SHORT COMMUNICATION
Functional Brain Imaging Reveals Reconstitution of the Central Nervous Itch Network Upon Rifampicin Therapy in Hepatobiliary Pruritus
Marcel VETTER1,2, Theresa BUCHWALD1–3, Arnd DÖRFLER4, Clemens FORSTER3# and Andreas E. KREMER1,2,5#*
1Department of Medicine 1, Friedrich-Alexander-University Erlangen-Nürnberg and University Hospital Erlangen, Erlangen, 2Deutsches Zentrum Immuntherapie, DZI Erlangen, Erlangen, 3Institute of Physiology and Pathophysiology, Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, 4Department of Neuroradiology, Friedrich-Alexander-University Erlangen-Nürnberg and University Hospital Erlangen, Erlangen, Germany, and 5Department of Gastroenterology and Hepatology, University Hospital Zürich, University of Zürich, Zürich, Switzerland.
*E-mail: andreas.kremer@usz.ch
#Contributed equally
Citation: Acta Derm Venereol 2025; 105: adv44350. DOI: https://doi.org/10.2340/actadv.v105.44350.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 12, 2025. Accepted after revision: Oct 24, 2025. Published: Nov 25, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by the German Research Council (DFG) within the FOR2690 to AEK (KR3618/3-1 and KR3618/3-2), the Interdisciplinary Center for Clinical Research (IZKF) Erlangen to AEK, and the German Society for Internal Medicine (DGIM) by the advanced clinician scientist programme to AEK.
INTRODUCTION
Various hepatobiliary diseases are accompanied by chronic pruritus, which can dramatically reduce the quality of life of affected patients. Up to 70% of patients with primary biliary cholangitis and primary sclerosing cholangitis develop pruritus during the course of their disease (1). The detailed pathophysiology of hepatobiliary pruritus remains enigmatic. Levels of the lysophospholipase autotaxin (ATX) correlated with itch intensity and response to some therapeutic interventions (2). Rifampicin, an oral pregnane X receptor (PXR) agonist has proven to inhibit ATX expression in vitro. Clinically, rifampicin is employed as a potent second-line treatment for cholestatic pruritus, particularly in cases where bile acid sequestrants or fibrates prove ineffective (3).
Central nervous processing of pruritus involves the thalamus, insular cortex, caudate nucleus, orbitofrontal regions, sensory cortex (S2), and periaqueductal gray (4). Functional connections between areas of the central nervous system can be studied by functional MRI (fMRI) (5). Using this technique, it could be proven that itch in patients with primary biliary cholangitis changes functional connectivities within associated brain areas (6). In this exploratory study, we used fMRI for the first time in patients with hepatobiliary pruritus before and after effective antipruritic therapy. The aim of this study was to explore the reversibility of the central nervous itch network.
METHODS
We studied 3 patients (2 patients with PSC and 1 patient with benign recurrent intrahepatic cholestasis [BRIC]) with moderate to severe intensity of hepatobiliary pruritus despite ongoing therapy with cholestyramine. Anion exchange resin therapy was stopped and rifampicin started at doses of 150–300 mg once daily. The first fMRI session was performed the day before therapy started; the second fMRI session was after 4 weeks of therapy. Table I summarizes patient characteristics.
Itch intensity was quantified before and after therapy using a visual analogue scale, which ranged from 0 (no itch) to 10 (worst imaginable itch). Both the average intensity and the worst itch intensity were recorded.
MR imaging was performed on a 3 T Siemens MAGNETOM Trio Tim scanner (Siemens, Erlangen, Germany). To minimize head motions, subjects’ heads were fixed with rubber pads: participants were instructed to keep their eyes closed, and ear plugs were provided for noise reduction. Functional imaging was conducted using the echo planar imaging (EPI) sequence, acquiring 110 whole-brain T2*-weighted images of the cortex with a temporal resolution of 3 s. The resting state was assessed from these blood-oxygen-level-dependent (BOLD) sensitive MRIs in the absence of external stimulation.
The strength of functional connectivity between brain regions was measured by the correlation of the BOLD signal. Previous findings have demonstrated that the left posterior insular cortex (IC), the left thalamus, and the periaqueductal gray (PAG) represent key regions in the central processing of pruritic input The posterior IC is probably the most important projection field of the afferent pathway from peripheral C-fibres to the cerebral cortex and receives input from the thalamus. The PAG, in turn, constitutes a central region of the descending modulation of both itch and pain (6). On this basis, those regions were selected a priori as reference (seed regions) for the present analysis (7). Prior to the analysis, the individual BOLD signals were extracted from these regions and used as predictors to perform general linear models analyses. This resulted in statistical T-values that described the strength of the connectivity between the reference region and the analysed regions (endpoints). In a second analysis, the changes in these connectivities (contrasts) under successful therapy were determined. All postprocessing and statistical analyses were performed using BrainVoyager QX 2.6 (Brain Innovation, Maastricht, The Netherlands).
