ORIGINAL REPORT
Impact of Vitiligo on Major Life-changing Decisions and Perceived Stigmatization: A Cross-sectional Study
Lucía CASTELLANO-LOPEZOSA1#, Clara UREÑA-PANIEGO2#, Sofía HASELGRUBER2, Gonzalo BLASCO-MORENTE2 and Salvador ARIAS-SANTIAGO1–3
1Faculty of Medicine, University of Granada, Granada, 2Department of Dermatology, Hospital Universitario Virgen de las Nieves, Granada, and 3Biosanitary Research Institute ibs.GRANADA, Granada, Spain
#These authors contributed equally to this work.
Vitiligo is a chronic autoimmune disease that profoundly affects patients’ quality of life. A cross-sectional, observational study was conducted with 51 patients using self-administered questionnaires, with the aim to evaluate the impact of vitiligo on major life-changing decisions (MLCDs) as well as on stigmatization using a modified version of the Patient Unique Stigmatization Holistic tool in dermatology (PUSH-D) scale. Results showed that the most affected MLCDs were clothing choices, social interactions, and lifestyle changes. Facial vitiligo was significantly associated with a greater impact on work-related decisions. Factors such as being single, not having children, being female, and longer disease duration were linked to higher impact on life decisions. The study emphasizes the importance of addressing both clinical severity and the psychological burden of vitiligo to improve patient care.
SIGNIFICANCE
Vitiligo, while not physically disabling, can have profound psychosocial consequences due to its visible nature, often leading to stigmatization, emotional distress, and reduced self-esteem. Despite growing awareness of its psychological impact, little is known about how vitiligo influences major life decisions, such as career paths, relationships, or family planning. Exploring this impact is essential to better understand the broader consequences of the disease and to limit long-term effects of its impact.
Key words: vitiligo; life-changing decisions; stigma; quality of life.
Citation: Acta Derm Venereol 2025; 105: adv44198. DOI: https://doi.org/10.2340/actadv.v105.44198.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 23, 2025. Accepted after revision: Jul 10, 2025. Published: Aug 5, 2025.
Corr: Salvador Arias-Santiago, Department of Dermatology, Hospital Universitario Virgen de las Nieves, Avenida de Madrid 15, ES-18012 Granada, Spain. E-mail: salvadorarias@ugr.es.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Vitiligo is an acquired pigmentation disorder affecting 0.1–2% of the population, characterized by the progressive loss of melanocytes (1). The condition has recently gained renewed clinical attention following the approval of ruxolitinib (Opzelura®, OPZ) (2), a receptor-independent JAK 1 and 2 inhibitor targeting interferon-gamma and IL-15. Although originally developed for other indications, such as myeloproliferative tumours, psoriatic arthritis, alopecia areata, and ulcerative colitis, its recent approval for vitiligo has shown promising results in terms of disease onset, progression, stability, repigmentation and relapse rates (2).
Vitiligo, beyond its physical effects, significantly impacts patients’ identity and self-esteem (3). Studies show its effect on quality of life is comparable to other chronic skin conditions like eczema or psoriasis, especially in social and sexual contexts (4). Tools such as the Dermatology Life Quality Index (DLQI), the Vitiligo Impact Scale (VIS), and the Vitiligo Impact Patient scale (VIPs) have been used to assess this impact (5). However, stigmatization in vitiligo remains an underexplored area. In 2022, the Patient Unique Stigmatization Holistic tool in dermatology (PUSH-D) questionnaire was developed, a validated and reliable tool that explores stigmatization in people with visible skin disease. Short and easy to use, it even allows for comparing the level of stigma across different skin conditions. (6)
The concept of major life-changing decisions (MLCDs) includes choices that have a significant impact on someone’s personal, professional, or emotional trajectory (7). A chronic illness diagnosis like vitiligo may shift patients’ priorities and limit these decisions. Even minor but recurring symptoms such as itching can lead to broader impacts, such as insomnia and decreased academic performance. Bhatti et al. found that dermatological conditions notably affect choices related to education, work, and relationships, particularly among younger individuals. Factors like disease severity, shame, appearance, and frequent hospital visits were closely linked to these effects (7).
In light of this, the aim of this study was to describe the impact of vitiligo on MLCDs in a cohort of patients with this disease while exploring the factors associated with a greater impact and to evaluate the degree of stigmatization among these patients.
