ORIGINAL REPORT
Curettage vs Electrodessication for Paediatric Molluscum Contagiosum: Efficacy and Safety Follow-Up Study
Daniel HILEWITZ1,2, Efrat BAR-ILAN1,2, Noa HADAYER1, Ayelet OLLECH2,3, Tal KIND1 and Shoshana GREENBERGER1,2
1Pediatric Dermatology Unit, The Department of Dermatology, Sheba Medical Center, Ramat Gan, 2Grey Faculty of Medical & Health Sciences, Tel Aviv University, Tel Aviv, and 3Current affiliation: Pediatric Dermatology Service, Shaare Zedek Medical Center, Faculty of Medicine, The Hebrew University of Jerusalem, Jerusalem, Israel
Molluscum contagiosum (MC) is a common paediatric cutaneous infection caused by a DNA poxvirus, resulting in lesions that often impair patients’ quality of life. Although MC typically resolves spontaneously, parents frequently seek treatment due to cosmetic concerns, pruritus, or fear of lesion spread. Currently, there is no gold standard treatment, and various therapeutic modalities – including curettage and electrodessication (ED) – are utilized in clinical practice. This prospective comparative study aimed to compare efficacy, cosmetic outcome, and patient satisfaction with curettage vs ED as treatment methods in the treatment of MC. The study included 103 paediatric patients presenting with confirmed MC and ≥ 10 lesions (or 5 on face), treated at Sheba Medical Center. Treatment allocation to either curettage or ED was based on guardian preference. Data collected included demographic and clinical characteristics, procedural outcomes, pain levels, and satisfaction ratings. Structured questionnaires were administered 6 weeks post-procedure to evaluate outcomes, including lesion recurrence, infection, remnants, healing duration, and patient/parent satisfaction. Statistical analyses were conducted, with statistical significance defined as p ≤ 0.05. Among the cohort (mean age, 4.37 years; 60% female), 67 (61.7%) patients were treated with curettage and 42 (38.3%) with ED. Most presented with facial lesions (67.96%) and multiple lesion sites (50.5%). Patients treated with curettage reported fewer remnants (42.9% vs 70%, p = 0.007), greater aesthetic satisfaction (p = 0.039), and faster recovery (p = 0.050). Pain levels were comparable between groups, but higher 1-week post-procedure in ED (p = 0.014). Recurrence rates were similar for both methods (49.2% curettage, 35% ED). Curettage offers clear advantages over ED for the treatment of MC, resulting in superior aesthetic outcomes, faster recovery, and lower post-procedural pain. Therefore, curettage should generally be preferred, while ED may be considered for precise interventions in sensitive anatomical areas.
Key words: molluscum contagiosum; curettage; electrodessication; aesthetic; scar.
SIGNIFICANCE
- Why was the study undertaken? The study aims to compare 2 treatment types: curettage and electrodessication, to find when it is best to use each method when treating paediatric MC.
- What does this study add? Curettage was associated with fewer remnants, faster recovery, and higher patient satisfaction, particularly in terms of aesthetic outcomes, when compared with electrodessication.
- What are the implications of this study for disease understanding and/or clinical care? The findings suggest curettage may be preferable in many cases, while electrodessication could be considered for anatomically sensitive areas. Further research is recommended to confirm these results.
Citation: Acta Derm Venereol 2025; 105: adv44300. DOI: https://doi.org/10.2340/actadv.v105.44300.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 3, 2025; Accepted after revision: Aug 27, 2025. Published: Oct 8, 2025.
