ORIGINAL REPORT
Successful Dose Reduction of Janus-kinase Inhibitors in Well-controlled Atopic Dermatitis: A Prospective, Multicentre, Real-world Study
Anne R. SCHLÖSSER1, Anouk G.M. CARON2# , Merle. S. DEN OUDEN1#, Sara J. BAART3, Louise A.A. GERBENS2, Phyllis I. SPULS2, Tamar E.C. NIJSTEN1, Renske SCHAPPIN1 and DirkJan HIJNEN1
, Merle. S. DEN OUDEN1#, Sara J. BAART3, Louise A.A. GERBENS2, Phyllis I. SPULS2, Tamar E.C. NIJSTEN1, Renske SCHAPPIN1 and DirkJan HIJNEN1
1Department of Dermatology, Erasmus University Medical Center, Rotterdam, 2Department of Dermatology, Amsterdam University Medical Center, Amsterdam, and 3Department of Biostatistics, Erasmus University Medical Center, Rotterdam, the Netherlands
#Contributed equally.
Janus kinase 1 (JAK1) inhibitors are effective for atopic dermatitis, but carry risks of adverse events. Dose reduction may mitigate these risks, although real-world evidence of dose reduction strategies is limited. This prospective, real-world study investigated JAK1 inhibitor dose reduction among 60 adults with controlled atopic dermatitis treated with abrocitinib or upadacitinib for ≥ 3 months. Doses were halved or administered every other day, as capsules cannot be split. Patients could resume their original dose if needed. The primary outcome was the proportion of patients maintaining the reduced dose at week 12. Secondary outcomes included physician- and patient-reported measures at baseline, and weeks 4, 8, and 12, analysed using linear mixed-effects models. At week 12, 80% (48/60) maintained the reduced dose. All outcomes remained within treat-to-target goals for atopic dermatitis at week 12, except for POEM (mean 8.87, 95% CI 7.43–10.31). While disease activity was significantly increased at week 8, no changes were seen at week 12. Absolute changes did not exceed the minimal clinically important difference. All 8 patients who resumed their initial dose regained disease control at week 12. In conclusion, JAK1 inhibitor dose reduction was feasible in 80% of patients without a clinically meaningful increase in disease activity.
SIGNIFICANCE
This study looked at whether people with well-controlled eczema could safely reduce their dose of JAK1 inhibitor medication in daily practice. Sixty patients lowered their dose of abrocitinib or upadacitinib under medical supervision. After 12 weeks, 80% of them stayed on the lower dose without losing control of their disease. Some symptoms increased slightly but not enough to be considered clinically relevant. Those who returned to their original dose regained disease control. These results suggest that reducing the dose of JAK1 inhibitors is possible, which may lower the risk of side effects and decrease long-term medication use.
Key words: dermatitis; atopic; dose–response relationship; drug; Janus kinase inhibitors; treatment outcome.
Citation: Acta Derm Venereol 2025; 105: adv44165. DOI: https://doi.org/10.2340/actadv.v105.44165.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 20, 2025. Accepted after revision: Oct 2, 2025. Published: Nov 17, 2025.
Corr: DirkJan Hijnen, Department of Dermatology, Erasmus University Medical Center, Dr. Molewaterplein 40, NL-3015 GD, Rotterdam, The Netherlands. E-mail: d.hijnen@erasmusmc.nl
Competing interests and funding: AS: none. AC: served as a sub-investigator in clinical trials and observational studies for AbbVie and Janssen and as a sub-investigator for the TREAT NL/BE registry. MdO: none. LG: is one of the main investigators of the TREatment of ATopic eczema, the Netherlands/Belgium registry (TREAT NL/BE) registry, which receives departmental independent research grants from pharmaceutical industries since December 2019, and is member of the TREAT Registry Taskforce Executive Committee, which receives research grants from pharmaceutical industries. PS: is Chief Investigator of the TREAT NL/BE registry, which receives departmental independent research grants from pharmaceutical industries since December 2019, is involved in performing clinical trials with many pharmaceutical industries that manufacture drugs used for the treatment of, e.g., psoriasis and atopic dermatitis, for which financial compensation is paid to the department/hospital. RS: none. SB: none. TN: none. DJH: investigator for AbbVie, Almirall, LEO Pharma, AstraZeneca, Galderma, Novartis, and Sanofi; consultancies for AbbVie, AstraZeneca, Janssen, LEO Pharma, Lilly, Novartis, Pfizer, and Sanofi.
INTRODUCTION
In recent years, several new but expensive drugs have been registered for the treatment of atopic dermatitis (AD) (1). Janus kinase (JAK) inhibitors, which target the JAK-signal transducer and activator of transcription (STAT) pathway, have demonstrated efficacy and safety in the treatment of AD up to 16 weeks. Abrocitinib and upadacitinib selectively inhibit JAK1, whereas baricitinib inhibits both JAK1 and JAK2 (2–7). Abrocitinib and upadacitinib are the most frequently prescribed JAK inhibitors in daily practice based on their superior effectiveness in clinical trials and daily practice studies (8–12). For the long-term treatment of AD, a standard daily dose of 100–200 mg abrocitinib or 15–30 mg upadacitinib is recommended, depending on disease activity (13, 14). As standard doses may result in overtreatment in a subset of patients, it is important to investigate dose reduction of JAK inhibitors to personalize treatment, reduce adverse events (AEs), and keep healthcare affordable (15–18). Evidence suggests that reducing the dose of JAK inhibitors may help reduce AEs (16, 18, 19), and a study in rheumatoid arthritis (RA) found that baricitinib dose reduction was successful in 76% of patients with controlled disease (20). To our knowledge, no real-world studies have investigated JAK inhibitor dose reduction in AD and its impact on disease control. As a result, there are no protocols that describe a structured dose reduction regimen for JAK inhibitors in AD patients. Therefore, the aim of this study is to investigate JAK1 inhibitor dose reduction and the impact on disease activity in patients with well-controlled AD in daily practice.