MATERIALS AND METHODS
Study design
This is an analytical, observational, and cross-sectional study aimed at assessing the impact of vitiligo on major life-changing decisions (MLCDs) and perceived stigmatization through a self-administered questionnaire. The objective is to evaluate the impact of vitiligo on patients’ life decisions and perceived stigma. Sociodemographic and clinical data were also collected.
Patient population
The target population includes patients diagnosed with vitiligo, regardless of sex, age, disease severity, or duration. Participants were recruited consecutively from the Phototherapy Unit at the Dermatology Department of Hospital Universitario Virgen de las Nieves, as well as through anonymous online surveys distributed to vitiligo patients via the Spanish Vitiligo Association (Asociación Española de Pacientes de Vitíligo, ASPAVIT) website (https://aspavit.org).
Inclusion criteria
Inclusion criteria were: patients diagnosed with vitiligo by a dermatologist, regardless of age and severity of the disease, and who provided their informed consent in order to participate in the study.
Exclusion criteria
Exclusion criteria were: individuals who did not wish to participate, individuals unable to provide informed consent, and patients with other chronic illnesses that may affect life decisions or perceived stigmatization.
Ethics
The study was approved by the Research Ethics Committee of the Province of Granada and is performed in accordance with the Organic Law 3/2018, of 5 December, on the Protection of Personal Data and Guarantee of Digital Rights (Code: SICEIA-2025-000744).
Variables of interest
Main variable: Impact of vitiligo on major life-changing decisions (MLCDs), evaluated by patients using a 4-point Likert scale (0 = no impact; 4 = significant impact) in the following areas, as described by Bhatti et al.:
- Job-related MLCD: work performance, career choice, absenteeism, salary, promotion opportunities and early retirement.
- Education-related MLCD: academic performance, highest level of education achieved.
- Social-related MLCD: family, social interactions, partner selection, sexual impairment.
- Parenthood-related MLCD: decision to have children, number of children.
- Other MLCD: place of residence, type of housing, living abroad, clothing choices, holiday destinations, sports participation, smoking and drug use.
Other variables:
- Sociodemographic and clinical variables (age, sex, occupation, education level, disease duration, visibility of lesions, comorbidities, and current or past treatments).
- World Health Organization-Five Well-Being Index (WHO-5): Assesses well-being over the previous 2 weeks through 5 statements rated on a scale from 0 to 5, with a total score ranging from 0 (lowest well-being) to 25 (highest well-being). Scores may be converted to a percentage (0–100%) by multiplying by 4. A score below 50% (or < 13 in raw score) suggests low mental well-being and may indicate the need for further evaluation for disorders such as depression.
- Perceived stigmatization: Assessed using a modified version of the Patient Unique Stigmatization Holistic tool in dermatology (PUSH-D). The questionnaire was adapted to a binary response format (yes/no) instead of the original Likert scale. It evaluates 2 dimensions:
- - Felt stigma: internal emotions such as shame or anticipation of discrimination (8 items).
- - Enacted stigma: actual experiences of discrimination in various contexts (9 items).
- Disease severity measured using 2 different tools based on the mode of patient participation: the VASI scale (8), administered by a dermatologist, for in-person patients; and its self-assessed digital version, SA-VASI, for remote participants (9). The latter assesses disease severity based on depigmentation level (0–100%) and affected body area across 7 regions: head/neck, arms, legs, trunk, genitals, hands, and feet. Patients estimate how many handprints (fingers together) are needed to cover the depigmented area, including decimals if needed. Final VASI score (tVASI) is calculated as follows:
tVASI (0–100) = ∑ VASI for each body region
VASI per region = % affected area (0%-maximum per region%) x depigmentation grade (0.0–1.0)
Statistical analysis
A descriptive analysis was conducted to characterize the sample, presenting continuous variables as means and standard deviations (SD), and categorical variables as absolute and relative frequencies. Either a χ2 or Fisher’s exact test was used for comparisons of categorical variables, and Student’s t-test or Wilcoxon– Mann–Whitney test for continuous variables. Correlation and linear regression analyses were performed to explore relationships among emotional well-being (WHO-5), perceived stigmatization (PUSH-D), and the impact on life decisions (MLCD). Additionally, multivariable regression models were developed to identify factors associated with MLCD impact, emotional well-being, and perceived stigma.
