SHORT COMMUNICATION
Cutaneous Graft-Versus-Host Disease Lichen Spinulosus-like: a New Form of Presentation of an Old Entity
Andrés VIDAL GONZÁLEZ1  , Laura TABOADA PAZ2, Sergio LÓPEZ ALCÁZAR1, Luis REQUENA CABALLERO3 and Marta FEITO RODRÍGUEZ1
, Laura TABOADA PAZ2, Sergio LÓPEZ ALCÁZAR1, Luis REQUENA CABALLERO3 and Marta FEITO RODRÍGUEZ1
1Dermatology, Hospital Universitario La Paz, Madrid, 2Dermatology, Complejo Hospitalario Universitario de Ferrol, Ferrol (A Coruña), and 3Dermatology, Fundación Jiménez Díaz, Madrid, Spain. E-mail: andresvidal97@gmail.com
Citation: Acta Derm Venereol 2025; 105: adv44373. DOI: https://doi.org/10.2340/actadv.v105.44373.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 10, 2025. Accepted after revision: Aug 19, 2025. Published: Sep 30, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Graft-versus-host disease (GVHD) remains a complex condition with a challenging diagnosis, in which dermatologists play a key role due to its frequent and varied cutaneous manifestations (1). We present the finding of hyperkeratotic spicules in an allotransplanted patient, compatible with an atypical variant of graft-versus-host disease (GVHD). Paediatric transplants represent 30% or less of all allogeneic stem cell transplants (SCT) performed worldwide (2). Advances in supportive care have significantly reduced early transplant-related mortality, thereby increasing the focus on long-term complications in these patients. Despite the efforts to reduce its incidence, chronic graft-versus-host disease (cGVHD) still affects around 50% of allogeneic HSCT recipients. The skin is the most commonly involved organ in cGVHD (3), lichen planus-like lesions and sclerotic changes being the most distinctive cutaneous features. However, less frequently, we may find atypical skin manifestations that can hinder diagnosis and proper management.
CASE REPORT
A 13-year-old girl had a history of extramedullary acute myeloid leukaemia diagnosed in 2019; hematopoietic progenitor transplantation was performed in March 2023 due to the failure of multiple lines of chemotherapy. She presented with grade IV GVHD with gastrointestinal and skin involvement in April 2023, showing good response to ruxolitinib and extracorporeal photopheresis.
In September 2023 the patient was referred to Dermatology for hyperkeratotic folliculocentric and spiculated lesions on erythematous plaques predominantly on the face, of evolution over weeks, resembling lichen spinulosus (Fig. 1). Subsequently, she presented extra-facial extension, with lesions on the neckline, back, pubis, and proximal region of the limbs. The patient had a history of unsuccessful treatments for seborrheic dermatitis and demodicosis, including topical corticosteroids (0.1% methylprednisolone cream), 1% pimecrolimus, and oral ivermectin. Differential diagnosis between lichen spinulosus, trichodysplasia spinulosa, and spicules associated with paraproteinemia was suggested. The biopsy showed compact parakeratotic hyperkeratosis in the infundibular exit with melanophagia in the basal layer (Fig. 2) and ruled out the presence of polyomavirus and nonspecific immunofixation for immunoglobulins (4). Eventually, she developed clinical manifestations compatible with enterocolitis and gastrointestinal involvement due to GVHD.

Fig. 1. (A, B) Folliculocentric hyperkeratotic spiculated lesions on erythematous plaques on the face and thorax. c-Spiny protrusions reminiscent of lichen spinulosus seen in more detail with dermoscopy.
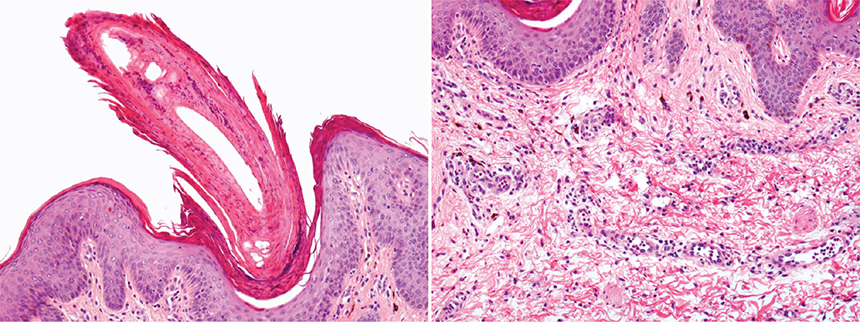
Fig. 2. (A) Compact parakeratotic hyperkeratosis in the infundibular exit (H&E, 100×). (B) Perivascular infiltrate composed of lymphocytes in the superficial middle dermis with intense melanophagia.
