ORIGINAL ARTICLE
Dipeptidyl Peptidase-4 Inhibitors Associated with Lower Psoriatic Disease Risk in Type 2 Diabetes: A 13-Year Nationwide Cohort Study with Mechanistic Validation
Chih-Tsung HUNG1  , Chi-Hsiang CHUNG2–4, Tsu-Hsuan WENG3 , Chun-Teng TSAI3 , Wu-Chien CHIEN2–6# and Yung-Lung CHANG7#
, Chi-Hsiang CHUNG2–4, Tsu-Hsuan WENG3 , Chun-Teng TSAI3 , Wu-Chien CHIEN2–6# and Yung-Lung CHANG7#
1Department of Dermatology, Tri-Service General Hospital, National Defense Medical University, Taipei, 2School of Public Health, National Defense Medical University, Taipei, 3Department of Medical Research, Tri-Service General Hospital, National Defense Medical University, Taipei, 4Taiwanese Injury Prevention and Safety Promotion Association, Taipei, 5Graduate Institute of Life Sciences, National Defense Medical University, Taipei, 6Graduate Institute of Medical Sciences, National Defense Medical University, Taipei, and 7Department of Biochemistry, National Defense Medical University, Taipei, Taiwan
#These authors contributed equally to this work.
Psoriatic disease, encompassing psoriasis and psoriatic arthritis, is a chronic inflammatory condition with bidirectional associations with type 2 diabetes mellitus. Current evidence regarding dipeptidyl peptidase-4 inhibitors’ effects on psoriatic disease presents conflicting findings, with the impact on psoriatic arthritis remaining unexplored. This study aimed to investigate the association between dipeptidyl peptidase-4 inhibitors use and psoriatic disease risk in diabetic patients. A nationwide population-based cohort study was conducted using Taiwan’s National Health Insurance Research Database (2009–2021), including 78,865 patients with type 2 diabetes mellitus: 15,773 dipeptidyl peptidase-4 inhibitors users and 63,092 matched controls. Primary outcomes were incident psoriasis and psoriatic arthritis. During a median follow-up of 7.08 years, 393 cases developed psoriatic disease: 51 cases in the dipeptidyl peptidase-4 inhibitors cohort vs 342 cases in controls. Dipeptidyl peptidase-4 inhibitors therapy was associated with significantly lower psoriatic disease risk (adjusted hazard ratio 0.583, 95% confidence interval 0.430–0.696). Individual dipeptidyl peptidase-4 inhibitors demonstrated varying protective effects, with alogliptin showing the strongest protection. In vitro experiments confirmed that dipeptidyl peptidase-4 inhibitors significantly attenuated inflammatory responses in human skin cells. This large-scale nationwide study demonstrates that dipeptidyl peptidase-4 inhibitors use is associated with a 41.7% lower risk in psoriatic disease in diabetic patients.
SIGNIFICANCE
Diabetes and skin diseases like psoriasis often occur together, creating health challenges for millions worldwide. Some diabetes medications might help protect against skin problems, but previous studies presented mixed results. We studied nearly 79,000 diabetes patients over 13 years and found that those taking specific diabetes drugs had a 42% lower risk of developing psoriasis or joint problems. Different medications showed varying levels of association. Laboratory tests indicated that these drugs may reduce skin inflammation. This means doctors could choose diabetes medications that control blood sugar while possibly reducing the risk of skin diseases, though clinical trials are needed.
Key words: dipeptidyl peptidase-4 inhibitors; psoriasis; psoriatic arthritis; population-based cohort study; type 2 diabetes mellitus.
Citation: Acta Derm Venereol 2025; 105: adv44343. DOI: https://doi.org/10.2340/actadv.v105.44343.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 8, 2025. Accepted after revision: Sep 18, 2025. Published: Nov 12, 2025.
Corr: Wu-Chien Chien, PhD, Department of Medical Research, Tri-Service General Hospital, National Defense Medical University, 7115R, No.325, Sec. 2, Chenggong Rd., Neihu Dist., Taipei City 114, Taiwan (R.O.C.), and Yung-Lung Chang, PhD, Department of Biochemistry, Tri-Service General Hospital, National Defense Medical University, No.325, Sec. 2, Chenggong Rd., Neihu Dist., Taipei City 114, Taiwan (R.O.C.). E-mails: chienwu@ndmctsgh.edu.tw; ylchang@mail.ndmctsgh.edu.tw
Competing interests and funding: The authors have no conflicts of interest to declare.