RESULTS
Sociodemographic and clinical features of the sample
A total of 51 patients were included in the study. Mean age of the patients was 49.60 years (SD = 13.43) and female to male ratio was 2.4 (36:15). Some 54.9% (28/51) of patients were married and 66.7% (34/51) had children. Most patients (66.6%, 34/51) had completed higher education, and 78.4% (40/51) were actively employed. Phototypes III (27.4%; 14/51) and IV (31.4%; 16/51) were the most frequent in our study. In total, 41% (21/51) of patients were being treated with topical ruxolitinib. More detailed information is given in Table I.
In terms of severity, a box-plot diagram was created to illustrate the severity of vitiligo in the patient sample based on both their SAVASI scores and facial involvement in particular (Fig. 1). As for perceived severity, a sector diagram displays the results in Fig. 2.
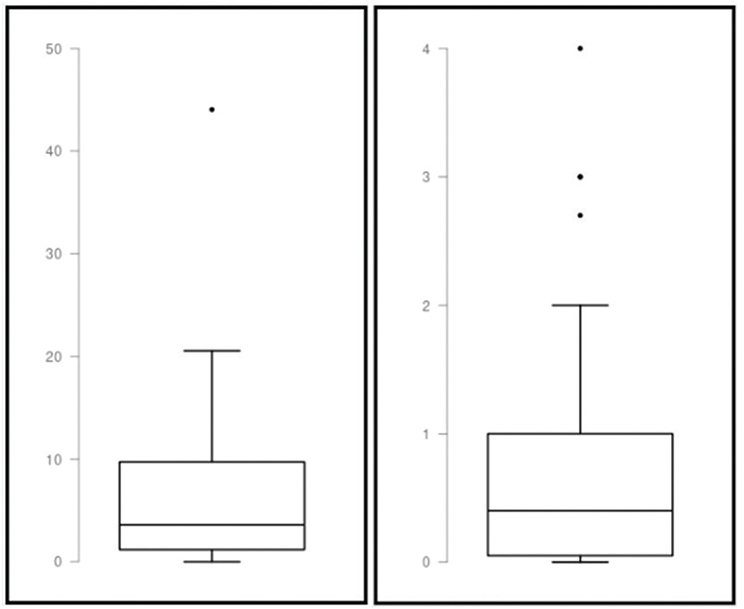
Fig. 1. Box-plot diagrams representing the severity of vitiligo based on SAVASI scores (left) and facial involvement (right). SAVASI: Severity of Alopecia and Vitiligo Activity and Severity Index.
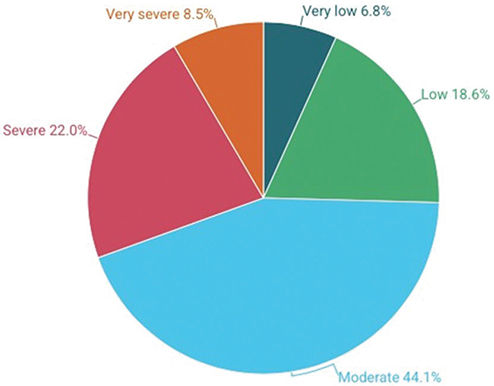
Fig. 2. Perceived severity of the disease.
Impact of vitiligo on major life-changing decisions
The most affected MLCDs were those related to social relationships (median [IQR] score 1 [0–2]), lifestyle (1 [0–2]), and choice of clothing (1 [0–2]). Other affected domains of MLCDs were career choice, job performance, love life, and holidays destination (0 [0–2] for all of them), among others. Fig. 3 displays the percentage of patients experiencing a moderate to severe impact of the disease on the most affected MLCDs. Detailed information is presented in Table II.
