SHORT COMMUNICATION
Early Recurrence of Nodular Basal Cell Carcinoma Despite Negative Margins: A Case Report
Yuto YAMAMURA, Kazuyasu FUJII*, Chisa NAKASHIMA, Shunya USUI and Atsushi OTSUKA
Department of Dermatology, Kindai University Hospital, 377-2 Ohno-Higashi, Osaka-Sayama, Osaka 589-8511, Japan. *E-mail: kazuyasu.fujii@med.kindai.ac.jp
Citation: Acta Derm Venereol 2025; 105: adv44195. DOI: https://doi.org/10.2340/actadv.v105.44195.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 20, 2025. Accepted after revision: Jul 7, 2025. Published: Jul 25, 2025
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Basal cell carcinoma (BCC) exhibits considerable clinical and histopathological heterogeneity, and classification based on histological subtypes is considered useful in predicting prognosis and determining treatment strategies (1). BCC is broadly categorized into indolent and aggressive subtypes (2). Indolent subtypes are generally well circumscribed and localized, with high cure rates achieved through surgical excision. In contrast, aggressive subtypes tend to invade irregularly into the deep dermis and lateral margins, making complete excision challenging and increasing the risk of recurrence (2, 3). Given these characteristics, surgery remains the primary treatment modality for BCC, and achieving histologically negative margins is regarded as the most critical factor in preventing recurrence (4).
In the present case, local recurrence occurred shortly after initial surgery, despite histologically confirmed negative margins. Moreover, although the recurrent lesion was classified as the nodular (indolent) type, it exhibited clinically aggressive behaviour. This report discusses a BCC case with an atypical clinical course.
CASE REPORT
An elderly woman in her 80s, with a history of hyperlipidaemia and lumbar compression fracture, and without any history of immunosuppressive therapy or evidence of immunocompromise, was referred to our department for evaluation of a slowly enlarging cutaneous tumour on the left vulva that had been present for several years. On initial examination, a pedunculated 5×4 cm tumour with mixed reddish and blackish coloration was observed on the left vulvar region. The surface of the lesion was glossy without ulceration (Fig. 1a). A skin biopsy under local anaesthesia revealed BCC histologically.
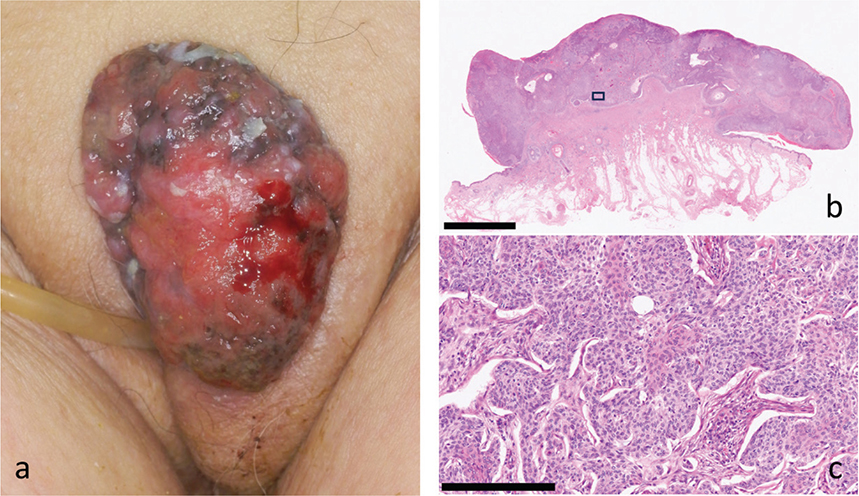
Fig. 1. Clinical and histopathological findings of the recurrent tumour. (a) Clinical appearance of the recurrent lesion. A 5×4 cm exophytic tumour with a reddish, glistening surface and scattered black pigmentation is seen on the left vulva. (b) Low-power view of the resected specimen showing multiple tumour nests in the dermis with a predominantly nodular architecture. The boxed area indicates the field shown in (c) (H&E stain, scale bar = 5 mm). (c) High-power view from the initial excision specimen showing features of mixed-type BCC. The upper area demonstrates nodular architecture with peripheral palisading, while the lower area exhibits infiltrative strands extending into the fibrous stroma. This area was located near the deepest surgical margin, which measured 1.5 mm at its narrowest point on deeper sections (H&E stain; scale bar = 250 μm).