This study was supported by grants from Tri-Service General Hospital Research Foundation (TSGH-B-114022, TSGH-A-114010, TSGH-D-114196, TSGH-D-114164, and TSGH-E-114224). The funding source had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors also appreciate the Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW), Taiwan, for providing the National Health Insurance Research Database (NHIRD).
INTRODUCTION
Psoriatic disease (PsD) encompasses psoriasis (PsO) and psoriatic arthritis (PsA). It represents a chronic immune-mediated inflammatory condition affecting millions worldwide (1). In Taiwan, the epidemiological burden has increased substantially, with PsO prevalence rising from 0.18% to 0.86% between 2006 and 2017, while PsA prevalence increased from 0.01% to 0.08%, despite stable incidence rates (2). This inflammatory disorder demonstrates a well-established bidirectional relationship with type 2 diabetes mellitus (T2DM). PsO patients exhibit a 38% higher diabetes risk. Diabetic patients show a 40% increased PsO risk (3).
Dipeptidyl peptidase-4 inhibitors (DPP-4is) are widely prescribed antidiabetic medications. They have emerged as potential modulators of inflammatory diseases beyond their established glucose-lowering effects (4, 5). While DPP-4is paradoxically increase bullous pemphigoid risk, they demonstrate protective effects against various inflammatory skin conditions, including cutaneous lupus erythematosus, lichen planus, and atopic dermatitis (6).
However, current evidence regarding DPP-4is and PsO presents conflicting findings that warrant clarification. A nationwide Israeli study demonstrated increased PsO risk, showing a 2.12-fold elevated risk among DPP-4is users (95% CI 0.99–4.66) (7). Conversely, compelling clinical evidence supports protective effects, including a notable case report documenting complete psoriatic plaque resolution following 3 months of sitagliptin treatment (8). Large-scale epidemiological studies have similarly demonstrated reduced incident PsO among DPP-4is users (6, 9, 10). The DINUP trial further investigates sitagliptin’s therapeutic potential in PsO management (11).
Despite these emerging findings, critical knowledge gaps persist. First, most studies have utilized relatively short observation periods or earlier datasets. These may not reflect contemporary prescribing patterns and patient populations. Second, while research has focused exclusively on PsO, the effects on PsA remain completely unexplored. PsA affects approximately 30% of psoriasis patients and involves distinct inflammatory pathways. Third, differential effects among various DPP-4is subtypes are unclear. This limits clinical decision-making regarding optimal agent selection. Finally, mechanistic understanding lacks robust experimental validation to support the observed epidemiological associations.
Therefore, we conducted this comprehensive nationwide cohort study using Taiwan’s National Health Insurance Research Database (2009–2021). We investigated the association between DPP-4is use and PsD risk in patients with T2DM. Our study addresses these critical limitations by utilizing a comprehensive 13-year dataset. We expanded beyond previous research to examine both PsO and PsA as distinct outcomes, and comparing effects among different DPP-4is subtypes. We incorporated mechanistic validation t in vitro experiments exploring interleukin-17A (IL-17A)-induced inflammatory responses in human keratinocytes. This multifaceted approach aims to provide definitive evidence regarding DPP-4is effects on the entire spectrum of psoriatic disease and elucidate underlying mechanisms.
MATERIALS AND METHODS
Data sources
This study utilized Taiwan’s National Health Insurance Research Database (NHIRD). The NHIRD encompasses over 99% of the population through mandatory enrolment. It comprises comprehensive anonymized records including outpatient, inpatient, and emergency data. Diagnoses were coded using ICD-9-CM (2009–2015) and ICD-10-CM (2016–2021), with validated accuracy (12, 13). The study was approved by Tri-Service General Hospital Institutional Review Board (TSGHIRB No. E202516043).