MATERIALS AND METHODS
Patient population
This prospective, observational, multicentre study included adult patients with moderate-to-severe well-controlled disease AD treated with a JAK1 inhibitor (abrocitinib or upadacitinib). Patients were included between April 2023 and August 2024 at the dermatology outpatient clinic of the Erasmus University Medical Center in Rotterdam, and the Amsterdam University Medical Center, the Netherlands. Most patients were already participants in the TREatment of ATopic eczema, the Netherlands/Belgium (TREAT NL/BE) registry (treatregister.nl), which collects daily practice data to investigate (cost-) effectiveness and safety of systemic immunomodulating therapies and phototherapy in AD (21). Patients were eligible for inclusion if they were aged ≥ 18 years, had a history of chronic moderate-to-severe AD (22), were treated with a JAK1 inhibitor for ≥ 3 months and if disease was well controlled (Appendix S1). Well-controlled disease was defined as an Eczema Area and Severity Index (EASI; 0–72) ≤ 7, or a Numeric Rating Scale Peak Pruritus past 24 h (NRS Peak Pruritus; 0–10) ≤ 4 (both considered as treat-to-target goals [23]), or an Atopic Dermatitis Control Tool (ADCT; 0–24) ≤ 6 (indicating mild disease activity [24, 25]). This study was approved by the local Medical Ethics Committee (MEC 2022-0717). All patients provided written informed consent.
Study design
In patients with well-controlled disease for a minimum duration of 4 weeks, the JAK1 inhibitor dose was reduced. Patients were evaluated every 4 weeks over a 12-week follow-up period (Appendix S2; Table SI). Abrocitinib was reduced from 200 mg daily to 100 mg daily, or from 100 mg daily to 100 mg every other day. Upadacitinib was reduced from 30 mg daily to 15 mg daily, or from 15 mg daily to 15 mg every other day. During follow-up, patients were allowed to return to their previous dose regimen if disease was uncontrolled.
Outcome measures
The primary outcome was the proportion of patients who maintained the reduced JAK1 inhibitor dose to week 12. To investigate the impact of dose reduction on disease activity, changes in physician- and patient-reported outcomes (following the Harmonising Outcome Measures for Eczema recommendations [26]) were assessed at every visit by experienced physicians and nurses, using the EASI, Investigator Global Assessment (IGA), Patient Oriented Eczema Measure (POEM), NRS Peak Pruritus, Dermatology Life Quality Index (DLQI), and ADCT. Changes from baseline to week 12 were compared with the established minimal clinically important difference (MCID) thresholds: EASI ≥ 6.6 (27); POEM ≥ 3.4 (27); NRS Peak Pruritus ≥ 3 (28); DLQI ≥ 4 (29); ADCT ≥ 5 (30). Additionally, treat-to-target criteria for AD were evaluated at week 12: EASI ≤ 7, POEM ≤ 7, NRS Peak Pruritus ≤ 4, DLQI ≤ 5 (23), and ADCT ≤ 6 (24, 25).
To investigate whether patients on a reduced dose experienced JAK1 inhibitor-related AEs, altered their weekly use of topical corticosteroid (TCS) use by potency (class I, mild; class II, moderate; class III, potent; class IV, very potent), or changed their healthcare utilization, these outcomes were analysed at week 12 and compared with baseline. Healthcare utilization includes consultations, (non)-prescribed medication for AD complications, work absenteeism, and out-of-pocket costs.
In patients who returned to their previous dose due to inadequate disease control during the 12-week follow-up period, regained disease control (EASI ≤ 7, or NRS Peak Pruritus ≤ 4, or ADCT ≤ 6) was assessed at week 12. Four patients who returned to their previous dose at week 12 were excluded from this analysis, because no data were available after week 12. Additionally, baseline disease severity was compared between patients who returned to their previous dose and those who maintained the reduced dose to week 12, to determine whether initial disease activity may have influenced treatment outcomes.
Statistical analyses
Statistical analyses and figures were performed using the R statistical software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria) and IBM SPSS Statistics for Windows (version 28.0.1.0; IBM Corp, Armonk, NY, USA). Patients who provided data for at least 1 time point after the start of dose reduction were included in the analyses. Descriptive statistics were used to summarize data. Differences were assessed using Fisher’s exact test and the Mann–Whitney U test. The primary outcome was determined by assessing the proportion of patients who achieved JAK1 inhibitor dose reduction at week 12. Linear mixed-effects models with random intercept and screening data were used to evaluate changes in all continuous outcomes. Data from all patients were included in the analysis at baseline. A time-varying covariate was included in our model to indicate whether a patient was on the reduced dose or had returned to their previous dose regimen due to loss of disease control. If a patient returned to their previous regimen, observations up to that timepoint were included in the analyses. Natural cubic splines were used to model the nonlinear association over time. When necessary, square root transformations were applied to improve model diagnostics, with values back transformed to the original scale for interpretation. Plots were generated to visualize estimated marginal means (EMMs), with horizontal lines indicating thresholds for mild disease activity and treat-to-target goals for AD. A p-value < 0.05 was considered statistically significant. A continuation ratio model (CRM) in the forward formulation was used to analyse IGA. Log odds were transformed to probabilities for interpretation, with effect plots showing the probability of each IGA score over time. An IGA ≤ 2 indicates mild disease (31). Missing data were rare (< 5% of observations) and assumed to be missing completely at random (MCAR). No imputation was performed. This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines (32). Refer to Appendices S3–S6 for additional methods.