The lesion was surgically excised with a 3-mm margin from the clinically visible border. Histopathological examination of the resected specimen revealed that the tumour was predominantly of the nodular type but exhibited focal areas of thin, cord-like infiltration, consistent with a diagnosis of mixed-type BCC (nodular predominant with focal infiltrative features) (Fig. 1b, c). The closest distance from the tumour to the deepest margin was 1.5 mm at an area with an infiltrative growth pattern; however, all surgical margins were negative.
Postoperatively, due to difficulty attending regular follow-up visits, the patient was monitored at the referring clinic. Six months after surgery, black macules began to appear on the surgical site and gradually increased in size (Fig. 2a). The patient was re-referred to our department with suspected recurrence. Clinical examination revealed clusters of black macules accompanied by surrounding erythema on the vulva. The lesion was excised with a 3-mm margin from the erythematous edge (Fig. 2b).
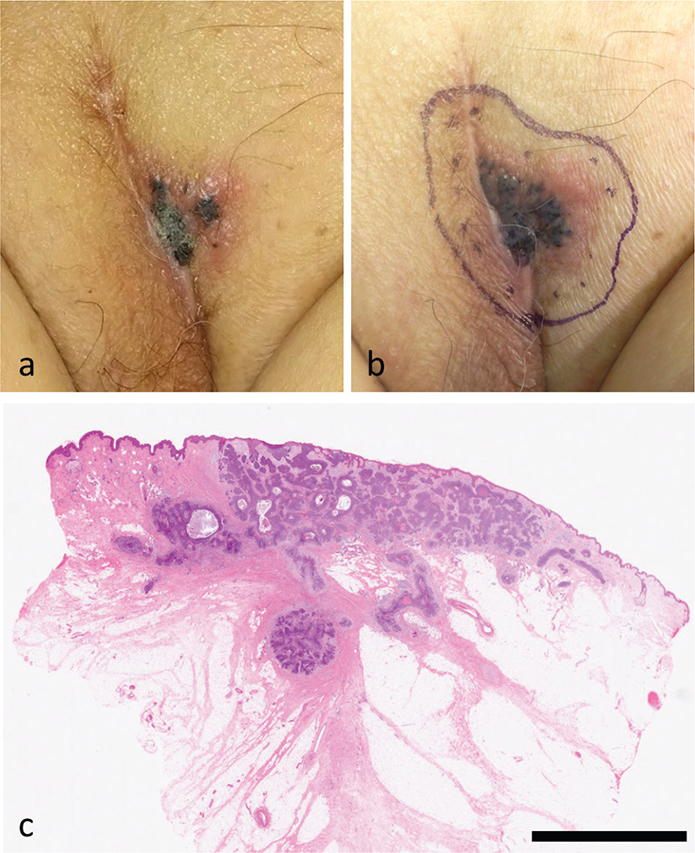
Fig. 2. Clinical progression of the recurrent lesion. (a) At 6 months postoperatively, scattered small black macules with faint erythema appeared at the surgical site. (b) One month later, the lesion had markedly enlarged, showing clustered black macules with prominent peripheral erythema. The lesion was excised with a 3 mm margin from the erythematous area. (c) Low-power view of the recurrent tumour showing a well-demarcated nodular proliferation of basaloid cells extending from the basal layer into the dermis, consistent with a nodular subtype of BCC (H&E stain, scale bar = 5 mm).
Histopathological analysis of the recurrent lesion showed nodular-type BCC without features of infiltrative growth. All margins were again negative (Fig. 2c).