Corr: Shoshana Greenberger, Pediatric Dermatology Unit, Sheba Medical Center, Ramat-Gan 52621, Israel. E-mail: Shoshana.greenberger@sheba.health.gov.il
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Molluscum contagiosum (MC) is a cutaneous infection caused by a DNA poxvirus and commonly affects children (peak age of onset from 2 to 12 years) (1). The virus is spread through direct skin-to-skin contact or indirect skin contact with fomites, such as bath towels, sponges, and gym equipment. MC ranks among the 50 most prevalent diseases worldwide (2). In children, its annual incidence ranges from 2% to 10% and its prevalence from 5.1% to 11.5% (3–10). Following an incubation period of 2–7 weeks, lesions typically occur on the chest, arms, trunk, legs, and face. Numerous lesions may develop in intertriginous areas, such as the axillae and intercrural regions. Lesions may infrequently occur on the mucous membranes of the lip, tongue, and conjunctiva. The palms are spared. Patients with underlying atopic dermatitis are predisposed to develop large numbers of lesions (11). The face is a frequent anatomical location for MC in children, and facial involvement has been associated with higher likelihood of recurring MC-related complaints (12). Importantly, patients with underlying atopic dermatitis are predisposed to develop larger numbers of lesions and suffer more from itching (13).
MC may resolve spontaneously; the average time to spontaneous resolution of MC is approximately 13 months, with 30% of cases persisting for more than 18 months (5, 14). Nonetheless, many patients and parents seek treatment. Severe impairments of quality of life have been reported in 10% of children with MC infection (14). This may result from itching, aggravation of atopic dermatitis, being bullied about the lesions, fear of the lesions spreading to other sites, or for cosmetic reasons (2).
Currently, there is no consensus on MC management. Available treatment options (15) include destructive modalities such as curettage, cryotherapy, electrodessication, and chemical agents such as topical NO, nitric oxide, cantharidin, potassium hydroxide, salicylic acid, phenols and immunomodulators (e.g., imiquimod) (16). Cantharidin 0.7% (YCANTHTM) is the only FDA-approved therapy for MC. Evidence-based guidelines supporting the efficacy of various treatments are currently limited. For patients with numerous lesions requiring treatment, curettage and electrodessication (cautery) are considered to be viable and effective procedures (17, 18). However, prospective studies comparing the efficacy and safety of these 2 methods are missing. Therefore, the aim of this study is to compare the differences in the clinical and aesthetic outcome, pain, and healing time in patients treated with either curettage or ED for MC removal.
PATIENTS AND METHODS
A prospective study was conducted at the Pediatric Dermatology Department at Safra Children’s Hospital, Sheba Medical Center, from 1 July 2023, to 1 January 2025. The study population included all paediatric patients (age < 18 years) referred for removal of MC under anaesthesia. Inclusion criteria included MC diagnosis confirmed by a dermatologist, at least 10 clinically typical, visible, and discrete MC lesions on trunk/limbs or 5 on the face. Exclusion criteria included children with immunosuppression or other systemic diseases that may affect MC resolution or wound healing and parents not willing to sign an informed consent form. Patients and their parents chose between the 2 methods of wart removal: curettage or ED. The 2 techniques were not used concurrently in the same patient, except in the case of eyelids, which were consistently treated with ED.
A total sample size of 88 participants (44 per group) was calculated to detect a medium effect size (w = 0.3) in the distribution of satisfaction levels (low, medium, high) between the 2 treatment groups using a χ2 test (α = 0.05, power = 80%). To account for potential dropouts, the final planned sample size was increased to 100 patients.
Data collected included demographic (age, sex, ethnicity) and clinical (skin type based on the Fitzpatrick scale, history of atopic conditions and previous treatments for MC, number, location, and size of the lesions, as well as whether they showed signs of inflammation). Treatment was done under sedation with sevoflurane or nitrous oxide gas. Curettage was done with a sterile Hebra curette and ED was done with high frequency desiccator AARON940 monopolar. All the parents were instructed to shower daily with water and soap and apply topical antibiotic (mupirocin or ointment) twice daily for 1 week after the procedure. Six weeks post-treatment, structured questionnaires were administered to participants or their parents to evaluate treatment outcomes. The questionnaire assessed the emergence of new lesions, the occurrence of post-procedural infections that required systemic antibiotics, and the presence of any remnants at the treated sites. Additionally, questions were asked on pain levels (a scale from 1 to 4, 1 = no pain, 2 = mild pain, 3 = moderate pain, 4 = severe pain) at 4 specific time points: the day of the procedure, the day following the intervention, 1 week post-procedure, and 6 weeks after treatment. Beyond clinical outcomes, the questionnaire also examined patient and parent satisfaction (on a scale from 0 to 10, 0–3: low, 4–7: medium, 8–10: high) with various aspects of the treatment: healing time, aesthetic satisfaction with the outcome, and overall satisfaction with the therapeutic process. Furthermore, participants were asked to rate the likelihood of recommending the procedure to others on a numerical scale from 0 to 10. Patients who failed to complete the follow-up questionnaire after 6 weeks following 2 separate reminders were excluded from the final analysis. This study was approved by the institutional ethics committee of Sheba Medical Center (9554-22-SMC).
