ORIGINAL REPORT
Atopic Dermatitis in Denmark: Regional Variation
Kristina IBLER1, Ann HÆRSKJOLD1, Jens OLSEN2, Lotte THEMSTRUP3, Maiken DALAGER4, Lone SKOV5, Charlotte G. MORTZ6, Emilie BALK-MØLLER7 and Christian VESTERGAARD8
1Department of Dermatology, Bispebjerg Hospital, Copenhagen University Hospital, Copenhagen, 2EY Parthenon, Frederiksberg, 3Department of Dermatology, Zealand University Hospital, Roskilde, 4Department of Dermatology, Aalborg University Hospital, Aalborg, 5Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte, Copenhagen, 6Department of Dermatology and Allergy Centre, Odense University Hospital, University of Southern Denmark, Odense, 7Medical Affairs, Sanofi Denmark, and 8Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
Using national registers, this study investigates regional variations in the number of individuals with and treatment of atopic dermatitis (AD) in Denmark. AD, a prevalent chronic skin disorder, affects up to 20% of children and 3% of adults globally; yet its epidemiology in Denmark remains unclear. A recent study indicated a lifetime prevalence of 21% among school-aged children in Odense, a medium-sized city in Denmark, highlighting the long-lasting nature of the condition. With advancements in machine learning, researchers can now identify AD cases in both adults and children through healthcare utilization data. While Denmark’s single-payer system aims to provide equitable access to healthcare, factors such as decentralized administration and patient choice can lead to regional variations in the treatment setup. The study spans from 1995 to 2020, revealing an overall identification of 537,001 individuals with AD. Results demonstrate consistent regional variations, with the Central Denmark Region exhibiting the highest recorded rates over 11 out of 14 years. There are also notable differences in advanced treatment rates and hospital consultations among regions. Thus, regional variation was observed, and to reduce unwarranted regional variation it is important to minimize diagnostic uncertainty and provide clearer guidance on when and how to treat AD.
SIGNIFICANCE
Atopic dermatitis is a common chronic skin condition that affects up to 20% of children and 3% of adults worldwide, causing significant discomfort and a lower quality of life. In Denmark, studies show that 21% of schoolchildren experience this condition, with cases often continuing into adolescence. New machine learning techniques allow for better identification of atopic dermatitis cases, even those not recorded in hospitals. Research using Denmark’s health data reveals ongoing differences in how frequently atopic dermatitis occurs and how it is treated across 5 regions, emphasizing the importance of consistent healthcare practices for all patients.
Key words: atopic dermatitis; regional variations; prevalence.
Citation: Acta Derm Venereol 2026; 106: adv44122. DOI: https://doi.org/10.2340/actadv.v106.44122.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 11, 2025. Accepted after revision: Nov 24, 2025. Published: Feb 10, 2026.
Corr: Jens Olsen, Economics, EY Parthenon, Frederiksberg, Denmark. E-mail: jens.olsen@parthenon.ey.com
Competing interests and funding: KI has received honoraria from Leo Pharma, Sanofi, and Almirall. She has served as investigator for Sanofi and Almirall. AH reports no conflict of interest. JO is an employee of EY Parthenon. EY Parthenon is a paid vendor of Sanofi. LT reports no conflict of interest. MD has been a speaker or has served on advisory boards for Sanofi, AbbVie, LEO Pharma, Pfizer, Eli Lilly, Novartis, UCB Pharma, Almirall, Bristol Meyers Squibb, Boehringer Ingelheim, and AstraZeneca, and has been sub-investigator in clinical trials for Sanofi, Almirall, Johnson & Johnson, and UCB. LS has been a paid speaker for AbbVie, Eli Lilly, Takeda, Sanofi, Pfizer, and LEO Pharma, and has been a consultant or has served on Advisory Boards with AbbVie, Janssen Cilag, Eli Lilly, LEO Pharma, UCB, Almirall, Bristol-Myers Squibb, Takeda, Stada, and Sanofi, and has received research and educational grants from Sanofi, Bristol-Myers Squibb, Almirall, UCB, and Janssen-Cilag. CGM reports no conflict of interest. EBM is a Sanofi employee and may hold shares and/or stock options in the company. CV has received honoraria from Novartis, AbbVie, Leo Pharma, Sanofi, GSK, Pierre Fabre, Almirall, Chiesi, and Pfizer. He has received unrestricted Grants from Novartis, Sanofi, and LEO Pharma, and has served as an investigator for Novartis, AbbVie, Sanofi, Almirall, and Pfizer.
This study was funded by Sanofi. Jan Håkon Rudolfsen from EY provided assistance with medical writing.