Study design and participants
We conducted a population-based matched-cohort study of 78,865 patients with diabetes mellitus from the Longitudinal Health Insurance Database (2009–2021) (Fig. 1). Patients with diabetes mellitus (ICD-9-CM code 250; ICD-10-CM code E11) recorded ≥ 3 times in outpatient or once in inpatient settings were included. The exposed group comprised DPP-4i users (≥ 90 days treatment, n = 15,773) matched 1:4 w ith unexposed controls (n = 63,092) by age, gender, and index year. We excluded patients receiving GLP-1 receptor agonists, those with PsD before 2009 or before first diabetes mellitus visit, and patients < 18 years.
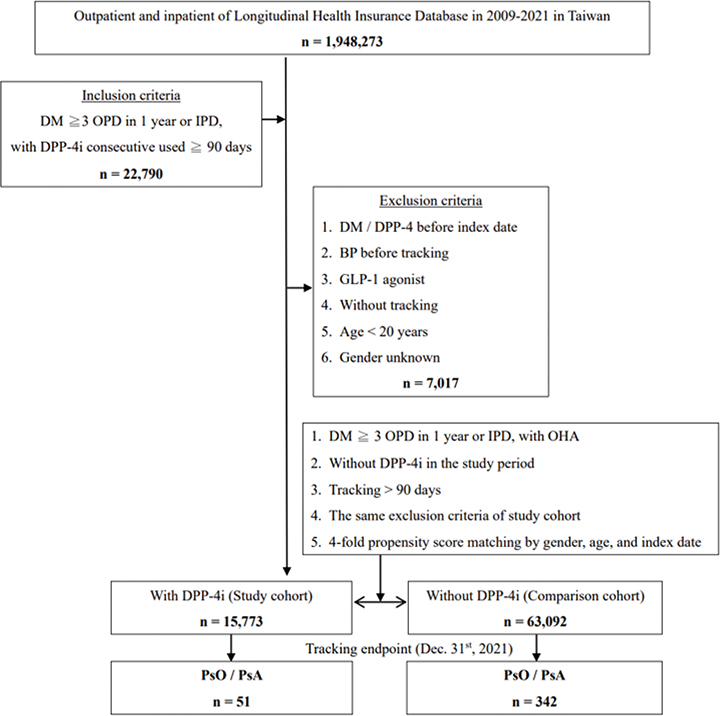
Fig. 1. Study population selection flowchart. Patient selection from Taiwan’s National Health Insurance Research Database (NHIRD) (2009–2021). From 1,948,273 patients in the Longitudinal Health Insurance Database (LHID), 22,790 met inclusion criteria (diabetes mellitus with dipeptidyl peptidase-4 inhibitors’ (DPP-4is) use ≥90 days). After applying exclusion criteria and 1:4 propensity score matching by gender, age, and index date, the final cohort comprised 15,773 DPP-4is users and 63,092 controls. During follow-up to December 2021, 51 psoriatic disease cases occurred in the DPP-4is group vs 342 in controls. NHIRD: National Health Insurance Research Database; LHID: Longitudinal Health Insurance Database; DPP-4is: dipeptidyl peptidase-4 inhibitors.
Outcome measures
Primary outcome was incident PsD, encompassing PsO (ICD-9-CM: 696.1; ICD-10-CM: L40.0, L40.4, L40.9) and PsA (ICD-9-CM: 696.0; ICD-10-CM: L40.5, L40.51, L40.52, L40.53, L40.54, L40.59). Follow-up extended from index date until PsD onset, insurance withdrawal, or 31 December 2021. Secondary analyses examined PsO and PsA separately.
Covariates
Variables included demographics (gender, age groups: 18–44, 45–64, ≥ 65 years), comorbidities assessed by Charlson Comorbidity Index revised (CCI_R, excluding diabetes) (14), healthcare utilization level, seasonality, urbanization level (4 levels), and geographic location. These covariates were included to control for potential confounding effects related to healthcare accessibility and resource distribution.
In vitro experimental validation
HaCaT human keratinocytes were cultured in Dulbecco’s Modified Eagle Medium at 37°C with 5% CO2. At 50–60% confluence, cells were treated with IL-17A (100 ng/ml) and/or DPP-4i (vildagliptin 5 µM, saxagliptin 0.5 µM). Gene expression of inflammatory markers (S100A7, IL-36γ, CXCL8, CCL20) was analysed by quantitative real-time polymerase chain reaction. Experiments were performed in triplicate with ≥ 3 independent replicates. Statistical significance was determined by analysis of variance with post hoc analysis (p < 0.05).