Statistical analysis
Categorical variables are presented with numbers and adjusted frequency, ordinal variables are presented with frequency, and continuous variables are presented by mean ± standard deviation. The normality of the data was tested by Kolmogorov–Smirnov test. Levene’s test was used to assess the equality of variances. Student’s t-test was used to compare the differences between 2 independent groups of continuous variables that are normally distributed. The Mann–Whitney test was used to evaluate the differences between independent groups that are not normally distributed and for ordinal variables. The association between 2 categorical variables was evaluated using either the χ2 test or Fisher’s exact test (2-tailed), depending on the specific dataset characteristics and sample sizes. Logistic regression is used to predict binary results as a function of continuous and categorial variables. A p-value ≤ 0.05 was considered statistically significant. Data were analysed by using SPSS software (IBM Corp, Armonk, NY, USA).
RESULTS
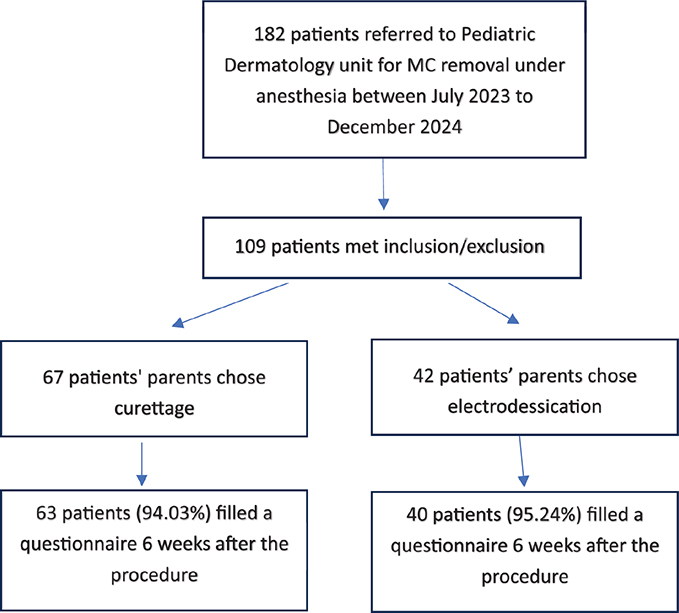
Between July 2023–December 2024, a total of 182 children (ages 0–18) were referred to the Pediatric Dermatology Unit at Safra Children’s Hospital, Sheba Medical Center, for the removal of MC under anaesthesia. Of these, 109 children met the inclusion and exclusion criteria, and their parents provided consent to participate in the study. Ultimately, 103 participants’ parents completed the questionnaire and were included in the study population (Fig. 1). The demographic characteristics of the study population and clinical details regarding the lesions are presented in Table I. The cohort comprised 43 male and 60 female patients with a mean age of 4.37 ± 2.66 years (range 1–13.1). Atopic dermatitis was a background diagnosis for only 4 (3.88%). Among the participants, 40 patients (38.3%) underwent wart removal via ED, while 63 patients (61.7%) underwent wart removal via curettage. The most common anatomical location of the lesions was the face, in 70 patients (67.96%). Of the study population, 52 (50.5%) had lesions in more than 1 anatomical region. Overall, 50 patients (48.5%) presented with lesions that measured between 0 and 3 mm in diameter. Within subgroups, 36.5% of the curettage group and 67.5% of the ED group fell into this category (p = 0.002). Similarly, 26 patients (25.2%) had lesions 5–10 mm in size, including 34.9% of those treated with curettage and 10% of those treated with ED (p = 0.005). Only 11 patients (10.7%) presented with lesions more than 10 mm in size and most of these also were removed by curettage. Twenty-nine patients (28.2%) presented with 5–10 lesions, 35 (34%) patients presented with 10–20 lesions, and 39 patients (37.9%) presented with more than 20 lesions. Forty-two (40.8%) of this cohort presented with inflamed lesions.