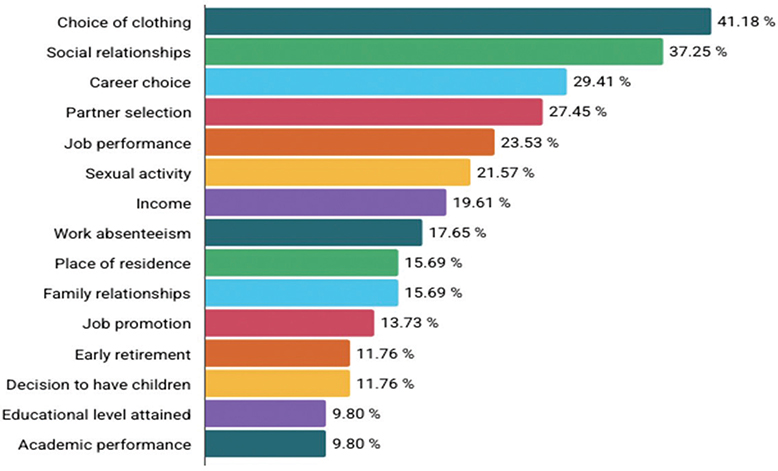
Fig. 3. Percentage of patients showing a moderate to high impact of vitiligo on MLCD. Only the most affected MLCDs are shown. MLCD: major life-changing decisions.
| Impact score | MLCD score, median (IQR)* |
| MLCD related to job, median (IQR) | |
| Impact of vitiligo on career choice | 0 (0–2) |
| Impact of vitiligo on job performance | 0 (0–2) |
| Impact of vitiligo on job promotion opportunities | 0 (0–0.25) |
| Impact of vitiligo on absenteeism days | 0 (0–1) |
| Impact of vitiligo on salary | 0 (0–0) |
| Impact of vitiligo on job dismissal or dropout | 0 (0–0) |
| Impact of vitiligo on early retirement decision | 0 (0–0) |
| MLCDs related to education, median (IQR), median (IQR) | |
| Impact of vitiligo on educational performance | 0 (0–1) |
| Impact of vitiligo on level of education achieved | 0 (0–0) |
| MLCDs related to relationships | |
| Impact of vitiligo on family relationships | 0 (0–1) |
| Impact of vitiligo on social relationships | 1 (0–2) |
| Impact of vitiligo on choice of partner | 0 (0–0.5) |
| Impact of vitiligo on love life | 0 (0–2) |
| Impact of vitiligo on existence of sexual impairment | 0 (0–1) |
| MLCDs related to paternity/maternity, median (IQR) | |
| Impact of vitiligo on desire to have children | 0 (0–0) |
| Impact of vitiligo on not having had children | 0 (0–1.5) |
| Impact of vitiligo on not having the number of children desired | 0 (0–1.5) |
| Other MLCDs, median (IQR) | |
| Impact of vitiligo on selection of current home | 0 (0–0) |
| Impact of vitiligo on selection of city/town to live in | 0 (0–0) |
| Impact of vitiligo on living abroad | 0 (0–0) |
| Impact of vitiligo on domestic travel | 0 (0–2) |
| Impact of vitiligo on travel abroad | 0 (0–1) |
| Impact of vitiligo on changing lifestyle or habits | 1 (0–2) |
| Impact of vitiligo on choice of clothing | 1 (0–2) |
| Impact of vitiligo on physical exercise (type of frequency) | 0 (0–1) |
| Impact of vitiligo on alcohol consumption | 0 (0–0) |
| Impact of vitiligo on smoking (tobacco) | 0 (0–0) |
| Impact of vitiligo on drugs consumption | 0 (0–0) |
| Impact of vitiligo on intake of antidepressant or anxiolytic medication | 0 (0–1) |
| IQR: interquartile range. *scale: 0–4: 0=no impact, 1=mild, 2= moderate, 3=high, 4=significant impact. |
|
Sociodemographic and clinical determinants linked with the most frequently impacted MCLDs
Univariate analyses were performed to explore the clinical and sociodemographic factors associated with MLCDs in patients with vitiligo. The most affected MLCD domains were included in the analysis: choice of clothing, social relationships, and lifestyle and habits changes. Clothing preferences appeared to be significantly associated with longer disease duration (p = 0.0022) and with not having children (p = 0.040). There was also a trend suggesting a higher impact on clothing among women with vitiligo (p = 0.027).
Regarding social interactions, the impact of vitiligo was greater among individuals who were single (p = 0.025) and those who did not have children (p = 0.019).
Changes in daily habits were more frequently reported by younger individuals (p = 0.037), with a tendency for greater impact among single participants as well (p = 0.053).
Impact of facial vitiligo on MLCDs
Facial involvement was found to be significantly associated with several MCLDs and a higher overall lifetime impact of the disease (p = 0.013). Specifically, it was associated with a more significant impact on the professional sphere compared with the impact observed when considering the overall extent of the disease. It was linked to the choice of professional career (p = 0.020), reported difficulties in job performance (p = 0.010), reduced opportunities for promotion (p = 0.0001), and lower income levels (p < 0.029).