Statistical analysis
Statistical analyses used SPSS version 22 (IBM Corp, Armonk, NY, USA). Categorical and continuous variables were compared using χ2 and t-tests, respectively. Incidence rates were calculated per 100,000 person-years. Multivariable Cox proportional hazard models estimated hazard ratios (HRs) and 95% confidence intervals (CIs), adjusting for age, gender, comorbidity, season, location, urbanization, and care level. Cumulative incidence was evaluated using Kaplan–Meier analysis with log-rank tests. Statistical significance was set at p < 0.05. Subgroup analyses examined individual DPP-4i agents (alogliptin, linagliptin, saxagliptin, sitagliptin, vildagliptin) and disease subtypes separately.
RESULTS
Baseline characteristics
This cohort comprised 78,865 participants: 15,773 DPP-4i users and 63,092 controls. Demographics were well balanced between groups, with 51.85% male participants in both cohorts (p = 0.999). Mean age was comparable (DPP-4i: 64.13 ± 11.86 years vs controls: 64.10 ± 11.75 years, p=0.775). Age distribution showed a majority ≥ 65 years (56.91%), followed by 45–64 years (36.34%) and 18–44 years (6.75%) in both groups. CCI_R scores differed slightly but significantly between groups (0.84 ± 1.35 vs 0.80 ± 1.31, p < 0.001). Median follow-up was 7.15 years for DPP-4i users and 7.04 years for controls (Table I, Table SI).
Incidence and risk assessment of psoriatic disease
During follow-up, 393 patients (0.50%) developed PsD. There were 51 cases (0.32%) in the DPP-4i group vs 342 cases (0.54%) in controls. After multivariable adjustment for demographics, comorbidities, and healthcare factors, DPP-4i therapy was associated with significantly reduced PsD risk (adjusted HR 0.583, 95% CI 0.430–0.696, p < 0.001), representing a 41.7% risk reduction (Tables II and III).
Gender-stratified analyses demonstrated consistent protective effects in both sexes. Males showed aHR 0.589 (95% CI 0.436–0.704, p < 0.001), and females showed aHR 0.575 (95% CI 0.423–0.687, p < 0.001). Age-stratified analyses revealed significant risk reduction across all strata: 18–44 years (aHR 0.515, 95% CI 0.382–0.618), 45–64 years (aHR 0.597, 95% CI 0.441–0.714), and ≥ 65 years (aHR 0.580, 95% CI 0.430–0.697), all p < 0.001 (see Table III).
Individual DPP-4 inhibitor effects
Analysis of individual DPP-4i agents revealed varying degrees of protection. Alogliptin demonstrated the strongest effect (aHR 0.468, 95% CI 0.345–0.562, p < 0.001), followed by sitagliptin (aHR 0.505, 95% CI 0.372–0.607, p < 0.001), vildagliptin (aHR 0.563, 95% CI 0.418–0.674, p < 0.001), saxagliptin (aHR 0.602, 95% CI 0.445–0.719, p < 0.001), and linagliptin (aHR 0.769, 95% CI 0.567–0.922, p = 0.011) (Table IV).
Disease-specific analysis
DPP-4i therapy demonstrated protective effects against both psoriatic manifestations. For PsO, the aHR was 0.573 (95% CI 0.428–0.687, p < 0.001), while for PsA, the aHR was 0.630 (95% CI 0.462–0.751, p < 0.001). Incidence rates per 100,000 person-years were substantially lower in the DPP-4i group for both PsO (37.24 vs 63.77) and PsA (7.98 vs 12.49) (Table V).
Temporal analysis
Kaplan–Meier analysis revealed consistently lower cumulative PsD incidence in the DPP-4i cohort throughout the 13-year follow-up period. The protective effect was evident from year 1 (3 vs 28 cases, p < 0.001) and sustained through to year 13 (51 vs 342 cases, p < 0.001), indicating durable benefit (Fig. 2, Table SII).