Among the study population, no new lesions developed in 58 patients (56.3%) by the end of the 6-week follow-up period (50.8% vs 65% for curettage or ED, p = 0.157). Notably, localized infection was reported by the patients or their parents in only 12 patients (11.6%) at the conclusion of the follow-up period.
Among the patients who underwent ED, 28 (70%) reported post-procedural remnants (in any of the lesions), compared with 27 patients (42.9%) in the curettage group (p = 0.007). Pain levels were generally low across both groups, with no significant differences between the 2 techniques in the mean pain level on the day of treatment or the following day. However, 1 week after the procedure, patients treated with electrodessication reported significantly higher pain compared with those treated by curettage (1.09 ± 0.43 vs 1.42 ± 0.87, p < 0.001). By 6 weeks, pain scores had declined in both groups and no significant difference was observed (p = 0.057) (Fig. 2). In both groups, the reported pain levels were highest on the day following the procedure compared with other time points assessed (Fig. 2). The clinical outcomes are based on the questionnaire responses presented in Table II.
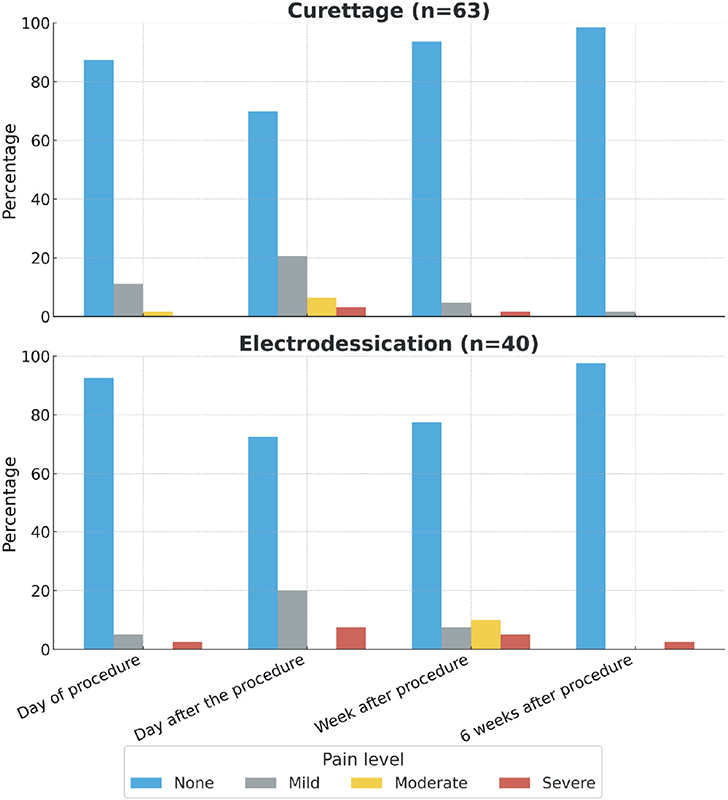
Fig. 2. Patients’ report of pain.
Patient satisfaction regarding aesthetic outcomes, healing time, overall treatment experience, and willingness to recommend the procedure is presented in Fig. 3 and Table III. Notably, aesthetic satisfaction and satisfaction with healing time were significantly higher in the curettage group (p = 0.039 and p = 0.05, respectively) (Fig. 4).

Fig. 3. Satisfaction with treatment.

Fig. 4. Representative picture of patient before and after curettage treatment.
No statistically significant risk factors for lesion recurrence were identified (Table IV).
DISCUSSION
MC lesions are a prevalent dermatological condition; however, there is no universally accepted management approach. This prospective study presents a comparative analysis of curettage and ED for the treatment of MC in a paediatric population, evaluating key clinical outcomes, pain levels, aesthetic satisfaction, and patient-reported measures of quality of life. Both methods demonstrated effectiveness in achieving lesion removal, and overall satisfaction was high. However, curettage had a significant advantage regarding post-procedural remnants and aesthetic satisfaction, providing valuable evidence to inform clinical decision-making in the management of this common dermatological condition.