Patient–clinician discrepancies in the perceived impact of vitiligo on major life choices
The results suggest that as the SA-VASI score increases, patients also tend to report a higher perceived severity of their condition. The Spearman coefficient obtained was ρ = 0.2840, which indicated a weak positive correlation. The associated p-value (p = 0.0434) indicates that this correlation is statistically significant, which supports the existence of a real, though limited, relationship between the 2 variables.
Regarding the relationship between SA-VASI and the subjective impact of vitiligo on quality of life, a weak to moderate positive correlation was observed (Spearman’s ρ = 0.3376, p = 0.0154), implying that, in general, higher perceived disease impact by the patient was associated with higher objective severity scores as measured by SA-VASI.
Perceived stigmatization in patients with vitiligo
Upon analysing the results of the Adapted Version of the PUSH-D questionnaire, more than 65% (34/51) of participants marked 0 or 1 item in total (Figure 4).
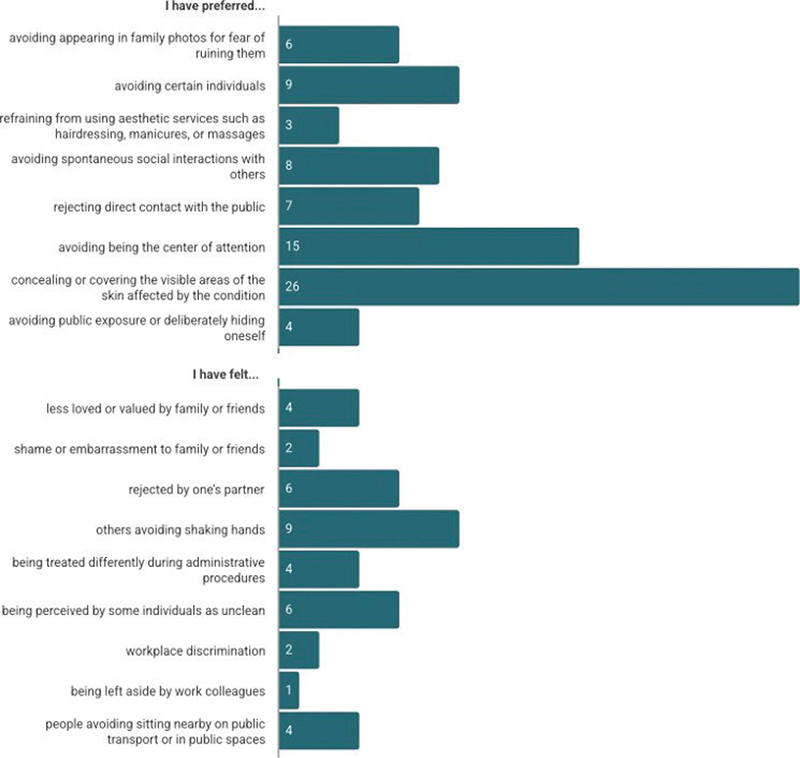
Fig. 4. Results of the modified version of the Patient Unique Stigmatization Holistic tool in dermatology.
Notably, those patients with the lowest scores on the WHO-5 also reported the highest levels of perceived stigma. The total PUSH-D score showed a moderate, statistically significant negative correlation with emotional well-being (r = –0.332, p = 0.0172), suggesting that higher levels of perceived stigmatization are associated with lower subjective well-being. A combination of active social avoidance behaviours and emotional responses was observed across responses among these patients.
No significant differences in perceived stigmatization were found between patients undergoing treatment with topical ruxolitinib and those who were not (p = 0.7069).
No significant associations were found between perceived stigmatization and vitiligo severity, whether measured by the SA-VASI scale (r = –0.143, p = 0.317) or by categorical perceived severity (p = 0.750).
DISCUSSION
The analysis of the correlation between the objective severity of vitiligo and patients’ subjective perceptions revealed only weak to moderate correlations. Patients may underestimate or overestimate the severity of their condition based on psychosocial and emotional factors that are not captured by standard scoring systems (10), which places emphasis on the importance of integrating both clinician and patient-reported measures into clinical evaluations, particularly in chronic and visible conditions such as vitiligo (11).