RESULTS
Patient characteristics
A total of 63 patients were included in this study. All patients maintained disease control for at least 4 weeks following screening, thereby meeting the criteria for JAK1 inhibitor dose reduction Three patients who were lost to follow-up were excluded from the analysis. Therefore, 60 patients (Erasmus University Medical Center: n = 55, Amsterdam University Medical Center: n = 5) were included in the final analysis. At baseline, 3 (5%) and 10 (17%) patients were treated with abrocitinib 100 mg daily and abrocitinib 200 mg daily, respectively. For upadacitinib, 27 (45%) patients were treated with 15 mg daily and 20 (33%) with 30 mg daily (Fig. 1). At baseline, the median duration of JAK1 inhibitor treatment was 10.5 months (IQR 4.3–21.8). Some 55% of the patients were female, with a median age of 32.0 years (IQR 26.3–44.5). Most patients had Fitzpatrick skin type II (62%). Atopic comorbidities, including asthma (50%), allergic conjunctivitis (23%), and allergic rhinitis (65%), were reported. All patients were previously treated with systemic immunosuppressants, and 53% had used at least 3 different systemic treatments. No significant differences in baseline disease severity scores were observed (Table I, Appendix S7, Table SII). Doses were reduced to abrocitinib 100 mg once daily (n = 10), abrocitinib 100 mg every other day (n = 3), upadacitinib 15 mg once daily (n = 20) and upadacitinib 15 mg every other day (n = 27) (Fig. 1). The primary reason patients reported for participating in this study was their fear of AEs or the presence of existing AEs (43%).
| Characteristic | Total (n = 60) | Reduced dose at week 12a (n = 48) | Returned to previous dose at week 12b (n = 12) | p-value |
| Age at the start dose reduction (years), median (IQR) | 32.0 (26.3–44.5) | 31.6 (25.0–42.8) | 35.5 (27.3–47.3) | 0.421 |
| Female, n (%) | 33 (55) | 27 (56) | 6 (50) | 0.754 |
| Fitzpatrick skin type, n (%) | 0.719 | |||
| I | 1 (2) | 1 (2) | 0 (0) | |
| II | 37 (62) | 29 (60) | 8 (67) | |
| III | 7 (12) | 5 (10) | 2 (17) | |
| IV | 8 (13) | 7 (15) | 1 (8) | |
| V | 4 (7) | 3 (6) | 1 (8) | |
| VI | 3 (5) | 3 (6) | 0 (0) | |
| BMI, median (IQR) | 26.0 (22.9–29.4) | 25.8 (22.6–29.1) | 26.8 (24.1–30.6) | 0.355 |
| Atopic comorbidity, n (%) | ||||
| Asthma | 30 (50) | 24 (50) | 6 (50) | 1.000 |
| Allergic conjunctivitis | 14 (23) | 12 (25) | 2 (17) | |
| Allergic rhinitis | 39 (65) | 31 (65) | 8 (67) | 1.000 |
| Family history of atopic diseasec, n (%) | 40 (67) | 34 (71) | 6 (50) | 0.189 |
| Baseline JAK1 inhibitor treatment | ||||
| Abrocitinib 100 mg, n (%) | 3 (5) | 2 (4) | 1 (8) | |
| Abrocitinib 200 mg, n (%) | 10 (17) | 8 (17) | 2 (17) | |
| Upadacitinib 15 mg, n (%) | 27 (45) | 21 (44) | 6 (50) | 0.754 |
| Upadacitinib 30 mg, n (%) | 20 (33) | 17 (35) | 3 (25) | |
| Duration of JAK1 inhibitor treatment (months), median (IQR) | 10.5 (4.3–21.8) | 10.0 (4.3–19.0) | 11.5 (4.3–23.5) | 0.788 |
| Previous systemic immunosuppressants, n (%) | ||||
| Cyclosporin A | 46 (77) | 35 (73) | 11 (92) | 0.262 |
| Methotrexate | 23 (38) | 18 (38) | 5 (42) | 1.000 |
| Azathioprine | 7 (12) | 5 (10) | 2 (17) | |
| Mycophenolic acid/mycophenolate mofetil | 13 (22) | 10 (21) | 3 (25) | |
| Dupilumab | 44 (73) | 34 (71) | 10 (83) | 0.486 |
| Tralokinumab | 4 (7) | 4 (8) | 0 (0) | |
| JAK inhibitord | 16 (27) | 11 (23) | 5 (42) | 0.273 |
| ≥ 3 previous used systemic treatments | 32 (53) | 23 (48) | 9 (75) | 0.115 |
| UVB phototherapy | 27 (45) | 21 (44) | 6 (50) | 0.754 |
| Disease severity outcomes | ||||
| EASI, median (IQR) | 1.6 (0.8–2.6) | 1.6 (0.8–2.1) | 2.0 (0.7–4.4) | 0.415 |
| IGA, n (%) | 0.854 | |||
| Clear | 2 (3) | 1 (2) | 1 (8) | |
| Almost clear | 42 (70) | 35 (73) | 7 (58) | |
| Mild | 15 (25) | 11 (23) | 4 (33) | |
| Moderate | 1 (2) | 1 (2) | 0 (0) | |
| Severe | 0 (0) | 0 (0) | 0 (0) | |
| POEM, median (IQR) | 4.0 (1.3–8.0) | 4.0 (1.3–8.5) | 6.0 (1.8–8.0) | 0.414 |
| NRS Peak Pruritus, median (IQR) | 2.0 (0.3–3.0) | 2.0 (0.0–3.0) | 2.5 (1.0–3.8) | 0.475 |
| DLQI, median (IQR) | 2.0 (1.0–4.0) | 1.5 (0.3–4.0) | 2.5 (1.0–4.8) | 0.413 |
| ADCT, median (IQR) | 2.0 (1.0–5.0) | 2.0 (1.0–5.0) | 4.5 (1.3–6.8) | 0.365 |