The advantage of ED compared with curettage include shorter duration of the procedure, even in the presence of many lesions, and a process that is reminiscent of the natural MC resolution (“BOTE” sign – for beginning of the end [19, 20]). The latter led us to hypothesize that overall aesthetic result and parents’ satisfaction would be higher in this group. However, we found higher aesthetic satisfaction rate, lower remnants rate, and a trend towards higher satisfaction from the healing process in the curettage compared with the ED group. Moreover, as the 2 groups differed in the sizes of the lesions (the curettage group included more patients with 5–10 mm lesions and the ED group included more patients with 0–3 mm lesions) the real difference might be larger in favour of the curettage. These findings may suggest that the inflammatory process induced by ED is different from the natural process that leads, in most cases, to resolution without remnants.
The recurrence rate of any MC lesion within our study population and after 6 weeks from the procedure was 43.6% (49.2% and 35% in the curettage and ED group, respectively). This rate was comparable to the work by Simonart et al. that reported a recurrence rate of 45% at an 8-week post-follow-up (21), and Harel et al. reported 30% recurrence post-curettage procedure (22). In contrast, Hanna et al. (23) had only 20% recurrence by curettage; however, only 10 lesions were treated. Importantly, both methods were effective in preventing high-volume recurrences (≥ 10 lesions), reinforcing their utility in managing MC. However, prior studies specifically evaluating recurrence rates for ED are lacking.
This study is subject to several limitations. Parent-driven selection of treatment modality introduces potential bias, as families may choose interventions based on personal preferences or preconceived beliefs regarding efficacy and pain, rather than randomized allocation. Randomized controlled trials directly comparing curettage and ED would offer more definitive evidence and stronger conclusions. Furthermore, reliance on subjective parental reports for complications such as remnants and infections may lead to over-interpretation, as post-inflammatory erythema or lesion inflammation could be misclassified as remnant/scarring or infection. Future studies should incorporate objective dermatological evaluations and longer follow-up periods to accurately gauge long-term complications.
Based on these findings, we propose that clinicians should potentially adopt curettage as the first-line treatment, while reserving ED for anatomically sensitive areas, such as the eyelids and lips, where greater precision is required. Further research is necessary to refine treatment protocols and optimize patient outcomes.
ACKNOWLEDGEMENTS
Ethical approval: Reviewed and approved by the Ethics Committee of Sheba Medical Center.
Ethics statement: The patients’ parents/guardians in this study have given written informed consent to the publication of their case details.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Braue A, Ross G, Varigos G, Kelly H. Epidemiology and impact of childhood molluscum contagiosum: a case series and critical review of the literature. Pediatr Dermatol 2005; 22: 287–294. https://doi.org/10.1111/j.1525-1470.2005.22401.x
- Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol 2014; 134: 1527–1534. https://doi.org/10.1038/jid.2013.446
- Gottlieb SL, Myskowski PL. Molluscum contagiosum. Int J Dermatol. 1994; 33: 453–461. https://doi.org/10.1111/j.1365-4362.1994.tb02853.x
- Basdag H, Rainer BM, Cohen BA. Molluscum contagiosum: to treat or not to treat? Experience with 170 children in an outpatient clinic setting in the northeastern United States. Pediatr Dermatol 2015; 32: 353-357. https://doi.org/10.1111/pde.12504
- Olsen JR, Gallacher J, Piguet V, Francis NA. Epidemiology of molluscum contagiosum in children: a systematic review. Fam Pract 2014; 31: 130–136. https://doi.org/10.1093/fampra/cmt075
- Koning S, Bruijnzeels MA, van Suijlekom-Smit LW, van der Wouden JC. Molluscum contagiosum in Dutch general practice. Br J Gen Pract J R Coll Gen Pract 1994; 44: 417–419.