INTRODUCTION
Atopic dermatitis (AD) is a chronic inflammatory skin condition characterized by itchiness and recurrent eczematous lesions (1–4). Globally, AD affects up to 20% of children and 3% of adults (5, 6). The chronicity, visibility, and symptom severity of AD can lead to substantial discomfort, psychosocial impact, and diminished quality of life for patients (7).
In Denmark the epidemiology of AD is not fully understood. In a study among 8th grade school children in Odense, a mid-sized city in Denmark with a population of 180,000 inhabitants, it was found that the lifetime prevalence of atopic dermatitis was 21% (8) and after 15 years of follow-up it persisted in 50% of the cases diagnosed at school age (9). Yet, until recently only individuals with AD treated in the hospital sector could be directly identified in Danish healthcare registers.
Advancements in the field have improved the ability to identify population-based cases of AD. A machine learning algorithm has been developed to identify adult AD cases not explicitly coded with an ICD-10 diagnosis in the National Patient Register (NPR), using data on primary care visits and dermatological medication prescriptions. Similarly, a separate algorithm has been developed for identifying AD in children (10, 11). These tools significantly enhance the accuracy of population-based estimates of the number of individuals with AD and treatment patterns in Denmark.
While Denmark’s single-payer system aims to provide equitable access to healthcare, factors such as decentralized administration, patient choice, and regional variations can lead to differences in treatment approaches for individuals with similar needs. Regional variations in AD treatment may reflect appropriate responses to genuine differences in disease presentation and severity. However, it is essential to investigate these variations to ensure they align with evidence-based practices and do not result in inequitable care. Addressing any unjustified disparities is crucial for providing personalized and targeted care for AD patients across all regions.
Denmark is divided into 5 administrative regions: the Capital Region, the Central Denmark Region, the North Denmark Region, Region Zealand, and the Region of Southern Denmark. All regions provide hospital access and specialized care for AD patients. In addition, many AD patients are diagnosed and treated in the primary healthcare sector by general practitioners (GPs) or private dermatologists. These practitioners are funded by the regions through fee-for-service agreements established via collective bargaining. While patients treated in primary care are not recorded in the NPR, their prescription medication use is documented in the National Prescription Register (12, 13).
This study aims to utilize Denmark’s extensive national health and administrative registers to investigate the prevalence of AD and regional variations in treatment strategies. These robust databases enable longitudinal tracking of healthcare utilization across the entire Danish population. By offering a detailed analysis of treatment approaches, the study aims to generate valuable insights to guide healthcare providers and policy-makers in optimising AD management and ensuring equitable care delivery across Denmark.
MATERIAL AND METHODS
Data were extracted from Danish national health and administrative registers, which contain extensive data on healthcare utilization, prescriptions, and patient demographics. Activity in the healthcare sector is routinely reported for administrative and reimbursement purposes and covers the entirety of the Danish population. These registers are linked through a unique 10-digit personal identification number, allowing for the precise merging of individual health and demographic records across different sources. In this study, data were available from 1995 to 2020. Yearly identification of AD and results regarding advanced treatment is reported by administrative regions from 2008 onwards, as this is the first full year after the establishment of the current hospital regions.
The patient population for this study was identified through multiple methods: Using the ICD-10 code L20 in the National Patient Register (NPR) (14), which includes patients diagnosed within the hospital system; applying a machine learning algorithm specifically designed to distinguish AD from other skin diseases in adults; and employing a second algorithm tailored to identify AD in children. These approaches ensure the inclusion of AD patients treated in the primary care sector who may not be captured in the NPR.
The algorithm for identifying adults with atopic dermatitis (AD) was developed to differentiate AD from other skin conditions by analysing healthcare utilization patterns. It was trained and tested on individuals diagnosed with skin conditions in hospital settings, as recorded in the National Patient Register (NPR). The model utilized data on prescription medications from the National Prescription Register (15) and primary care interactions from the Danish National Health Service Register for Primary Care (16), enabling it to effectively distinguish AD from other dermatological conditions.
To identify children with atopic dermatitis (AD), an algorithm developed by Henriksen et al. (2015) (10) was applied. This model identified individuals based on hospital diagnoses recorded in the National Patient Register (NPR) or the use of disease-specific prescription medications (tacrolimus, pimecrolimus, or “corticosteroids for topical use” [10]) from the National Prescription Register. The frequency of prescription medication collection was used as a classification criterion, and individuals with comorbidities associated with similar patterns of drug consumption were excluded.