The significance threshold was adjusted using the Bonferroni correction according to the number of endpoints analysed: number of connectivities studied (n = 28) x number of analyses per connectivity (n = 3; before treatment, after treatment, contrast of both measurements) = 81 (p = 0.000596; critical T-value: ±4.3320).
RESULTS
Rifampicin at doses of 150–300 mg once daily strongly ameliorated pruritus within 4 weeks of treatment. The worst-itch intensity dropped from 9.1 to 5.8 (Fig. 1A). Similarly, itch intensity within the last 24h declined from 6.3 to 1.0 (Fig 1B). None of the patients reported any adverse events.
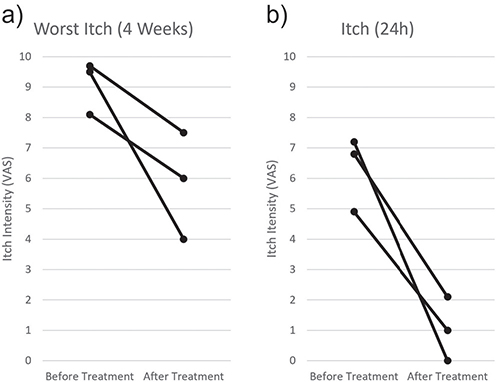
Fig. 1. Intensity of itch before and after treatment with rifampicin. (A) Worst pruritus intensity within the last 4 weeks before and after treatment with rifampicin. (B) Itch intensity 24 h before pre- and post-therapeutic fMRI. VAS: visual analogue scale, n = 3.
Functional connectivities involved in pruritus increased between various areas of the CNS after successful antipruritic therapy. Compared with pre-treatment, connectivities increased between the seed region thalamus and orbitofrontal region (left), anterior cingulate cortex, caudate (bilateral), and posterior insular cortex (bilateral). Similarly, the connectivities between the seed region left insular cortex and the orbitofrontal region (bilateral), anterior cingulate cortex, caudate (bilateral), and insula increased after therapy. Finally, we observed significant increases in connectivity between the PAG and the thalamus (right) and the posterior insular cortex (bilateral). Intriguingly, we did not observe any significant changes in the connectivities to the secondary somatosensory cortex (S2) (Fig. 2).
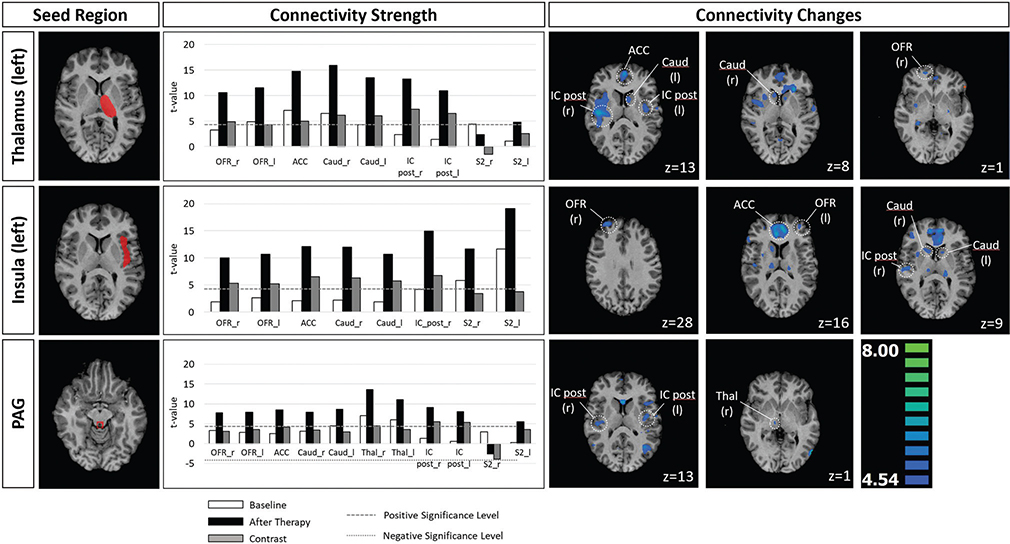
Fig. 2. Strength and changes (contrasts) of connectivities between brain regions before and after antipruritic therapy using the reference regions thalamus (left), posterior insula (left), and periductal gray (PAG). A positive value of the contrasts depicts an increase in connectivity between the seed region and the respective region after therapy. The dotted and dashed lines mark the statistical thresholds. Bars outside of this corridor are statistically significant. For those areas contrast of BOLD signals before and after treatment are shown. The height of the cross-section is defined by the z-coordinate according to the Talairach coordinate system. r: right, l: left, OFR: orbitofrontal region, ACC: anterior cingulate cortex, Caud: cauda, IC: insular cortex, S2: somatosensory cortex S2, Thal: thalamus, n = 3.