- Villa L, Varela JA, Otero L, Sánchez C, Junquera ML, Río JS del, et al. Molluscum contagiosum: a 20-year study in a sexually transmitted infections unit. Sex Transm Dis 2010; 37: 423–424. https://doi.org/10.1097/OLQ.0b013e3181cfca1c
- McCollum AM, Holman RC, Hughes CM, Mehal JM, Folkema AM, Redd JT, et al. Molluscum contagiosum in a pediatric American Indian population: incidence and risk factors. PloS One 2014; 9: e103419. https://doi.org/10.1371/journal.pone.0103419
- Dohil MA, Lin P, Lee J, Lucky AW, Paller AS, Eichenfield LF. The epidemiology of molluscum contagiosum in children. J Am Acad Dermatol 2006; 54: 47–54. https://doi.org/10.1016/j.jaad.2005.08.035
- Silverberg NB. Pediatric molluscum: an update. Cutis 2019; 104: 301–305; E1; E2.
- Wollenberg A, Wetzel S, Burgdorf WHC, Haas J. Viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol 2003; 112: 667–674. https://doi.org/10.1016/j.jaci.2003.07.001
- Andre N, Jurban E, Alyagon A, Moskovich C, Kaplan O, Test G, et al. Facial vs non-facial molluscum contagiosum infection in children: a cross-sectional study. Acta Derm Venereol 2024; 104: adv40091. https://doi.org/10.2340/actadv.v104.40091
- Andre N, Alyagon A, Jurban E, Moscovici K, Horev A. Does molluscum contagiosum need to be managed differently in atopic children? Acta Derm Venereol 2024; 104: adv39983. https://doi.org/10.2340/actadv.v104.39983
- Olsen JR, Gallacher J, Finlay AY, Piguet V, Francis NA. Time to resolution and effect on quality of life of molluscum contagiosum in children in the UK: a prospective community cohort study. Lancet Infect Dis 2015; 15: 190–195. https://doi.org/10.1016/S1473-3099(14)71053-9
- van der Wouden JC, van der Sande R, Kruithof EJ, Sollie A, van Suijlekom-Smit LW, Koning S. Interventions for cutaneous molluscum contagiosum. Cochrane Database Syst Rev 2017; 2017: CD004767. https://doi.org/10.1002/14651858.CD004767.pub4
- Forbat E, Al-Niaimi F, Ali FR. Molluscum contagiosum: review and update on management. Pediatr Dermatol 2017; 34: 504–515. https://doi.org/10.1111/pde.13228
- Nguyen HP, Franz E, Stiegel KR, Hsu S, Tyring SK. Treatment of molluscum contagiosum in adult, pediatric, and immunodeficient populations. J Cutan Med Surg 2014; 18: 299–306. https://doi.org/10.2310/7750.2013.13133
- Molluscum Contagiosum Treatment & Management: Approach Considerations, Pharmacologic Therapy, Benign Neglect 2024 Jan 9 [cited 2025 Mar 24]. Available from: https://emedicine.medscape.com/article/910570-treatment#d12?form=fpf
- Butala N, Siegfried E, Weissler A. Molluscum BOTE sign: a predictor of imminent resolution. Pediatrics 2013; 131: e1650–1653. https://doi.org/10.1542/peds.2012-2933
- Sil A, Bhanja DB, Chandra A, Biswas SK. BOTE sign in molluscum contagiosum. BMJ Case Rep CP 2020; 13: e239142. https://doi.org/10.1136/bcr-2020-239142
- Simonart T, De Maertelaer V. Curettage treatment for molluscum contagiosum: a follow-up survey study. Br J Dermatol 2008; 159: 1144–1147. https://doi.org/10.1111/j.1365-2133.2008.08833.x
- Harel A, Kutz AM, Hadj-Rabia S, Mashiah J. To treat molluscum contagiosum or not – curettage: an effective, well-accepted treatment modality. Pediatr Dermatol 2016; 33: 640–645. https://doi.org/10.1111/pde.12968
- Hanna D, Hatami A, Powell J, Marcoux D, Maari C, Savard P, et al. A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children. Pediatr Dermatol 2006; 23: 574–579. https://doi.org/10.1111/j.1525-1470.2006.00313.x