Statistical analysis
In AD, and other conditions, the actual incidence date is difficult to determine. The incidence date of AD was defined as the date of the first registered diagnosis code of AD or as the date of the first collection of AD-related dermatological medication, based on the specified identification criteria (i.e., identification via the algorithm for children, the algorithm for adults, or via registered diagnosis code of AD). To enable regional comparisons, incidence rates were age-adjusted using direct standardization for the regional population each year, divided into 4 age strata. Additionally, given the differing treatment approaches for children (under 18 years) and adults (18 years and older), age-specific incidence rates are also presented. Regional affiliation for individuals with AD was determined based on their region of residence at the time of their incidence date.
To assess hospital access for individuals with AD, the percentage of individuals with AD who had at least 1 AD-related hospital contact during the study period was presented. An AD-related hospital contact was defined as an inpatient or outpatient contact where the ICD-10 diagnosis code L20 was recorded as either a primary or secondary diagnosis.
Lastly, to present regional variation in access to advanced treatment, the rate of individuals who collected a prescription for at least 1 advanced treatment at a pharmacy, or received advanced treatment at a hospital, was identified. Advanced treatments were identified as treatment with any of the following medications: ciclosporin, methotrexate, azathioprine or mycophenolate mofetil (systemic), dupilumab or tralokinumab (biologics), or abrocitinib, baricitinib, or upadacitinib (JAK inhibitors). Given the advancements in advanced treatments for AD during the study period, regional treatment rates are presented as relative treatment rates, compared with the national treatment rate for each year. To illustrate both inter- and intraregional variation, the relative treatment rates are visualized using a strip chart for each year.
The advanced treatment rates were calculated as the number of individuals receiving advanced treatment for the first time each year, divided by the prevalence of AD in the respective region during the same year. A sensitivity analysis was performed using the total regional population as the denominator, irrespective of AD prevalence. This alternative approach did not alter the overall findings or interpretations of the results.
RESULTS
Summary statistics of the AD population are presented in Table I. A total of 537,001 individuals with AD were identified in the study period (1995–2020). By the end of 2020, 457,876 individuals identified with AD were alive and resident in Denmark (prevalence estimate). The median age at the defined incidence date was 9.5 years (mean age 19 years), with 52% of the individuals being female, and 59% being identified as children. Taking the population figures into account, the age distribution of identified individuals per 100,000 was: 0–5 years: 66%; 6–11 years: 15%; 12–17 years: 16%; 18+ years: 3%. Relatively many adults were identified in the first years of the study period, indicating that these individuals probably met the inclusion criteria before 1995 at a younger age (for some, as children). Regarding age, sex, income, or education, no significant regional variation was observed in the personal characteristics of the AD population.
| Item | Total | Capital Region (31%*) | Central Denmark Region (23%*) | North Denmark Region (10%*) | Region Zealand (15%*) | Region of Southern Denmark (21%*) |
| N (% of total population) | 537,001 | 167,129 (31%) | 126,005 (23%) | 52,093 (10%) | 74,288 (14%) | 117,486 (22%) |
| Age, years, mean (SD) | 19 (21) | 18.7 (21) | 18.1 (20) | 20.1 (21) | 20.8 (22) | 18.8 (20.6) |
| <18 years | 315,720 (59%) | 97,659 (58%) | 76,288 (61%) | 29,629 (57%) | 42,049 (57%) | 70,095 (60%) |
| Income | ||||||
| Annual income**, euros, 2021 prices, mean (SD) | 36,046 (42,440) | 39,179 (51,083) | 34,793 (46,985) | 33,212 (30,821) | 35,770 (30,260) | 34,407 (34,748) |
| Sex | ||||||
| Female | 278,557 (52%) | 87,055 (52%) | 65,089 (52%) | 26,860 (52%) | 38,689 (52%) | 60,864 (52%) |
| Male | 258,444 (48%) | 80,074 (48%) | 60,916 (48%) | 25,233 (48%) | 35,599 (48%) | 56,622 (48%) |
| Education | ||||||
| Bachelor or equivalent | 21,593 (4%) | 7,990 (5%) | 4,677 (4%) | 1,828 (4%) | 2,696 (4%) | 4,402 (4%) |
| Elementary school | 82,562 (15%) | 21,296 (13%) | 19,348 (15%) | 9,538 (18%) | 12,941 (17%) | 19,439 (17%) |
| Not in the education registers | 13,990 (3%) | 5,418 (3%) | 2,718 (2%) | 1,379 (3%) | 1,823 (2%) | 2,652 (2%) |
| Master or higher | 8,562 (2%) | 4,605 (3%) | 1,515 (1%) | 541 (1%) | 797 (1%) | 1,104 (1%) |
| Secondary education | 88,321 (16%) | 27,999 (17%) | 20,104 (16%) | 8,679 (17%) | 13,061 (18%) | 18,478 (16%) |
| Short cycle tertiary | 6,253 (1%) | 2,162 (1%) | 1,355 (1%) | 499 (1%) | 921 (1%) | 1,316 (1%) |
| *Region size of Denmark. The Danish Regions were established in 2008. However, data in the registers can also be categorized by the 2008 regional categorization for 1995–2007, as this categorization is based on data on municipality of residence. **Annual income in population aged 25–65 years old. SD: standard deviation. Index: time of identification. |
||||||
Table II presents healthcare contact associated with AD incidence, stratified by age. Overall, the majority of individuals (60.1%) were diagnosed following a visit to their general practitioner. Together, general practitioners and private practising dermatologists diagnosed 95.2% of the total population. For 1.3% of the population, the healthcare contact could not be determined, and diagnosis was made based on the collection of prescription medications.