While the most affected MLCDs overall were clothing preferences, social interaction, and changes in lifestyle and daily habits, facial involvement appeared to be specifically associated with a greater impact on work-related decisions. This observation is consistent with the findings of Silveira et al., highlighting that individuals with vitiligo are frequently excluded from public-facing occupations in Brazil and are deemed ineligible to join the military in India (12). These examples underscore the significant impact that facial involvement can have on professions with strict aesthetic or public image requirements (13).
An important factor associated with a greater impact of the disease in MLCDs was being single as well as not having children, which could reveal the importance of a strong support system (14), longer duration of the disease, or being female or young. This latter finding is consistent with those of Sampogna et al., who found higher rates of dysmorphic concerns in women with skin conditions compared with men (15); Zahra et al. also reported higher levels of social stigma and social appearance anxiety among women, leading to a more impaired quality of life compared with men (13).
Perceived stigmatization was explored using a binary-adapted version of the PUSH-D scale. The majority of patients marked few or no items, particularly on the emotional subscale (“you have felt…”), which may suggest low perceived stigma in patients with vitiligo. This could also suggest that the binary response system contributed to an underreporting of perceived stigmatization, as opposed to other studies that show a greater impact on felt and enacted stigma in vitiligo patients (16).
The presence of stigma was associated with reduced emotional well-being, as evidenced by the negative correlation between PUSH-D scores and WHO-5 scores; this may either highlight the emotional burden of stigmatization or be a confounding factor. Interestingly, perceived stigmatization did not correlate with objective disease severity. This could suggest that perceived stigma is shaped more by individuals’ subjective experience than by measurable clinical features (11).
Limitations
Several limitations must be acknowledged. First, the relatively small sample size, while sufficient for exploratory analyses, limits generalizability. In addition to this, the underrepresentation of younger individuals may have influenced the results, given that skin diseases often have a more pronounced psychosocial impact on the paediatric population (17). Moreover, the cross-sectional design does not allow causal inference. Furthermore, to this date the SA-VASI system lacks stratified severity levels, preventing use of concordance analyses like the kappa coefficient; instead, Spearman’s correlation was applied. Lastly, the use of a binary version of the PUSH-D scale reduces the validity of the stigmatization data and restricts interpretability.
Conclusion
This study addresses the multifaceted impact of vitiligo, showing its influence not only on physical appearance but also on psychosocial well-being and key life decisions. While facial involvement notably exacerbates the disease’s impact, particularly in professional domains, the overall effect on life-changing decisions seems to be less pronounced compared with other dermatological conditions such as psoriasis (18) or atopic dermatitis (19). Discrepancies between clinical assessments and patient perceptions underline the importance of a patient-centred approach in treatment. Further research is needed, as well as validated tools adapted to real-world clinical settings, ensuring that both the physical and emotional needs of patients are adequately addressed.
ACKNOWLEDGEMENTS
IRB approval status: The study was approved by the Institutional Review Board of our centre (approval number SICEIA-2025-000744)).