Fig. 2. Kaplan–Meier survival analysis for psoriatic disease risk. Cumulative risk of psoriatic disease over 13 years in diabetes patients stratified by dipeptidyl peptidase-4 inhibitors (DPP-4is) treatment. Solid line: DPP-4is group (n = 15,773); dashed line: control group (n = 63,092). DPP-4is treatment demonstrated consistently lower cumulative incidence throughout follow-up (log-rank test p < 0.001).
In vitro mechanistic validation
IL-17A treatment significantly upregulated expression of psoriasis-associated inflammatory genes (S100A7, IL-36γ, CXCL8, CCL20) in HaCaT keratinocytes. Both vildagliptin and saxagliptin substantially attenuated these IL-17A-induced inflammatory responses (p < 0.05). Vildagliptin demonstrated slightly superior anti-inflammatory activity compared with saxagliptin. These findings provide mechanistic support for the protective effects observed in the clinical cohort (Fig. 3).
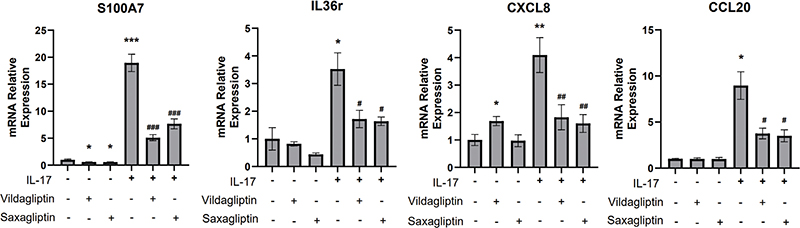
Fig. 3. Anti-inflammatory effects of dipeptidyl peptidase-4 inhibitors (DPP-4is) in human keratinocytes. Expression levels of inflammatory markers (S100 calcium-binding protein A7 [S100A7], interleukin-36 gamma [IL-36γ], C-X-C motif chemokine ligand 8 [CXCL8], C-C motif chemokine ligand 20 [CCL20]) in HaCaT cells treated with interleukin-17A (IL-17A) (100 ng/ml) ± DPP-4is (vildagliptin 5 µM, saxagliptin 0.5 µM). Both DPP-4is significantly attenuated IL-17A-induced inflammatory gene expression. Data presented as mean ± standard error of the mean (SEM) from 3 independent experiments. P < 0.05, *P < 0.01, **P < 0.001 vs. control; #P < 0.05, ##P < 0.01, ###P < 0.001 vs. IL-17A alone. S100A7: S100 calcium-binding protein A7; IL-36γ: interleukin-36 gamma; CXCL8: C-X-C motif chemokine ligand 8; CCL20: C-C motif chemokine ligand 20; IL-17A: interleukin-17A; DPP-4is: dipeptidyl peptidase-4 inhibitors; SEM: standard error of the mean.
DISCUSSION
This large-scale nationwide cohort study demonstrates that DPP-4i use is associated with a significantly reduced risk of developing PsD in patients with T2DM. The aHR was 0.583 (95% CI 0.430–0.696, p < 0.001), representing a 41.7% risk reduction. These findings provide important evidence regarding DPP-4i effects on PsD and address critical knowledge gaps in this evolving field.
Comparison with previous studies and novel findings
Previous research has yielded conflicting results. An Israeli study suggested increased PsO risk among DPP-4i users, with a 2.12-fold increased risk (95% CI 0.99–4.66, p = 0.050) (7). Conversely, clinical evidence supports protective effects, including complete resolution of psoriatic lesions after sitagliptin treatment (8). Clinical studies have reported that DPP-4i can reduce systemic inflammation levels and improve skin lesion severity in PsO patients (9, 15). Large-scale studies demonstrated reduced incident PsO among DPP-4i users, with Chen et al. reporting an aHR of 0.56 (95% CI 0.52–0.61) for psoriasis specifically (16). The DINUP trial evaluated sitagliptin efficacy in combination with narrow-band ultraviolet-B phototherapy for PsO treatment, demonstrating additional benefits with improved PASI scores (11).
Our findings align with protective effects, demonstrating consistent risk reduction. While previous studies focused exclusively on PsO, our study uniquely examined both PsO and PsA as distinct outcomes. We showed protective effects against both conditions: PsO (aHR 0.573, 95% CI 0.428–0.687, p < 0.001) and PsA (aHR 0.630, 95% CI 0.462–0.751, p < 0.001). This is particularly significant, as PsA affects approximately 30% of PsO patients and represents a distinct clinical entity previously unexplored in DPP-4i studies.