| Item | Total | Capital region of Denmark | Central region of Denmark | North Denmark Region | Region Zealand | Region of Southern Denmark |
| Under 6 years at index | ||||||
| General practitioner | 125,347 (60.9) | 37,652 (55.6) | 31,674 (64.9) | 11,797 (63.7) | 16,248 (61.9) | 27,976 (62.9) |
| Dermatologist | 65,846 (32) | 25,557 (37.8) | 14,580 (29.9) | 5,839 (31.5) | 8,655 (33) | 11,215 (25.2) |
| Hospital contact | 14,306 (7) | 4,362 (6.4) | 2,517 (5.2) | 879 (4.7) | 1,325 (5) | 5,223 (11.7) |
| No contact registered | 264 (0.1) | 105 (0.2) | 54 (0.1) | 14 (0.1) | 28 (0.1) | 63 (0.1) |
| 6–11 years at index | ||||||
| General practitioner | 31,894 (60.9) | 8,112 (53.9) | 8,574 (65.4) | 3,127 (60.1) | 4,558 (62.5) | 7,523 (64.4) |
| Dermatologist | 19,222 (36.7) | 6,564 (43.6) | 4,260 (32.5) | 1,987 (38.2) | 2,623 (35.9) | 3,788 (32.4) |
| Hospital contact | 759 (1.5) | 198 (1.3) | 176 (1.3) | 58 (1.1) | 69 (0.9) | 258 (2.2) |
| No contact registered | 457 (0.9) | 164 (1.1) | 99 (0.8) | 33 (0.6) | 47 (0.6) | 114 (1) |
| 12–17 years at index | ||||||
| General practitioner | 32,075 (55.7) | 7,267 (48.6) | 8,564 (59.7) | 3,302 (56) | 4,755 (56) | 8,187 (58.8) |
| Dermatologist | 24,709 (42.9) | 7,439 (49.8) | 5,558 (38.7) | 2,528 (42.9) | 3,660 (43.1) | 5,524 (39.6) |
| Hospital contact | 468 (0.8) | 119 (0.8) | 132 (0.9) | 33 (0.6) | 39 (0.5) | 145 (1) |
| No contact registered | 373 (0.6) | 120 (0.8) | 100 (0.7) | 32 (0.5) | 42 (0.5) | 79 (0.6) |
| 18 or above at index | ||||||
| General practitioner | 133,441 (60.3) | 38133 (54.9) | 31,662 (63.7) | 14,035 (62.5) | 18,903 (58.6) | 30,708 (64.8) |
| Dermatologist | 78,748 (35.6) | 27,791 (40) | 15,949 (32.1) | 7,794 (34.7) | 12,353 (38.3) | 14,861 (31.4) |
| Hospital contact | 3,096 (1.4) | 1,121 (1.6) | 838 (1.7) | 134 (0.6) | 275 (0.9) | 728 (1.5) |
| No contact registered | 5,996 (2.7) | 2,425 (3.5) | 1,268 (2.6) | 501 (2.2) | 708 (2.2) | 1094 (2.3) |
| Total | ||||||
| General practitioner | 322,757 (60.1) | 91,164 (54.5) | 80,474 (63.9) | 32,261 (61.9) | 44,464 (59.9) | 74,394 (63.3) |
| Dermatologist | 188,525 (35.1) | 67,351 (40.3) | 40,347 (32) | 18,148 (34.8) | 27,291 (36.7) | 35,388 (30.1) |
| Hospital contact | 18,629 (3.5) | 5,800 (3.5) | 3,663 (2.9) | 1,104 (2.1) | 1,708 (2.3) | 6,354 (5.4) |
| Noc registered | 7,090 (1.3) | 2,814 (1.7) | 1,521 (1.2) | 580 (1.1) | 825 (1.1) | 1,350 (1.1) |
| Nominal number of diagnosed individuals, percentage within age strata in parentheses. Index: time of identification. | ||||||
The Capital Region of Denmark consistently had a higher ratio of individuals diagnosed by a privately practising dermatologist, across all age strata. Similarly, the Region of Southern Denmark had the highest rate of diagnosis associated with a hospital contact for all age groups younger than 18.