DISCUSSION
This case represents a rare instance of BCC that recurred locally within a short period despite histologically negative surgical margins. It offers important insights into recurrence risk stratification and postoperative management of BCC. In general, recurrence and local control rates of BCC are strongly influenced by its histological subtype. Indolent subtypes are typically well circumscribed and amenable to complete excision, resulting in low recurrence rates, whereas aggressive subtypes tend to infiltrate irregularly into the dermis and laterally, making complete resection more difficult and recurrence more likely (2, 5). In this case, the primary tumour was diagnosed as a mixed-type BCC composed of nodular and infiltrative components, and the surgical specimen appeared to have sufficient margins. However, early local recurrence at the same site within 6 months suggests the possibility of microscopic residual tumour.
While achieving histologically negative margins is considered crucial in BCC excision (4), tumours may exhibit discontinuous infiltration as cords or small nests, which are not always detectable even with serial sectioning (6). In this case, deeper sections of the specimen were evaluated to enhance diagnostic accuracy, and all margins were confirmed to be negative. Nevertheless, the presence of aggressive components, such as infiltrative features, increases the risk of underdiagnosed residual disease, and local recurrence may still occur despite negative margins.
Previous reports have shown that the histological subtype of recurrent BCC may differ from the primary lesion, with some cases demonstrating more aggressive features upon recurrence, while others show a shift toward indolent morphology (1, 7). The mechanism underlying these histological changes remains unclear. In this case, the component closest to the deep margin was infiltrative, yet the recurrent tumour exhibited purely nodular features. One possible explanation is that the nodular component was present within the infiltrative area, or that surgical manipulation or prior biopsy caused morphological alterations, giving rise to an infiltrative-like pattern in what was originally a nodular tumour. Regardless, the likelihood of de novo BCC arising at the same site within 6 months is extremely low, supporting the interpretation that the recurrence was due to residual tumour left at the time of initial surgery.
Recurrence of BCC typically occurs after an average of 2 to 3 years (1, 3), and indolent subtypes are generally associated with slow progression. In contrast, the recurrent tumour in this case, despite being histologically nodular, demonstrated rapid clinical growth mimicking an aggressive subtype. This discrepancy underscores that the clinical behaviour of BCC does not always correlate with its histological subtype.
In summary, this case highlights 2 key points: (i) BCC may recur early due to microscopic residual disease even when margins are histologically negative; and (ii) indolent-type BCC may exhibit clinically aggressive behaviour. This case thus contributes valuable insight into the complexity of BCC recurrence and the limitations of current histopathological assessment.
REFERENCES
- Bartoš V, Pock L, Hercogová J, Mandys V. Recurrent basal cell carcinoma: a clinicopathological study and evaluation of histomorphological findings in primary and recurrent lesions. Acta Dermatovenerol Alp Panonica Adriat 2011; 20: 67–75.
- Crowson AN. Basal cell carcinoma: biology, morphology and clinical implications. Mod Pathol 2006; 19: S127–S147. https://doi.org/10.1038/modpathol.3800512
- Di Maria A, Foresta V, Matarazzo G, Rega D, Schicchi L, Cantelli M, et al. Recurrence of basal cell carcinoma treated with surgical excision and histopathological analysis with frozen section technique with complete margin control (CMC-FS): a 15-year experience of a reference center. Cancers (Basel) 2023; 15: 2359. https://doi.org/10.3390/cancers15153840
- Iurilli M, Cazzato V, Ramella V, Papa G. Exploring the role of surgical margins and reoperation in basal cell carcinoma recurrence: a study of 3036 cases. Arch Dermatol Res 2025; 317: 604–612. https://doi.org/10.1007/s00403-025-04084-3
- Sexton M, Jones DB, Maloney ME. Histologic pattern analysis of basal cell carcinoma: study of a series of 1039 consecutive neoplasms. J Am Acad Dermatol 1990; 23: 1118–1126. https://doi.org/10.1016/0190-9622(90)70344-H
- Rezac L, Wallis L, Black WH, Pearlman RL. Evaluation of a teledermatology postoperative follow-up model after Mohs micrographic surgery. Dermatol Surg 2024; 50: 587–588. https://doi.org/10.1097/DSS.0000000000004126
- Lang PG Jr, Maize JC. Histologic evolution of recurrent basal cell carcinoma and treatment implications. J Am Acad Dermatol 1986; 14: 186–196. https://doi.org/10.1016/S0190-9622(86)70020-0