Differential effects among DPP-4i subtypes
Our study provides the first comprehensive comparison of different DPP-4i subtypes regarding PsD risk. We revealed significant differences: alogliptin (aHR 0.468), sitagliptin (aHR 0.505), vildagliptin (aHR 0.563), saxagliptin (aHR 0.602), and linagliptin (aHR 0.769). These differential effects may relate to variations in DPP-4 selectivity and pharmacokinetic profiles. Alogliptin’s high selectivity for DPP-4 may contribute to its superior protective effect (17). These differential effects among DPP-4i subtypes provide additional evidence supporting the observed association between DPP-4 inhibition and PsD risk reduction, though the underlying mechanisms require further investigation.
Mechanistic insights and experimental validation
Experimental evidence supports anti-inflammatory effects of DPP-4i through multiple mechanisms. Recent diabetic mouse models with imiquimod-induced psoriasis-like lesions showed that DPP-4i treatment reduced skin inflammation through MAPK/NF-κB pathway inhibition, decreasing inflammatory mediators including TNF-α, IL-1β, IL-17A, and IL-23 (18). Notably, DPP-4 expression and activity are dramatically upregulated in psoriatic skin, with 6.6-fold increased enzymatic activity and 11-fold elevated mRNA levels compared with normal skin (5).
Our in vitro studies demonstrated that both vildagliptin and saxagliptin significantly attenuated IL-17A-induced expression of key psoriatic inflammatory markers (S100A7, IL-36γ, CXCL8, CCL20) in human keratinocytes. Importantly, emerging research has highlighted skin–joint crosstalk mechanisms in psoriatic disease. Mellor et al. demonstrated that keratinocyte-derived S100A9 affects both skin and joint inflammation (19). Xu et al. showed that keratinocyte-secreted CXCL10 contributes to joint inflammation in psoriatic arthritis (20). These studies provide mechanistic support for how keratinocyte-targeted interventions could influence both manifestations of psoriatic disease.
The mechanistic evidence suggests DPP-4 inhibition modulates immunopathological processes through altering chemokine truncation and enhancing GLP-1 signalling pathways (21, 22). However, we acknowledge our experimental scope focused primarily on keratinocyte responses, and future research should include more comprehensive cellular models.
Clinical implications and limitations
The differential effects among DPP-4i suggest potential differences in protective mechanisms that warrant further investigation. The protective effects against both PsO and PsA suggest potential systemic benefits for the entire PsD spectrum. These observational findings generate hypotheses that require validation through randomized controlled trials before any clinical recommendations can be made. The consistency across all demographic subgroups and sustained protection throughout 13 years indicates the robustness of these associations, though causality cannot be established from observational data alone.
Several limitations should be acknowledged. Taiwan’s NHIRD lacks detailed clinical information including PsO severity scores, preventing assessment of disease severity-dependent effects. The database also does not contain data on important lifestyle factors such as smoking, weight, or income, which prevents adjustment for these potential confounders. This represents a significant limitation of our observational study design. The predominantly Taiwanese population may limit generalizability to other ethnic groups. Potential unmeasured confounders may influence observed associations despite statistical adjustment.
Regarding diagnostic accuracy, while ICD coding has inherent limitations, several well-regarded studies have successfully employed NHIRD for psoriasis and psoriatic arthritis epidemiological research, confirming the reliability of these diagnostic codes in large cohort studies (23, 24). The use of ICD-based definitions represents the standard methodology required for large database research. We acknowledge that PsA coding specificity may be particularly affected by underdiagnosis or misdiagnosis in clinical practice. However, any misclassification is likely non-differential between treatment groups and would tend to bias results toward the null, potentially leading to conservative estimates of the observed associations.
Our in vitro experimental approach focused primarily on keratinocyte inflammatory responses. While HaCaT cells have certain limitations including tumour origin and potential ethnic differences, they represent an internationally recognized model for studying psoriasis-related inflammatory mechanisms. The transformed nature of HaCaT cells and their Caucasian origin may limit direct extrapolation to primary Asian keratinocytes, and the single-cell model cannot capture the complex multicellular interactions involved in PsA pathogenesis. Future research should focus on prospective randomized controlled trials to establish causality, mechanistic studies using more comprehensive cellular models to explore effects on joints and systemic immune systems, and investigation of optimal dosing strategies for PsD prevention.