Regional variation in incidence
The annual incidence rates are illustrated in Fig. 1, with annual age-adjusted incidence rates provided in Table III. The crude regional incidence rates ranged from 170–283 per 100,000. After age standardizing the incidence rates, the range was 178–276 per 100,000. A persistent variation in incidence rates was observed, with the Region of Central Denmark reporting the highest incidence rates in 11 out of the 14 study years. In the remaining 3 years, this region had the second highest incidence rates. Conversely, the Region of Northern Denmark consistently recorded the lowest incidence rates in 12 out of 14 study years. On average, the Region of Central Denmark exhibited annually 18% higher than the national average. When considering age-standardized incidence rates, the average annual difference was 12%.
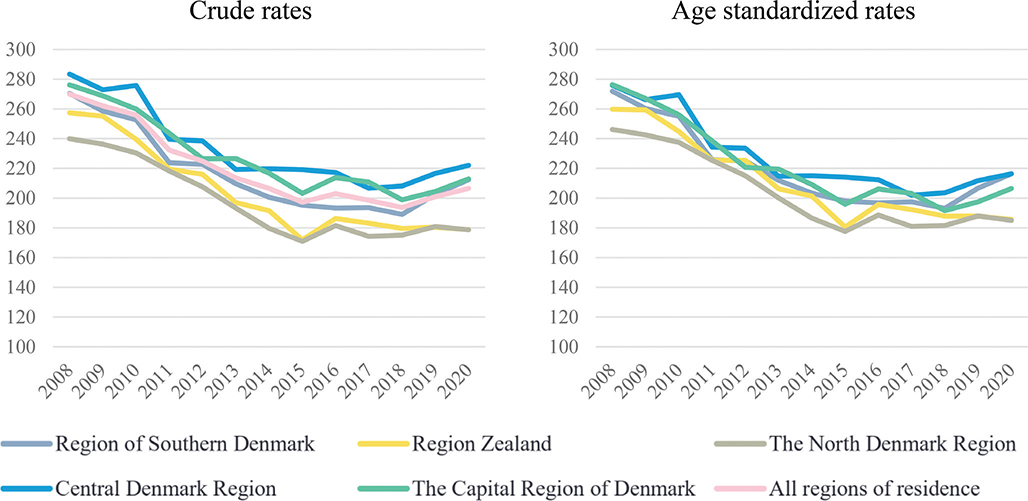
Fig. 1. Overall annual incidence rates (per 100,000 inhabitants), crude and standardized (2008–2020).
Age-stratified incidence rates are presented in Fig. 2. The regional variation in incidence of AD is less pronounced when analysed by age groups compared with the overall rates. In the adult population (18+ years), Region Zealand is the only region with consistently higher incidence rates of AD. This trend may be linked to the relatively low incidence rates observed in Region Zealand among the younger age groups. Additionally, while the Region of Central Denmark ranks among the highest across all age groups, it is particularly notable for the 6–11-year-old age group.
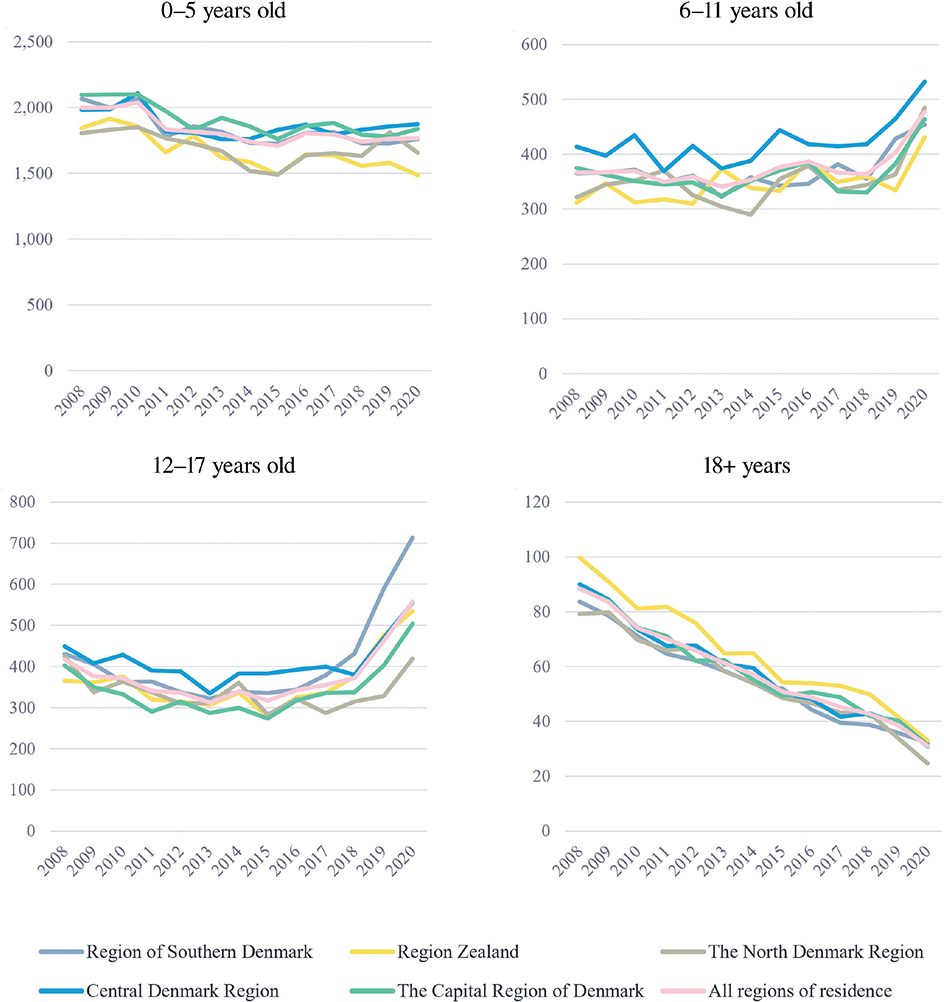
Fig. 2. Annual incidence rates (per 100,000 inhabitants) stratified by age groups.
Treatment intensification
Table IV presents the ratio of individuals with at least 1 AD-related hospital contact, while Fig. 3 illustrates the ratio of individuals receiving advanced treatment relative to the national average. The Region of Southern Denmark stands out, with the proportion of individuals having a hospital consultation being nearly twice as high as other regions (12.5%). However, this high consultation rate does not correspond to a similarly elevated frequency of advanced treatment, as the Region of Southern Denmark deviates by less than 20% from the national average in terms of advanced treatments.