| Fisher’s exact test was used for categorical variables. Mann–Whitney U test was used for ordinal variables and continuous variables. No statistical tests were performed for outcomes with a small number of observations (n ≤ 3). A p-value of < 0.05 was considered statistically significant. aDefined as all patients who maintained their reduced dose at week 12. bDefined as all patients who returned to their previous dose regimen during the study. cIncludes atopic dermatitis, asthma, allergic rhinoconjunctivitis, atopic eye disease, eosinophilic oesophagitis. dIncludes previous use of abrocitinib, baricitinib, and/or upadacitinib. ADCT: Atopic Dermatitis Control Tool; BMI: body mass index; CI: confidence interval; DLQI: Dermatology Life Quality Index; EASI: Eczema Area and Severity Index; IGA: Investigator Global Assessment; IQR: interquartile range; JAK: Janus kinase; n: number of patients; NRS Peak Pruritus: Numeric Rating Scale Peak Pruritus for the last 24 h; POEM: Patient Oriented Eczema Measure; UVB: ultraviolet B rays. |
||||
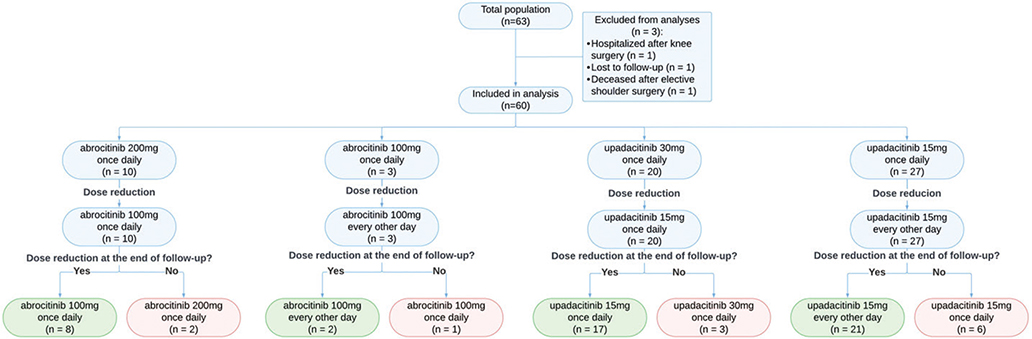
Fig. 1. Flowchart of patients. At screening, patients had been treated with a JAK1 inhibitor for a minimum of 3 months. Patients in the different dose reduction regimens are shown, as well as those who remained on the reduced dose at the end of follow-up and those who returned to their previous regimen due to inadequate disease control. n: number of patients.
Clinical effectiveness of dose reduction
At week 12, 48 out of 60 (80%) patients maintained their reduced JAK1 inhibitor dose, without returning to their previous dose regimen. Fig. 2 presents plots based on the model, illustrating the estimated mean changes in outcomes over 12 weeks. Table II gives the EMMs and their changes at different timepoints. Only the POEM score exceeded the treat-to-target goal at week 12 (8.87, 95% CI 7.43–10.31), while all other outcomes remained within the treat-to-target goals at week 12. While disease activity was significantly increased at week 8 for all outcomes, no changes were seen between weeks 8 and 12. Although increased, absolute changes (EASI 1.39; POEM 3.17; NRS Peak Pruritus 0.91; DLQI 1.35; ADCT 1.72) did not exceed the MCID between baseline and week 12. Fig. 3 shows the probabilities of IGA scores over time. The probability of achieving an IGA of 1 decreased from 70% at baseline to 50% at week 12, while the probability of an IGA of 2 increased from 30% to 40%. Additional plots by treatment status – observations during reduced dosing and after return to the previous dose – are provided in the Supplementary data (Appendix S8, Table SIII; Appendix S12–S13, Figs S1–S2).
| Follow-up time | Change in scores | |||||||||
| Baseline (n = 60) | Week 4 (n = 56) | Week 8 (n = 52) | Week 12 (n = 48) | Baseline–week 12 | Baseline–week 8 | Week 8–week 12 | ||||
| Outcome (range) | Estimate (95% CI) | Estimate (95% CI) | Estimate (95% CI) | Estimate (95% CI)a | Changeb | p-value | Change | p-value | Change | p-value |
| EASI (0–72) | 1.74 (1.30–2.23) | 2.80 (2.23–3.45) | 3.26 (2.61–3.98) | 3.13 (2.49–3.84) | 1.39 | < 0.001 | 1.52 | < 0.001 | –0.13 | 0.9189 |
| POEM (0–28) | 5.70 (4.34–7.06) | 8.20 (6.99–9.41) | 9.21 (7.99–10.44) | 8.87 (7.43–10.31) | 3.17 | < 0.001 | 3.51 | < 0.001 | –0.35 | 0.8502 |
| NRS Peak Pruritus (0–10) | 1.56 (1.14–2.04) | 2.49 (2.00–3.04) | 2.82 (2.29–3.41) | 2.46 (1.90–3.10) | 0.91 | 0.0031 | 1.27 | < 0.001 | –0.36 | 0.3190 |
| DLQI (0–30) | 1.88 (1.23–2.67) | 3.07 (2.28–3.98) | 3.56 (2.70–4.55) | 3.23 (2.31–4.30) | 1.35 | 0.0069 | 1.68 | < 0.001 | –0.34 | 0.6803 |
| ADCT (0–24) | 2.85 (2.09–3.74) | 4.49 (3.60–5.47) | 5.12 (4.16–6.17) | 4.61 (3.56–5.79) | 1.72 | 0.0042 | 2.26 | < 0.001 | –0.51 | 0.5596 |