This nationwide cohort study provides robust evidence that DPP-4i use in diabetic patients is associated with significantly reduced risk of developing both PsO and PsA. Our findings extend beyond previous research by demonstrating differential effects among DPP-4i subtypes and including both cutaneous and articular manifestations of PsD. The results, supported by mechanistic evidence from cellular studies, suggest that DPP-4i may offer important benefits beyond glycaemic control in managing T2DM patients at risk of PsD. However, these observational findings require validation through randomized controlled trials before clinical practice recommendations can be made.
ACKNOWLEDGEMENTS
IRB approval status: The study was approved by Tri-Service General Hospital Institutional Review Board (TSGHIRB No. E202516043).
REFERENCES
- Boehncke WH, Schon MP. Psoriasis. Lancet 2015; 386: 983–994. https://doi.org/10.1016/S0140-6736(14)61909-7
- Iskandar IY, Teng-Chou C, Li-Chia C, Meng-Sui L, Yen-Yun Y, Ting-Chun W, et al. Incidence, prevalence, and mortality of people with psoriasis and psoriatic arthritis in Taiwan: a nationwide cohort study. Acta Derm Venereol 2022; 102: adv00807. https://doi.org/10.2340/actadv.v102.1962
- Chiu H-Y, Hung C-J, Muo C-H, Fan K-C, Sung F-C. The bidirectional association between type 2 diabetes and psoriasis: two retrospective cohort studies. Indian J Dermatol Venereol Leprol 2020; 86: 366. https://doi.org/10.4103/ijdvl.IJDVL_428_18
- Ohnuma K, Dang NH, Morimoto C. Revisiting an old acquaintance: CD26 and its molecular mechanisms in T cell function. Trends Immunol 2008; 29: 295–301. https://doi.org/10.1016/j.it.2008.02.010
- Van Lingen R, Van De Kerkhof P, Seyger M, De Jong E, Van Rens D, Poll M, et al. CD26/dipeptidyl-peptidase IV in psoriatic skin: upregulation and topographical changes. Br J Dermatol 2008; 158: 1264–1272. https://doi.org/10.1111/j.1365-2133.2008.08515.x
- Chiu H-Y, Huang Y-H. Dipeptidyl peptidase-4 inhibitors and the risk of chronic inflammatory skin diseases in type 2 diabetes mellitus in Taiwan: a nationwide population-based cohort study. J Invest Dermatol 2024; 144: 2321–2324. https://doi.org/10.1016/j.jid.2024.03.017
- Kridin K, Amber K, Khamaisi M, Comaneshter D, Batat E, Cohen AD. Is there an association between dipeptidyl peptidase-4 inhibitors and autoimmune disease? A population-based study. Immunol Res 2018; 66: 425–430. https://doi.org/10.1007/s12026-018-9005-8
- Nishioka T, Shinohara M, Tanimoto N, Kumagai C, Hashimoto K. Sitagliptin, a dipeptidyl peptidase-IV inhibitor, improves psoriasis. Dermatology 2012; 224: 20–21. https://doi.org/10.1159/000333358
- Lynch M, Malara A, Timoney I, Ahern T, Awdeh F, Sweeney C, et al. Dipeptidyl peptidase-4 inhibition in psoriasis patients with diabetes: a double-blind randomized controlled trial. Dermatology 2021; 237: 66–69. https://doi.org/10.1159/000502130
- Kim SC, Schneeweiss S, Glynn RJ, Doherty M, Goldfine AB, Solomon DH. Dipeptidyl peptidase-4 inhibitors in type 2 diabetes may reduce the risk of autoimmune diseases: a population-based cohort study. Ann Rheum Dis 2015; 74: 1968–1975. https://doi.org/10.1136/annrheumdis-2014-205216
- Lynch M, Ahern TB, Timoney I, Sweeney C, Kelly G, Hughes R, et al. Dipeptidyl peptidase-4 inhibition and narrow-band ultraviolet-B light in psoriasis (DINUP): study protocol for a randomised controlled trial. Trials 2016; 17: 1–10. https://doi.org/10.1186/s13063-016-1157-z