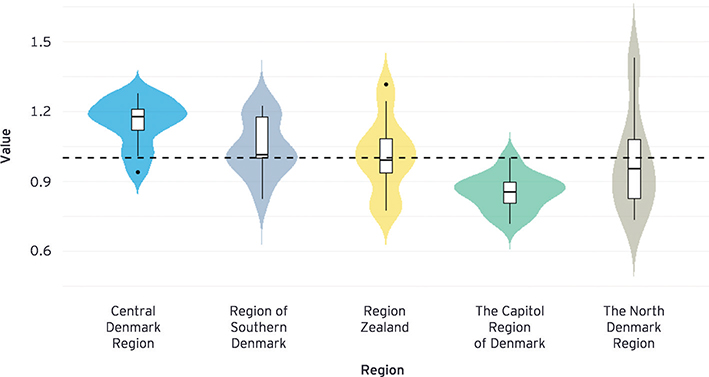
Fig. 3. Distribution of advanced treatment rates in the years 2008–2020, relative to national average (black dashed line), presented as box-plots with highlighted density areas.
In the Region of Northern Denmark, only 5.2% of the incident population have a hospital contact during the study period. This region exhibits the largest variation in annual treatment rates. The mean treatment rate in the Region of Northern Denmark reflects the national average; however, this is due to 2 outliers in 2014 and 2018 (1.43 and 1.38), respectively.
Finally, in the Region of Central Denmark and the Capital Region the hospital treatment rate is 7.5% and 9.4%, respectively. Despite the relatively similar hospital treatment rates, the Region of Central Denmark provides advanced treatment more frequently than the national average in all years, except 1, while the Capital Region is consistently providing a lower rate of advanced treatment in all years.
DISCUSSION
Recent advances in identifying AD cases in Danish register data have enabled the investigation of regional variations in number of patients with and treatment of AD. In this study, evidence of regional variations in the incidence of AD across Danish hospital regions has been provided. Although the annual relative differences in incidence of AD across Danish hospital regions are modest, they are consistent over time, leading to a substantial cumulative effect on prevalence. Additionally, significant differences were observed in the proportion of individuals receiving hospital care and advanced treatment. Variation in incidence rates was more pronounced within specific age-related strata compared with the overall population. This is expected, as regional variation tends to increase when the patient population decreases. However, in this case, the evidence suggests a diagnostic delay, particularly in the region of Zealand.
