Z, Mei Y, Chen H, et al. Diagnostic Value of T-SPOT.TB test in cutaneous mycobacterial infections. Acta Derm Venereol 2018; 98: 989–990. http://doi.org/10.2340/00015555-3011
- Chen Y, Jiang J, Jiang H, Chen J, Wang X, Liu W, et al. Mycobacterium gordonae in patient with facial ulcers, nosebleeds, and positive T-SPOT.TB test, China. Emerg Infect Dis 2017; 23: 1204–1206. http://doi.org/10.3201/eid2307.162033
- Kobashi Y, Obase Y, Fukuda M, Yoshida K, Miyashita N, Oka M. Clinical reevaluation of the QuantiFERON TB-2G test as a diagnostic method for differentiating active tuberculosis from nontuberculous mycobacteriosis. Clin Infect Dis 2006; 43: 1540–1546. http://doi.org/10.1086/509327
- Lai CC, Tan CK, Lin SH, Liu WL, Liao CH, Huang YT, et al. Diagnostic value of an enzyme-linked immunospot assay for interferon-γ in cutaneous tuberculosis. Diagn Microbiol Infect Dis 2011; 70: 60–64. http://doi.org/10.1016/j.diagmicrobio.2010.11.012
- Strobel K, Sickenberger C, Schoen C, Kneitz H, Kolb-Mäurer A, Goebeler M. Diagnosis and therapy of Mycobacterium marinum: a single-center 21-year retrospective analysis. J Dtsch Dermatol Ges 2022; 20: 1211–1218. http://doi.org/10.1111/ddg.14847
- Yeo PM, Lee SX, Tan YE, Sng LH, Ang CC. Epidemiology, risk factors, and outcomes of adult cutaneous non-tuberculous mycobacterial infection over a 10-year period in Singapore. Int J Dermatol 2019; 58: 679–687. http://doi.org/10.1111/ijd.14356
- Chung J, Ince D, Ford BA, Wanat KA. Cutaneous infections due to nontuberculosis mycobacterium: recognition and management. Am J Clin Dermatol 2018; 19: 867–878. http://doi.org/10.1007/s40257-018-0382-5
- Wang XY, Jia QN, Li J. Treatment of non-tuberculosis mycobacteria skin infections. Front Pharmacol 2023; 14: 1242156. http://doi.org/10.3389/fphar.2023.1242156
- Pai M, Denkinger CM, Kik SV, Rangaka MX, Zwerling A, Oxlade O, et al. Gamma interferon release assays for detection of mycobacterium tuberculosis infection. Clin Microbiol Rev 2014; 27: 3–20. http://doi.org/10.1128/cmr.00034-13
- Xin H, Cao X, Zhang H, Liu J, Pan S, Li X, et al. Dynamic changes of interferon gamma release assay results with latent tuberculosis infection treatment. Clin Microbiol Infect 2020; 26: 1555.e1551–1555.e1557. http://doi.org/10.1016/j.cmi.2020.02.009
- Pourakbari B, Mamishi S, Benvari S, Sauzullo I, Bedini A, Valentini P, et al. Can interferon-γ release assays be useful for monitoring the response to anti-tuberculosis treatment? A systematic review and meta-analysis. Arch Immunol Ther Exp (Warsz) 2020; 68: 4. http://doi.org/10.1007/s00005-020-00568-4
- Clifford V, He Y, Zufferey C, Connell T, Curtis N. Interferon gamma release assays for monitoring the response to treatment for tuberculosis: a systematic review. Tuberculosis (Edinb) 2015; 95: 639–650. http://doi.org/10.1016/j.tube.2015.07.002