Reviewing the temporal sequence, we observed that the skin findings appeared following a dose reduction of ruxolitinib (from 2.5 mg BID to 2.5 mg QD) and improved markedly with the intensification of immunosuppression with oral methylprednisolone, photopheresis, and ruxolitinib (Fig. 3). This finding, together with the forms of follicular keratosis pilaris-like GVHD described in the literature, led us to confirm that we were dealing with an atypical variant of GVHD.

Fig. 3. (A, B) Complete resolution of the lesions after the introduction of an immunosuppressive regime with methylprednisolone, photopheresis, and ruxolitinib.
DISCUSSION
Graft-versus-host disease is a frequent complication following allogeneic stem cell transplantation (SCT), occurring in over 50% of cases, influenced by both donor and recipient characteristics (5). GVHD typically manifests in 2 forms: an acute presentation occurring from days to weeks post-allogeneic SCT, or a chronic form that emerges months to years later. Acute GVHD commonly presents as a morbilliform erythematous rash, often accompanied by fever, diarrhoea, and elevated liver enzymes. In contrast, cGVHD is a more variable condition (6).
Cutaneous GVHD has historically been categorized into lichenoid and sclerodermoid variants. However, early manifestations can be subtle, and, even in children, a wide range of atypical skin presentations may also be encountered (7). These manifestations may include vitiligoid, poikiloderma, papulosquamous, and keratosis pilaris-like eruptions. These atypical cutaneous findings, mimicking other skin conditions, should lead dermatologists to have a high clinical suspicion for GVHD in patients with stem cell transplantation.
Regarding this distinct follicular distribution, several studies have proposed the existence of a form of follicular GVHD in the adult population. Sale and Beauchamp suggest the hair follicle bulge as an early GVHD target (8). Follicular involvement is an almost constant histopathological finding in GVHD; however, cases where follicular eruptions are the primary clinical manifestation in either acute or chronic GVHD have rarely been reported. Some of these reports include the comedonal variant, with follicular lesions that may resemble closed and open acne-like comedones (9). Other variants include keratosis pilaris-like eruptions, with erythematous follicular papules evolving into old scaly papules (5, 10). Additionally clinical manifestations combining lichenoid and keratosis pilaris-like eruption have also been described (11). While several adult cases of follicular GVHD have been described, we were unable to find any published reports specifically documenting folliculocentric chronic GVHD in paediatric patients. Though keratosis pilaris-like GVHD is briefly mentioned in some studies (12), to our knowledge this is the first reported case of cGVHD mimicking lichen spinulosus.
The primary differential diagnosis is trichodysplasia spinulosa, a rare skin disease in immunocompromised patients caused by active infection with TSPyV polyomavirus, leading to characteristic follicular papules and spines. Nonetheless, we ruled out this diagnosis, considering that the biopsy did not show compatible histology (eosinophilic trichohyalin protein deposits in the inner root sheath) and was negative for TSPyV immunohistochemistry. Moreover, the intensification of the immunosuppressive regimen would lead to a worsening of trychodysplasia lesions, not an improvement, as we can appreciate in our case. Another skin entities that may present with spiny protrusions includes folliculotropic mycosis fungoides (13) and multiple myeloma (14).
One of the difficulties in the diagnosis of these atypical variants of cGVHD is clinicopathological correlation. Traditionally, the histological diagnosis of acute GVHD was based on the presence of basal apoptosis, with or without lichenoid infiltrate. Chronic GVHD appears as a pleomorphic disorder with protean morphological clinical patterns including eczematoid, psoriasiform, erythrodermic, lupus erythematous-like, and keratosis pilaris-like eruption (1). Collaboration between dermatologists and pathologists is essential to reach a diagnosis.
First-line treatment typically involves systemic corticosteroids, but long-term use can lead to significant side effects, and many patients become steroid-refractory or dependent, necessitating additional therapies. Skin-directed treatments such as topical corticosteroids, topical calcineurin inhibitors, and phototherapy have demonstrated efficacy in improving skin symptoms and reducing the need for systemic immunosuppression (15). For more severe or refractory cases, systemic agents such as immunomodulatory drugs, kinase inhibitors, extracorporeal photopheresis, as we have used in our case, are increasingly employed, though optimal sequencing and selection remain areas of ongoing research. There is no universally agreed treatment algorithm, and management is often personalized based on organ involvement and patient response.
In conclusion, this case highlights a rare and atypical presentation of chronic graft-versus-host disease in a paediatric patient, manifesting with lichen spinulosus-like cutaneous lesions. It underscores the importance of maintaining a high index of suspicion for cGVHD in patients with unusual skin findings following stem cell transplantation, especially when conventional treatments for other dermatologic conditions fail.