| Estimated marginal means and their changes between timepoints with corresponding p-values. Estimated marginal means are presented on the original scale and changes are adjusted for multiple testing. A time-varying covariate was included in the model. Data from all patients were included in the analysis at baseline. If a patient returned to their previous regimen, subsequent data were excluded from analysis from that point onward. A p-value of < 0.05 was considered statistically significant. aThresholds for mild disease and treat-to-target goals for AD: EASI ≤ 7, POEM ≤ 7, NRS Peak Pruritus ≤ 4, DLQI ≤ 5, ADCT ≤ 6. bMinimal clinically important difference (MCID) definitions: EASI (≥ 6.6), POEM (≥ 3.4), NRS Peak Pruritus (≥ 3), DLQI (≥ 4), and ADCT (≥ 5). Missing data: POEM, DLQI, and ADCT scores were missing at weeks 4 and 8 (n = 2). NRS Peak Pruritus was missing at week 8 (n = 1). ADCT: Atopic Dermatitis Control Tool; CI: confidence interval; DLQI: Dermatology Life Quality Index; EASI: Eczema Area and Severity Index; n: number of patients; NRS Peak Pruritus: Numeric Rating Scale Peak Pruritus for the last 24 h; POEM: Patient Oriented Eczema Measure. |
||||||||||

Fig. 2. Estimated mean change in Eczema Area and Severity Index (EASI, 0–72). (A) Patient Oriented Eczema Measure (POEM, 0–28); (B) Numeric Rating Scale Peak Pruritus for the last 24 h (NRS Peak Pruritus, 0–10); (C) Dermatology Life Quality Index (DLQI, 0–30); and (D) Atopic Dermatitis Control Tool (ADCT, 0–24). (E) Linear-mixed effects models with cubic splines were used to model nonlinear changes over time. A time-varying covariate was included in the model. Data from all patients were included in the analysis at baseline. If a patient returned to their previous regimen, subsequent data were excluded from analysis from that point onwards. Lower scores indicate mild disease activity. Horizontal lines are shown to represent thresholds for mild disease and treat-to-target goals for AD: EASI ≤ 7, POEM ≤ 7, NRS Peak Pruritus ≤ 4, DLQI ≤ 5, ADCT ≤ 6. The light-blue area represents the 95% confidence interval (CI). EASI, NRS Peak Pruritus, DLQI, and ADCT remained within the treat-to-target goals. POEM scores exceeded the treat-to-target goal. The minimal clinically important difference (MCID) was not exceeded for all outcomes: EASI (≥ 6.6), POEM (≥ 3.4), NRS Peak Pruritus (≥ 3), DLQI (≥ 4), and ADCT (≥ 5). Missing data: POEM, DLQI, and ADCT scores were missing at week 4 and week 8 (n = 2). NRS Peak Pruritus was missing at week 8 (n = 1). n: number of patients on the reduced dose at each timepoint; CI: confidence interval.
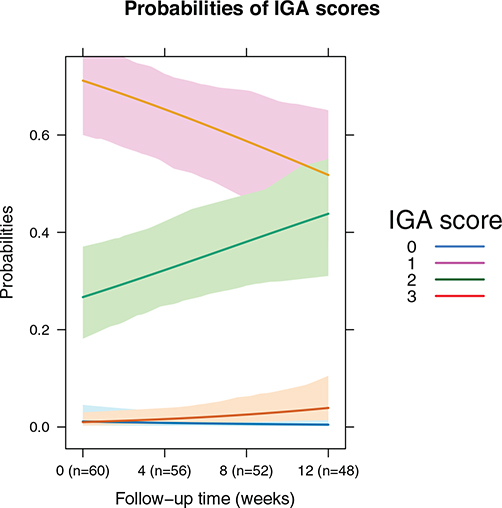
Fig. 3. IGA probabilities over time. The figure illustrates the predicted marginal probabilities for each IGA score (0, 1, 2, 3) at specified follow-up time points (baseline, week 4, week 8, week 12). The probabilities reflect the likelihood of patients being in each IGA category based on the continuation ratio model. Data from all patients were included in the analysis at baseline. If a patient returned to their previous regimen, subsequent data were excluded from analysis from that point onwards. The data indicate that the probability of having an IGA 1 decreased over time, while the probability of an IGA 2 increased. IGA score 4 is not represented, as it was not observed in the study population. Missing data: POEM, DLQI, and ADCT scores were missing at week 4 and week 8 (n = 2). NRS Peak Pruritus was missing at week 8 (n = 1). IGA: Investigator Global Assessment.
Effects of dose reduction on adverse events and topical treatment use
Among patients on a reduced dose at week 12 (n = 48), the most frequently reported AE at baseline was acne (16/48, 33%). At week 12, acne was decreased in 5 patients (31%) and in remission in 5 patients (31%) (Appendix S9, Table SIV). In addition, 21% of patients were using a higher TCS class at week 12 compared with baseline, while 13% were using a lower class. A total of 67% continued to use the same class of TCS, with 25% of these patients using the TCS more frequently: 4 patients applied their TCS on 1 additional day per week, 3 patients on 2 additional days, and 1 patient on 4 additional days.
Healthcare utilization
Among patients on a reduced dose at week 12 (n = 48), patient-reported healthcare utilization remained low at week 12 compared with baseline. Due to small samples, no statistical analyses were performed. Observationally, no clear differences were found (Appendix S10, Table SV). Additional results on AEs, TCS use, and healthcare utilization are provided in the Supporting Information (Appendix S9–S11, Table SIV–SIX).