REFERENCES
- Pérez-Bootello J, Cova-Martín R, Naharro-Rodríguez J, Segurado-Miravalles G. Vitiligo: pathogenesis and new and emerging treatments. Int J Mol Sci 2023; 24: 17306. https://doi.org/10.3390/ijms242417306
- Kang C. Ruxolitinib cream 1.5%: a review in non-segmental vitiligo. Drugs 2024; 84: 579–586. https://doi.org/10.1007/s40265-024-02027-2
- Eleftheriadou V, Ahmed A, Nesnas J, Nagra R. The lifetime risk and impact of vitiligo across sociodemographic groups: a UK population-based cohort study. Br J Dermatol 2024; 192: 63–71. https://doi.org/10.1093/bjd/ljae282
- Rosmarin D, Soliman AM, Piercy J, Marwaha S, Anderson P, Camp HS. Health-related quality-of-life burden among adults with vitiligo: relationship to disease severity and disease location. Dermatol Ther (Heidelb) 2024; 14: 1633–1647. https://doi.org/10.1007/s13555-024-01187-z
- Seneschal J. Clinical features of vitiligo and social impact on quality of life. Dermatol Pract Concept 2023; 13: e2023312S. https://doi.org/10.5826/dpc.1304S2a312S
- Ezzedine K, Shourick J, Bergqvist C, Misery L, Chuberre B, Kerob D, et al. Patient Unique Stigmatization Holistic tool in dermatology (PUSH-D): development and validation of a dermatology-specific stigmatization assessment tool. J Eur Acad Dermatol Venereol 2023; 37: 443–450. https://doi.org/10.1111/jdv.18641
- Bhatti ZU, Salek S, Finlay AY. Concept of major life-changing decisions in life course research. Curr Probl Dermatol 2013; 44: 52–66. https://doi.org/10.1159/000350389
- Komen L, da Graça V, Wolkerstorfer A, de Rie MA, Terwee CB, van der Veen JPW. Vitiligo Area Scoring Index and Vitiligo European Task Force assessment: reliable and responsive instruments to measure the degree of depigmentation in vitiligo. Br J Dermatol 2015; 172: 437–443. https://doi.org/10.1111/bjd.13432
- Komen L, van der Kraaij GE, van der Veen JPW, de Rie MA, Wolkerstorfer A. The validity, reliability and acceptability of the SAVASI: a new self-assessment score in vitiligo. J Eur Acad Dermatol Venereol 2015; 29: 2145–2151. https://doi.org/10.1111/jdv.13161
- Ezzedine K, Eleftheriadou V, Jones H, Bibeau K, Kuo FI, Sturm D, et al. Psychosocial effects of vitiligo: a systematic literature review. Am J Clin Dermatol 2021; 22: 757–774. https://doi.org/10.1007/s40257-021-00631-6
- Bibeau K, Ezzedine K, Harris JE, van Geel N, Grimes P, Parsad D, et al. Mental health and psychosocial quality-of-life burden among patients with vitiligo: findings from the Global VALIANT study. JAMA Dermatol 2023; 159: 1124–1128. https://doi.org/10.1001/jamadermatol.2023.2787
- Silveira LP, Grijsen ML, Follador I, Dellatorre G. How persistent stigma and discrimination keep people with visible skin diseases out of jobs: vitiligo in Brazil today. Lancet Reg Health Am 2023; 23: 100524. https://doi.org/10.1016/j.lana.2023.100524
- Zahra M, Zubair A, Aslam N, Naz M. Investigating the impact of perceived social stigmatization and social appearance anxiety on quality of life among patients with facial skin diseases. Arch Dermatol Res 2025; 317: 198. https://doi.org/10.1007/s00403-024-03719-1
- Ning X, Zhang Y, Wang W, Yan H. The association between social support and depression among patients with vitiligo in China. Front Psychol 2022; 13: 939845. https://doi.org/10.3389/fpsyg.2022.939845
- Sampogna F, Samela T, Abeni D, Schut C, Kupfer J, Bewley AP, et al. A cross-sectional study on gender differences in body dysmorphic concerns in patients with skin conditions in relation to sociodemographic, clinical and psychological variables. J Eur Acad Dermatol Venereol 2025; 39: 823–832. https://doi.org/10.1111/jdv.20247
- Fakih A, Tannous R, Lajnef M, Seneschal J, Andreu N, Tran VT, et al. Stigma in vitiligo: associated factors and severity strata of the Patient Unique Stigmatization Holistic tool in Dermatology (PUSH-D) score. Br J Dermatol 2024; 190: 712–717. https://doi.org/10.1093/bjd/ljae020
- Paller AS, Rangel SM, Chamlin SL, Hajek A, Phan S, Hogeling M, et al. Stigmatization and mental health impact of chronic pediatric skin disorders. JAMA Dermatol 2024; 160: 621–630. https://doi.org/10.1001/jamadermatol.2024.0594
- Sánchez-Díaz M, Díaz-Calvillo P, Soto-Moreno A, Molina-Leyva A, Arias-Santiago S. Factors influencing major life-changing decisions in patients with psoriasis: a cross-sectional study. Acta Derm Venereol 2023; 103: adv11640. https://doi.org/10.2340/actadv.v103.11640
- Fuentes-Barragán L, García-Moronta C, Sanabria-de la Torre R, León-Pérez FJ, Molina-Leyva A, Arias-Santiago S, et al. Impact on major life-changing decisions in patients with atopic dermatitis. Acta Derm Venereol 2025; 105: adv42241. https://doi.org/10.2340/actadv.v105.42241