Accurate diagnosis requires close clinicopathological correlation and multidisciplinary collaboration, particularly between dermatology and pathology. Given the variability in clinical presentation and the absence of standardized treatment algorithms, recognizing and reporting such atypical variants is essential to improving diagnostic accuracy and optimizing patient care in paediatric cGVHD.
ACKNOWLEDGEMENTS
Consent statement: All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication.
Data availability statement: The data that support the findings of this study are available on request from the corresponding author.
REFERENCES
- Kim S, Choi J, Kim J, Cho B, Kim DW, Park H. Clinicopathologic characteristics of cutaneous chronic graft-versus- host diseases: a retrospective study in Korean patients. Int J Dermatology 2010; 49: 1386–1392. https://doi.org/10.1111/j.1365-4632.2010.04552.x
- Haroun E, Agrawal K, Leibovitch J, Kassab J, Zoghbi M, Dutta D, Lim SH. Chronic graft- versus-host disease in pediatric patients: differences and challenges. Blood Rev 2023; 60: 101054. https://doi.org/10.1016/j.blre.2023.101054
- Wolff D, Radojcic V, Lafyatis R, Cinar R, Rosenstein RK, Cowen EWet al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: IV. The 2020 Highly morbid forms report. Transplant Cell Ther 2021; 27: 817–835. https://doi.org/10.1016/j.jtct.2021.06.001
- Requena L, Sarasa JL, Masllorens FO, et al. Follicular spicules of the nose: a peculiar cutaneous manifestation of multiple myeloma with cryoglobulinemia. J Am Acad Dermatol 1995; 32: 834–839. https://doi.org/10.1016/0190-9622(95)91542-7
- Cornejo CM, Kim EJ, Rosenbach M, Micheletti RG. Atypical manifestations of graft-versus-host disease. J Am Acad Dermatol 2015; 72: 690–695. https://doi.org/10.1016/j.jaad.2014.12.022
- Peñas PF, Zaman S. Many faces of graft-versus-host disease. Aust J Dermatology 2010; 51: 1–10. https://doi.org/10.1111/j.1440-0960.2009.00577.x
- Nanda A, Husain MAA, Al-Herz W, Almekaimi A, Al-Sabah H, Al-Otaibi M. Chronic cutaneous graft-versus-host disease in children: a report of 14 patients from a tertiary care pediatric dermatology clinic. Pediatr Dermatol 2018; 35: 343–353. https://doi.org/10.1111/pde.13432
- Sale GE, Beauchamp M. Parafollicular hair bulge in human GVHD: a stem cell-rich primary target. Bone Marrow Transplant 1993; 11: 223–225.
- Llamas-Velasco M, Solano-López Morel GE, Gruber-Wackernagel A, Concha-Garzón MJ, Requena L, Cerroni L. Comedonal graft-vs-host disease: a distinct clinical expression of a lichenoid follicular GVHD. J Cutan Pathol 2014; 41: 853–858. https://doi.org/10.1111/cup.12391
- Vashisht D, Kothari R, Baveja S, Neema S, Sengupta P, Sandhu S. Follicular graft vs host reaction: a rare presentation. Indian Dermatol Online J 2020; 11: 988. https://doi.org/10.4103/idoj.IDOJ_87_20
- Martí N, Martin JM, Monteagudo C, López V, Jordá E. Follicular graft-versus-host disease: a rare manifestation of chronic cutaneous graft-versus-host disease. Am J Dermatopathol 2008; 30: 620–621. https://doi.org/10.1097/DAD.0b013e3181855701
- Baird K, Cooke K, Schultz KR. Chronic graft versus host disease (GVHD) in children. Pediatr Clin North Am 2010; 57: 297–322. https://doi.org/10.1016/j.pcl.2009.11.003
- Tomasini C, Michelerio A, Quaglino P. Spiky/keratosis-pilaris-like early follicular mycosis fungoides: a clinicopatho-logic study of 20 cases with extended follow-up. J Cutan Pathol 2021; 48: 1124–1132. https://doi.org/10.1111/cup.14002
- Smith MP, Manabat-Hidalgo C. Follicular spicules of multiple myeloma. Dermatol Online J 2019; 25: 11. https://doi.org/10.5070/D32510045822
- Strong Rodrigues K, Oliveira-Ribeiro C, de Abreu Fiuza Gomes S, Knobler R. Cutaneous graft-versus-host disease: diagnosis and treatment. Am J Clin Dermatol 2018; 19: 33–50. https://doi.org/10.1007/s40257-017-0306-9