Unsuccessful dose reduction
In total, 20% (12/60) of patients returned to their previous dose regimens, all due to inadequate disease control. There was no significant difference in sex distribution within this group, with 50% female and 50% male (p = 0.754). Four patients returned to the previous dose at week 4, 4 at week 8 and 4 at week 12. Two patients (2/12, 17%) were using abrocitinib 100 mg once daily, 1 patient (1/12, 8%) abrocitinib 100 mg every other day, 3 (3/12, 25%) patients upadacitinib 15 mg once daily, and 6 (6/12, 50%) patients upadacitinib 15 mg every other day. Among patients on an every-other-day dosing regimen (abrocitinib or upadacitinib), 23% (7/30) returned to their original dose, compared with 17% (5/30) in the daily dosing regimen (p = 0.748) (see Fig. 1). At week 12, all 8 patients who had returned to their previous dose at week 4 or 8 had regained well-controlled disease (EASI ≤ 7, or NRS Peak Pruritus ≤ 4, or ADCT ≤ 6), with 75% of patients achieving an EASI ≤ 7, 75% a NRS Peak Pruritus ≤ 4, and 75% an ADCT ≤ 6.
DISCUSSION
In this prospective observational study, we investigated JAK1 inhibitor dose reduction and its effect on disease activity in patients with well-controlled AD. After 12 weeks of dose reduction, 80% of patients maintained their reduced dose. Most disease severity outcomes remained within the treat-to-target goals for AD at week 12. Although there was a deterioration in all disease severity outcomes, the MCID between baseline and week 12 was not exceeded, suggesting limited clinical relevance. In total, 20% of patients returned to their previous regimen. All patients who returned before week 12 regained well-controlled disease. This suggests that dose reductions can be safely attempted, as disease control can be achieved by returning to the previous dose regimen.
Takeuchi et al. also reported significant increases in disease activity outcomes with baricitinib dose reduction from 4 mg to 2 mg in 975 rheumatoid arthritis patients. However, also in these patients, most remained within the defined parameters of disease control. The rate of unsuccessful dose reduction was 18%, and most patients were able to recapture control after returning to their previous regimen (20). These findings are in line with our study.
The EMMs at week 12 were within the treat-to-target goals for AD, except for POEM. This patient-reported questionnaire measures patient-perceived AD severity by assessing symptoms such as itch, sleep, bleeding, oozing, cracking, flaking, and dry skin (33). In our study, the highest-scoring sub-questions were those related to itch and dry skin. Interestingly, most patients already had high baseline POEM scores. At week 12, the estimated mean was 8.87, which marks the lower threshold for moderate disease classification (8–16) (34). Despite this, during shared decision-making, patients were willing to continue the reduced dose rather than return to their previous dose regimen, even with higher disease severity scores. A higher POEM compared with lower scores on other outcomes suggests that patients may experience persistent AD symptoms, but these have a limited impact on quality of life (DLQI) and disease control (ADCT).
Acne was the most frequently reported JAK1 inhibitor-related AE (n = 16) at baseline in patients on a reduced dose at week 12, with 63% (10 out of 16 patients) experiencing improvement or complete remission at week 12. These results are in line with previous studies, including a meta-analysis of 11,396 patients with various dermatological conditions treated with JAK inhibitors, which showed higher odds ratios for acne at higher doses of upadacitinib and abrocitinib (35). Additionally, Takeuchi et al. (20) found that dose reduction was associated with a lower rate of non-serious infections (30.6 per 100 patient-years for baricitinib 4 mg vs 24.9 for 2 mg). Similarly, our study observed a trend of fewer infections after dose reduction. However, the sample size is too small and the duration too short to draw definitive conclusions. The primary reason patients reported for participating in this study was their fear of AEs or the presence of existing AEs (43%), highlighting the importance of dose reduction to improve patient well-being.
Besides its potential impact on AEs, dose reduction may also offer cost-saving benefits, particularly with an every-other-day dosing regimen, although, from a pharmacological perspective, reducing the dose of JAK inhibitors to an every-other-day regimen may seem irrational given the short half-lives of abrocitinib (5 h) and upadacitinib (9–14 h) (36, 37). Our study suggests that an every-other-day regimen may be a feasible option for remaining disease control. In our study, all patients reported that they remained compliant, although adherence was not objectively measured. Nonetheless, it is essential to educate patients on the correct use of the dosing regimen and offer tools to increase adherence.
A psychological benefit of dose reduction is that it may affect the patients’ experience of AD. The “less is more” principle suggests that taking less medication may reduce self-awareness or focus on the disease, thereby improving quality of life. Psychologist Leventhal developed the Illness Perception Model, highlighting the relationship between perceived illness, treatment, and quality of life (38). Reducing medication dosage, when possible, can shift the focus away from the disease and improve quality of life.
Strengths and limitations
The key strength of this study is that it fills an evidence gap on JAK1 inhibitor dose reduction in daily practice, with potential implications for improving cost-efficiency in healthcare. Several limitations should be acknowledged. The absence of a randomized controlled design and blinding, as well as the relatively small sample size and academic patient populations, may impact the generalizability of our findings. Future studies should include a larger patient population and explore disease stability between different dose reduction strategies, such as daily dosing and every-other-day dosing, as well as variations between different JAK inhibitors. Moreover, the limited study duration restricts the ability to draw conclusions on long-term outcomes. Because AD is a chronic yet fluctuating disease, assessing long-term disease control is crucial using continuous real-world data collection, such as the TREAT Registry Taskforce registries or the BioDay Registry (21, 39).
Future directions
Given that AD is a chronic and fluctuating disease, a flexible dosing strategy may be beneficial. Some patients may require higher doses during disease flares and lower doses during stable periods. If no other (severe) AEs are present, it could be beneficial to give patients more autonomy in adjusting their dosage to keep AD under control. More autonomy allows patients to gain better control over their disease, making them feel more confident in managing their AD, which may lead to improved treatment outcomes. Future studies should focus on long-term outcomes of dose reduction and explore individualized and flexible dosing strategies such as the use of JAK inhibitors “as needed”. Similar developments have recently been seen with the use of inhaled corticosteroids/formoterol on an as-needed basis for the treatment of chronic asthma (40). Furthermore, identifying predictors of response to JAK1 inhibitor dose reduction is needed to optimize personalized treatment.