Both environmental and hereditary factors contribute to AD. However, with nearly 10% of the Danish population diagnosed during the study period, the law of large numbers suggests that the persistent differences in incidence rates over time, as shown in Fig. 1, should not occur. The variation in hospital care rates is particularly noteworthy. For instance, in the Region of Southern Denmark, the admission rate among children appears relatively high compared with other regions. However, this is explained by a different referral practice in the Region of Southern Denmark, as it is an explicit practice that all children with moderate-to-severe AD are referred to a hospital. Conversely, the Region of Northern Denmark may allocate fewer resources to AD treatment, as it consistently has the lowest proportion of individuals receiving hospital care. However, the establishment of a new dermatological department in 2020 may help align the Region of Northern Denmark with other regions in the future.
The results presented are descriptive, and it remains unknown whether the observed regional variation is associated with patient outcomes. Consequently, it cannot be determined whether this variation is warranted or unwarranted. Previous studies, however, have highlighted a diminishing marginal effect on patient outcomes as treatment rates increase – a concept known as flat-of-the-curve medicine (17, 18). Future studies should therefore investigate the health outcomes associated with advanced AD treatment, focusing on the relationship between incidence rates, specialist density of specialists per capita, and hospital contact rates.
For instance, in the capital region of Denmark relatively more patients were diagnosed by a medical specialist in dermatology, with 43.5% diagnosed by either a private dermatologist or at a hospital (see Table II). The region’s higher density of private dermatologists likely lowers the threshold for referrals from general practitioners (18). As a result, the number of AD diagnoses may be higher in the capital region, which could significantly impact health outcomes.
The registries utilized do not contain information regarding the severity of AD. Consequently, the observed variation in the utilization of advanced therapies cannot be linked to differences in disease severity. Nonetheless, it is important to note that the initiation of biologics and JAK inhibitors adheres to the treatment recommendations and guidelines issued by the Danish Medicines Council. All 5 regions comply with these guidelines, thereby ensuring a uniform treatment approach across Denmark.
Apart from the uniform use of biologics and JAK inhibitors, it cannot be ruled out that the variation in advanced (systemic) treatment and the differences in access to hospital care may have clinical significance for patients. However, additional factors such as healthcare-seeking behaviour and patient adherence to treatment also play a role.
Strengths and weaknesses
We observed an increase in AD incidence among children aged 6–17 in 2020, which is suspected to be linked to the COVID-19 pandemic. The widespread use of antibacterial hand sanitizers and increased hand washing may have caused dry skin and rashes that could be misdiagnosed as AD or alleviated by AD-related treatments. Additionally, hand sanitizer use may have exacerbated existing AD, leading to an increased need for advanced treatment. It is important to note that the algorithm used to identify children with AD was developed before the pandemic and did not account for these anomalies.
By the end of 2020, 457,876 individuals identified with AD were alive and resident in Denmark (prevalence estimate). This figure corresponds to 8%, and this estimate is in line with findings reported by Vinge et al. (2024), who estimate a lifetime prevalence of AD of 9% (19).
The definition and estimation of the incidence date of AD as either the date of the first registered diagnosis code for AD or the date of the first collection of AD-related dermatological medication, based on the specified identification criteria, are associated with uncertainty. This is because the true incidence of AD in the majority of patients is likely to be earlier. However, determining the correct incidence date, particularly for mild-to-moderate atopic dermatitis (AD), is difficult when using registry data. As stated, it should be noted that a relatively large number of adult individuals were identified with AD in the initial years of the study period, indicating that these individuals probably met the inclusion criteria at a younger age prior to this. Therefore, the reported mean age at incidence should be interpreted with caution.
Another assumption in the study is that AD persists from incidence to end of study period. Given the extended follow-up period, it is likely that some individuals become symptom free during this time. Although this could not be investigated directly, it is acknowledged that it may have influenced the findings, particularly the proportion of individuals receiving advanced treatment.
A limitation of this study is the inability to determine with statistical certainty whether the observed variations in outcomes are due to chance or represent systematic differences. However, the consistent patterns of high/low treatment rates over time have been referred to in related literature as “surgical signatures”, which are typically considered indicative of unwarranted regional variation (20).
Policy implications
Whilst the degree of regional variation in incidence rates is modest, the persistency of the variation over time should be addressed. Furthermore, the observed variation in the proportion of individuals with hospital contacts, as well as in the use of advanced treatment, highlights a lack of consensus among Danish physicians regarding the perception and management of AD.
To reduce unwarranted regional variation, it is essential to minimize diagnostic uncertainty and provide clearer guidance on when and how to treat AD.
Conclusion
Regional variation in the incidence of AD was observed. While the differences across regions are not substantial, the persistent patterns of high and low incidence rates warrant further attention. Additionally, there is clear evidence of regional variation in the proportion of AD cases managed in hospitals, and the proportion receiving advanced treatment for their condition.