- Cheng CL, Lee CH, Chen PS, Li YH, Lin SJ, Yang YH. Validation of acute myocardial infarction cases in the national health insurance research database in taiwan. J Epidemiol 2014; 24: 500–507. https://doi.org/10.2188/jea.JE20140076
- Cheng CL, Chien HC, Lee CH, Lin SJ, Yang YH. Validity of in-hospital mortality data among patients with acute myocardial infarction or stroke in National Health Insurance Research Database in Taiwan. Int J Cardiol 2015; 201: 96–101. https://doi.org/10.1016/j.ijcard.2015.07.075
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373–383. https://doi.org/10.1016/0021-9681(87)90171-8
- Lynch M, Tobin AM, Ahern T, O’Shea D, Kirby B. Sitagliptin for severe psoriasis. Clin Exp Dermatol 2014; 39: 841–842. https://doi.org/10.1111/ced.12408
- Chen Y-C, Chen T-H, Sun C-C, Chen J-Y, Chang S-S, Yeung L, et al. Dipeptidyl peptidase-4 inhibitors and the risks of autoimmune diseases in type 2 diabetes mellitus patients in Taiwan: a nationwide population-based cohort study. Acta Diabetol 2020; 57: 1181–1192. https://doi.org/10.1007/s00592-020-01533-5
- Feng J, Zhang Z, Wallace MB, Stafford JA, Kaldor SW, Kassel DB, et al. Discovery of alogliptin: a potent, selective, bioavailable, and efficacious inhibitor of dipeptidyl peptidase IV. J Med Chem 2007; 50: 2297–2300. https://doi.org/10.1021/jm070104l
- Shao Z, Li X, Xu X, Chen P. DPP-4 inhibitor linagliptin ameliorates imiquimod-induced psoriasis-like skin alterations in type 2 diabetic mice by inhibiting the MAPK/NF-κB inflammatory pathway. Drug Dev Res 2022; 83: 1373–1382. https://doi.org/10.1002/ddr.21966
- Mellor LF, Gago-Lopez N, Bakiri L, Schmidt FN, Busse B, Rauber S, et al. Keratinocyte-derived S100A9 modulates neutrophil infiltration and affects psoriasis-like skin and joint disease. Ann Rheum Dis 2022; 81: 1400–1408. https://doi.org/10.1136/annrheumdis-2022-222229
- Xu F, Cui YZ, Yang XY, Zheng YX, Chen XB, Zhou H, et al. CXCL10 secreted by SPRY1-deficient epidermal keratinocytes fuels joint inflammation in psoriatic arthritis via CD14 signaling. J Clin Invest 2025; 135. https://doi.org/10.1172/JCI186135
- Proost P, De Meester I, Schols D, Struyf S, Lambeir A-M, Wuyts A, et al. Amino-terminal truncation of chemokines by CD26/dipeptidyl-peptidase IV: conversion of RANTES into a potent inhibitor of monocyte chemotaxis and HIV-1-infection. J Biol Chem 1998; 273: 7222–7227. https://doi.org/10.1074/jbc.273.13.7222
- Tian L, Gao J, Hao J, Zhang Y, Yi H, O’Brien TD, et al. Reversal of new-onset diabetes through modulating inflammation and stimulating β-cell replication in nonobese diabetic mice by a dipeptidyl peptidase IV inhibitor. Endocrinology 2010; 151: 3049–3060. https://doi.org/10.1210/en.2010-0068
- Iskandar IYK, Chen TC, Chen LC, Lee MS, Yang YY, Wang TC, et al. Incidence, prevalence, and mortality of people with psoriasis and psoriatic arthritis in Taiwan: a nationwide cohort study. Acta Derm Venereol 2022; 102: adv00807. https://doi.org/10.2340/actadv.v102.1962
- Jensen P, Ahlehoff O, Egeberg A, Gislason G, Hansen PR, Skov L. Psoriasis and new-onset depression: a Danish nationwide cohort study. Acta Derm Venereol 2016; 96: 39–42. https://doi.org/10.2340/00015555-2183