Conclusion
Our findings indicate that JAK1 inhibitor dose reduction is a feasible and well-tolerated strategy for many patients with well-controlled AD, with minimal impact on disease activity and a trend toward a favourable safety profile. Although a small subset of patients required a rescue to the original dose, they successfully regained disease control after resuming their previous dose regimen. Overall, dose reduction in well-controlled AD appears to be a viable strategy worth considering.
ACKNOWLEDGEMENTS
The authors would like to thank all patients for their participation in this study and express their gratitude to Linda Paine for her assistance in its coordination.
IRB approval status: Our study was reviewed and approved by the Institutional Review Board of Erasmus Medical Center (MEC-2022-0717).
REFERENCES
- NVDV. Conventionele systemische immunosuppressieve therapie CE. Utrecht: NVDV, 2019.
- Eichenfield LF, Flohr C, Sidbury R, Siegfried E, Szalai Z, Galus R, et al. Efficacy and safety of abrocitinib in combination with topical therapy in adolescents with moderate-to-severe atopic dermatitis: the JADE TEEN randomized clinical trial. JAMA Dermatol 2021; 157: 1165–1173. https://doi.org/10.1001/jamadermatol.2021.2830
- Guttman-Yassky E, Teixeira HD, Simpson EL, Papp KA, Pangan AL, Blauvelt A, et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): results from two replicate double-blind, randomised controlled phase 3 trials. Lancet 2021; 397: 2151–2168. https://doi.org/10.1016/S0140-6736(21)00588-2
- Reich K, Kabashima K, Peris K, Silverberg JI, Eichenfield LF, Bieber T, et al. Efficacy and safety of baricitinib combined with topical corticosteroids for treatment of moderate to severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol 2020; 156: 1333–1343. https://doi.org/10.1001/jamadermatol.2020.3260
- Reich K, Teixeira HD, de Bruin-Weller M, Bieber T, Soong W, Kabashima K, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2021; 397: 2169–2181. https://doi.org/10.1016/S0140-6736(21)00589-4
- Silverberg JI, Simpson EL, Thyssen JP, Gooderham M, Chan G, Feeney C, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol 2020; 156: 863–873. https://doi.org/10.1001/jamadermatol.2020.1406
- Simpson EL, Sinclair R, Forman S, Wollenberg A, Aschoff R, Cork M, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet 2020; 396: 255–266. https://doi.org/10.1016/S0140-6736(20)30732-7
- Olydam JI, Schlösser AR, Custurone P, Nijsten TEC, Hijnen D. Real-world effectiveness of abrocitinib treatment in patients with difficult-to-treat atopic dermatitis. J Eur Acad Dermatol Venereol 2023; 37: 2537–2542. https://doi.org/10.1111/jdv.19378
- Schlösser AR, Boeijink N, Olydam J, Nijsten TEC, Hijnen D. Upadacitinib treatment in a real-world difficult-to-treat atopic dermatitis patient cohort. J Eur Acad Dermatol Venereol 2024; 38: 384–392. https://doi.org/10.1111/jdv.19581
- Silverberg JI, Thyssen JP, Fahrbach K, Mickle K, Cappelleri JC, Romero W, et al. Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis. J Eur Acad Dermatol Venereol 2021; 35: 1797–1810. https://doi.org/10.1111/jdv.17351
- Wan H, Jia H, Xia T, Zhang D. Comparative efficacy and safety of abrocitinib, baricitinib, and upadacitinib for moderate-to-severe atopic dermatitis: a network meta-analysis. Dermatol Ther 2022; 35: e15636. https://doi.org/10.1111/dth.15636
- Drucker AM, Lam M, Elsawi R, Prieto-Merino D, Malek R, Ellis AG, et al. Comparing binary efficacy outcomes for systemic immunomodulatory treatments for atopic dermatitis in a living systematic review and network meta-analysis. Br J Dermatol 2024; 190: 184–190. https://doi.org/10.1093/bjd/ljad393
- NVDV. Standpunt voorschrijven upadacitinib bij volwassen patiënten en adolescenten vanaf 12 jaar met matig tot ernstig constitutioneel eczeem. 2022. Available from: https://nvdv.nl/storage/app/media/uploaded-files/NTvDV_01_2022_NVDV-Standpunt%20voorschrijven%20%20upadacitinib.pdf
- NVDV. Abrocitinib bij volwassen patienten met matig tot ernstig constitutioneel eczeem (standpunt). 2022. Avaliable from nvdv-standpunt-abrocitinib-bij-volwassen-patieenten-met-matig-tot-ernstig-constitutioneel-eczeem.pdf
- Medicijnkosten: Zorginstituut Nederland. 2023. Available from: https://www.medicijnkosten.nl/
- Chang PH, Huang SF, Chang PS, Yu Y. Safety considerations of systemic Janus kinase inhibitors in atopic dermatitis applications. J Dermatol 2021; 48: 1631–1639. https://doi.org/10.1111/1346-8138.16116
- Gao Q, Zhao Y, Zhang J. Efficacy and safety of abrocitinib and upadacitinib versus dupilumab in adults with moderate-to-severe atopic dermatitis: a systematic review and meta-analysis. Heliyon 2023; 9: e16704. https://doi.org/10.1016/j.heliyon.2023.e16704
- Simpson EL, Silverberg JI, Nosbaum A, Winthrop KL, Guttman-Yassky E, Hoffmeister KM, et al. Integrated safety analysis of abrocitinib for the treatment of moderate-to-severe atopic dermatitis from the Phase II and Phase III clinical trial program. Am J Clin Dermatol 2021; 22: 693–707. https://doi.org/10.1007/s40257-021-00618-3