ACKNOWLEDGEMENTS
IRB approval status: The data that support the findings of this study are available from Statistics Denmark’s Research Service. The study was complied with the regulations and instructions set up by Statistics Denmark. We used only anonymized data and present data only in aggregate and anonymous form. We did not contact or require any active participation from study participants. Ethics committee approval and written informed consent are not required for register-based research, according to Danish law.
REFERENCES
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Pain is a common and burdensome symptom of atopic dermatitis in United States adults. J Allergy Clin Immunol Pract 2019; 7: 2699–2706. https://doi.org/10.1016/j.jaip.2019.05.055
- Yu SH, Attarian H, Zee P, Silverberg JI. Burden of sleep and fatigue in US adults with atopic dermatitis. Dermatitis 2016; 27: 50–58. https://doi.org/10.1097/DER.0000000000000161
- Blome C, Radtke MA, Eissing L, Augustin M. Quality of life in patients with atopic dermatitis: disease burden, measurement, and treatment benefit. Am J Clin Dermatol 2016; 17: 163–169. https://doi.org/10.1007/s40257-015-0171-3
- Ali F, Vyas J, Finlay A. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol 2020; 100: 330–340. https://doi.org/10.2340/00015555-3511
- Åberg N, Hesselmar B, Åberg B, Eriksson B. Increase of asthma, allergic rhinitis and eczema in Swedish schoolchildren between 1979 and 1991. Clin Exp Allergy 1995; 25: 815–819. https://doi.org/10.1111/j.1365-2222.1995.tb00023.x
- Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess 2019; 8: 126–128. https://doi.org/10.1080/21556660.2019.1619570
- Sibbald C, Drucker AM. Patient burden of atopic dermatitis. Dermatol Clin 2017; 35: 303–316. https://doi.org/10.1016/j.det.2017.02.004
- Mortz CG, Lauritsen JM, Bindslev-Jensen C, Andersen KE. Prevalence of atopic dermatitis, asthma, allergic rhinitis, and hand and contact dermatitis in adolescents. The Odense Adolescence Cohort Study on Atopic Diseases and Dermatitis. Br J Dermatol 2001; 144: 523–532. https://doi.org/10.1046/j.1365-2133.2001.04078.x
- Mortz CG, Andersen KE, Dellgren C, Barington T, Bindslev-Jensen C. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence and comorbidities. Allergy 2015; 70: 836–845. https://doi.org/10.1111/all.12619
- Henriksen L, Simonsen J, Haerskjold A, Linder M, Kieler H, Thomsen SF, et al. Incidence rates of atopic dermatitis, asthma, and allergic rhinoconjunctivitis in Danish and Swedish children. J Allergy Clin Immunol 2015; 136: 360–366. https://doi.org/10.1016/j.jaci.2015.02.003
- Liljendahl MS, Ibler K, Vestergaard C, Skov L, Jain P, Rudolfsen JH. Identifying mild-to-moderate atopic dermatitis using a generic machine learning approach: a Danish National Health Register Study. Acta Derm Venereol 2025; 105: adv42250. https://doi.org/10.2340/actadv.v105.42250
- Wennberg JE. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ 2002; 325: 961–964. https://doi.org/10.1136/bmj.325.7370.961
- Birkmeyer JD, Reames BN, McCulloch P, Carr AJ, Campbell WB, Wennberg JE. Understanding of regional variation in the use of surgery. Lancet 2013; 382: 1121–1129. https://doi.org/10.1016/S0140-6736(13)61215-5
- Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health 2011; 39: 30–33. https://doi.org/10.1177/1403494811401482
- Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health 2011; 39: 38–41. https://doi.org/10.1177/1403494810394717
- Andersen JS, Olivarius NDF, Krasnik A. The Danish National Health Service Register. Scand J Public Health 2011; 39: 34–37. https://doi.org/10.1177/1403494810394718
- Enthoven AC. Cutting cost without cutting the quality of care. N Engl Journal Med 1978; 298: 1229–1238. https://doi.org/10.1056/NEJM197806012982204
- Islam MK, Kjerstad E. The ambiguous effect of GP competition: the case of hospital admissions. Health Econ 2017; 26: 1483–1504. https://doi.org/10.1002/hec.3439
- Vinge AS, Skov L, Johansen JD, Quaade AS. Atopic dermatitis and hand eczema in Danish adults: a nationwide population-based study. Contact Dermatitis 2025; 92: 21–30. https://doi.org/10.1111/cod.14691
- Weinstein JN, Bronner KK, Morgan TS, Wennberg JE. Trends and geographic variations in major surgery for degenerative diseases of the hip, knee, and spine: is there a roadmap for change? Health Aff (Millwood) 2004; 23: VAR81–VAR89. https://doi.org/10.1377/hlthaff.var.81