DISCUSSION
Chronic hepatobiliary pruritus is a debilitating symptom in many hepatobiliary disorders, particularly those with cholestatic features. Effective therapeutic options are limited, but rifampicin has proven efficacy in several placebo-controlled trials with complete or partial remission in 77% of cases (8). Rifampicin therapy also ameliorated pruritus in our study and was accompanied by increased connectivities between CNS areas involved in pruritus.
It has been reported that patients with chronic pruritus secondary to atopic dermatitis have reduced connectivities between CNS areas involved in pruritus (9). There is evidence that this association is also found in hepatobiliary pruritus and could be a kind of central sensitization to itch similar to a central sensitization for chronic pain (6, 10). The augmented connectivity between CNS regions involved in pruritus after effective therapy with rifampicin could thus be interpreted as a reconstitution of the original status. The data from this proof of principle study suggest that image morphology correlates with reversibility of hepatobiliary pruritus. Given the absence of established objective biomarkers for itch intensity and its modulation during therapy, the application of fMRI may provide particular value in the context of clinical trials. Nevertheless, fMRI should not be regarded as a replacement for clinical rating scales but rather as an objective and complementary tool to support and enrich patient-reported outcomes.
Our preliminary study is limited due to low patient numbers and the use of a single anti-pruritic therapy. We cannot fully exclude an off-target effect of rifampicin on the CNS independent of the reduction of pruritus. However, the highly significant results in only 3 patients studied underline a strong effect. A potential influence of habituation on the results of the second fMRI measurement cannot be ruled out. Further comprehensive studies with larger patient numbers, a control group, and use of multiple antipruritic agents are warranted to confirm these results.
In conclusion, our data suggest for the first time reversibility of central nervous changes after effective therapy for hepatobiliary pruritus. Functional connectivity investigated by fMRI could be suitable to objectify response to anti-pruritic therapies in clinical trials. Our data warrant further investigations of these brain-imaging studies in lager cohorts.
ACKNOWLEDGEMENT
The authors would like to thank Marilisa Hoche for taking care of patients regarding performance of the fMRI measurements.
Statements of ethics: The study protocol conformed to the ethical guidelines of the revised Declaration of Helsinki (2013, Fortalezza) and was approved by the local Ethics Committee at the Friedrich-Alexander University Erlangen-Nürnberg (file number 327_17B). All patients provided written informed consent before enrolment.
REFERENCES
- Kremer AE, Mettang T, Weisshaar E. Non-dermatological challenges of chronic itch. Acta Derm Venereol 2020; 100: adv00025. https://doi.org/10.2340/00015555-3345
- Kremer AE, van Dijk R, Leckie P, Schaap FG, Kuiper EM, Mettang T, et al. Serum autotaxin is increased in pruritus of cholestasis, but not of other origin, and responds to therapeutic interventions. Hepatology 2012; 56: 1391–1400. https://doi.org/10.1002/hep.25748
- Tandon P, Rowe BH, Vandermeer B, Bain VG. The efficacy and safety of bile acid binding agents, opioid antagonists, or rifampin in the treatment of cholestasis-associated pruritus. Am J Gastroenterol 2007; 102: 1528–1536. https://doi.org/10.1111/j.1572-0241.2007.01200.x
- Najafi P, Carré J-L, Ben Salem D, Brenaut E, Misery L, Dufor O. Central mechanisms of itch: a systematic literature review and meta-analysis. J Neuroradiol 2020; 47: 450–457. https://doi.org/10.1016/j.neurad.2019.11.005
- Cheddad El Aouni M, Ben Salem D, Misery L. Functional MRI of pruritus. J Neuroradiol 2020; 47: 400–401. https://doi.org/10.1016/j.neurad.2020.09.001
- Mosher VAL, Swain MG, Pang JXQ, Kaplan GG, Sharkey KA, MacQueen GM, et al. Primary biliary cholangitis alters functional connections of the brain’s deep gray matter. Clin Transl Gastroenterol 2017; 8: e107. https://doi.org/10.1038/ctg.2017.34
- Vierow V, Forster C, Vogelgsang R, Dörfler A, Handwerker HO. Cerebral networks linked to itch-related sensations induced by histamine and capsaicin. Acta Derm Venereol 2015; 95: 645–652. https://doi.org/10.2340/00015555-2006
- Khurana S, Singh P. Rifampin is safe for treatment of pruritus due to chronic cholestasis: a meta-analysis of prospective randomized-controlled trials. Liver Int 2006; 26: 943–948. https://doi.org/10.1111/j.1478-3231.2006.01326.x
- Desbordes G, Li A, Loggia ML, Kim J, Schalock PC, Lerner E, et al. Evoked itch perception is associated with changes in functional brain connectivity. Neuroimage Clin 2015; 7: 213–221. https://doi.org/10.1016/j.nicl.2014.12.002
- Arendt-Nielsen L, Morlion B, Perrot S, Dahan A, Dickenson A, Kress HG, et al. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain 2018; 22: 216–241. https://doi.org/10.1002/ejp.1140