- Simpson EL, Papp KA, Blauvelt A, Chu CY, Hong HC, Katoh N, et al. Efficacy and safety of upadacitinib in patients with moderate to severe atopic dermatitis: analysis of follow-up data from the Measure Up 1 and Measure Up 2 randomized clinical trials. JAMA Dermatol 2022; 158: 404–413. https://doi.org/10.1001/jamadermatol.2022.0029
- Takeuchi T, Genovese MC, Haraoui B, Li Z, Xie L, Klar R, et al. Dose reduction of baricitinib in patients with rheumatoid arthritis achieving sustained disease control: results of a prospective study. Ann Rheum Dis 2019; 78: 171–178. https://doi.org/10.1136/annrheumdis-2018-213271
- Spuls PI, Gerbens LAA, Apfelbacher CJ, Wall D, Arents BWM, Barbarot S, et al. The International TREatment of ATopic Eczema (TREAT) Registry Taskforce: an initiative to harmonize data collection across national atopic eczema photo- and systemic therapy registries. J Invest Dermatol 2017; 137: 2014–2016. https://doi.org/10.1016/j.jid.2017.05.014
- Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta DErm Venereol 1980; Suppl 92: 44–47. https://doi.org/10.2340/00015555924447
- De Bruin-Weller M, Biedermann T, Bissonnette R, Deleuran M, Foley P, Girolomoni G, et al. Treat-to-target in atopic dermatitis: an international consensus on a set of core decision points for systemic therapies. Acta Derm Venereol 2021; 101: adv00402. https://doi.org/10.2340/00015555-3751
- Chen R, Loman L, van der Gang LF, Sloot MM, de Bruin-Weller MS, Schuttelaar MLA. Assessing disease control in patients with atopic dermatitis by using the Atopic Dermatitis Control Tool in daily practice. Dermatology 2024; 240: 732–738. https://doi.org/10.1159/000541466
- Pariser DM, Simpson EL, Gadkari A, Bieber T, Margolis DJ, Brown M, et al. Evaluating patient-perceived control of atopic dermatitis: design, validation, and scoring of the Atopic Dermatitis Control Tool (ADCT). Curr Med Res Opin 2020; 36: 367–376. https://doi.org/10.1080/03007995.2019.1699516
- Stuart BL, Howells L, Pattinson RL, Chalmers JR, Grindlay D, Rogers NK, et al. Measurement properties of patient-reported outcome measures for eczema control: a systematic review. J Eur Acad Dermatol Venereol 2021; 35: 1987–1993. https://doi.org/10.1111/jdv.17335
- Schram ME, Spuls PI, Leeflang MM, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy 2012; 67: 99–106. https://doi.org/10.1111/j.1398-9995.2011.02719.x
- Reich A, Riepe C, Anastasiadou Z, Mędrek K, Augustin M, Szepietowski JC, et al. Itch assessment with visual analogue scale and numerical rating scale: determination of minimal clinically important difference in chronic itch. Acta Derm Venereol 2016; 96: 978–980. https://doi.org/10.2340/00015555-2433
- Basra MK, Salek MS, Camilleri L, Sturkey R, Finlay AY. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology 2015; 230: 27–33. https://doi.org/10.1159/000365390
- Simpson E, Eckert L, Gadkari A, Mallya UG, Yang M, Nelson L, et al. Validation of the Atopic Dermatitis Control Tool (ADCT©) using a longitudinal survey of biologic-treated patients with atopic dermatitis. BMC Dermatol 2019; 19: 15. https://doi.org/10.1186/s12895-019-0095-3
- Futamura M, Leshem YA, Thomas KS, Nankervis H, Williams HC, Simpson EL. A systematic review of Investigator Global Assessment (IGA) in atopic dermatitis (AD) trials: many options, no standards. J Am Acad Dermatol 2016; 74: 288–294. https://doi.org/10.1016/j.jaad.2015.09.062
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Initiative S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 2007; 335: 806–808. https://doi.org/10.1136/bmj.39335.541782.AD
- Williams HC, Schmitt J, Thomas KS, Spuls PI, Simpson EL, Apfelbacher CJ, et al. The HOME Core outcome set for clinical trials of atopic dermatitis. J Allergy Clin Immunol 2022; 149: 1899–1911. https://doi.org/10.1016/j.jaci.2022.03.017
- Charman CR, Venn AJ, Ravenscroft JC, Williams HC. Translating Patient-Oriented Eczema Measure (POEM) scores into clinical practice by suggesting severity strata derived using anchor-based methods. Br J Dermatol 2013; 169: 1326–1332. https://doi.org/10.1111/bjd.12590
- Chen BL, Huang S, Dong XW, Wu DD, Bai YP, Chen YY. Janus kinase inhibitors and adverse events of acne in dermatologic indications: a systematic review and network meta-analysis. J Dermatolog Treat 2024; 35: 2397477. https://doi.org/10.1080/09546634.2024.2397477
- AbbVie. Rinvoq: summary of product characteristics. European Medicines Agency (EMA), 2019: p. 47.
- Pfizer. Cibinqo: summary of product characteristics. European Medicines Agency (EMA), 2021: p. 21.
- Leventhal H, Cameron LD. The self-regulation of health and illness behaviour. Abingdon, UK: Routledge; 2003.
- BioDay Eczema and Atopic Diseases Registry. Available from: https://bioday.nl/
- Papi A, Ferreira DS, Agache I, Baraldi E, Beasley R, Brusselle G, et al. European Respiratory Society short guide-lines for the use of as-needed ICS/formoterol in mild asthma. Eur Respir J 2023; 62: 2300047. https://doi.org/10.1183/13993003.00047-2023