ORIGINAL REPORT
Prevalence of Steatotic Liver Disease with Fibrosis and Diagnostic Screening Tools in Patients with Psoriasis
Charlotte NÄSLUND-KOCH1  , Marianne B. Løvendorf1,2 , Helene M. MARTIN1 , Mila B. JOHANSEN1,3 , Morten B. TRELLE4,5 , Claus ZACHARIAE1,3 , Lise L. GLUUD3,6 and Lone SKOV1,3
, Marianne B. Løvendorf1,2 , Helene M. MARTIN1 , Mila B. JOHANSEN1,3 , Morten B. TRELLE4,5 , Claus ZACHARIAE1,3 , Lise L. GLUUD3,6 and Lone SKOV1,3
1Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte, Hellerup, 2The Leo Foundation Skin Immunology Research Center, Department of Immunology and Microbiology, Faculty of Health and Medical Science, University of Copenhagen, Copenhagen, 3Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, 4Department of Clinical Biochemistry, Odense University Hospital – Svendborg, Svendborg, 5Department of Clinical Research, University of Southern Denmark, Odense, and 6Gastro Unit, Copenhagen University Hospital – Hvidovre, Copenhagen, Denmark
The prevalence of steatotic liver disease (SLD) with fibrosis in patients with psoriasis is unknown and no consensus on screening exists. Therefore, patients from The Copenhagen Translational Skin Immunology Biobank and Research Programme (BIOSKIN) were examined. SLD was defined as controlled attenuation parameter (CAP) > 250 dB/m and fibrosis as median liver stiffness measurement (LSM) ≥ 8 kPa using transient elastography. Biomarkers included fibrosis-4 index (FIB-4), N-terminal propeptide of collagen (type III), and enhanced liver fibrosis (ELF) test. A total of 403 patients (median age 51 years, 54% men, median BMI 27), 80% with moderate-to-severe psoriasis were enrolled. Based on the transient elastography, 40% of the patients had steatosis (mean CAP 245, ± 55 dB/m) and 5% had fibrosis (median LSM 4.8 kPa, IQR 3.8–5.8). According to self-reported alcohol consumption, all patients with steatosis except for 2 were categorized as having metabolic dysfunction-associated steatotic liver disease (MASLD). With transient elastography as the reference, FIB-4 and ELF had better diagnostic accuracy than PIIINP with Area Under the Receiver Operating Characteristic Curve (AUROC) of 0.92 (95% confidence interval 0.87–0.97) for FIB-4, 0.90 (0.83–0.97) for ELF test, and 0.77 (0.66–0.87) for PIIINP.
SIGNIFICANCE
Psoriasis is associated with steatotic liver disease, but it remains unclear whether these patients also have an increased risk of liver fibrosis. Moreover, no consensus exists on optimal screening strategies. In this study of 403 patients with psoriasis, 40% had steatosis and 5% had liver fibrosis. These prevalence estimates fall within the range reported in overweight populations, although direct comparisons are limited by the lack of a control group. The fibrosis-4 index (FIB-4) and enhanced liver fibrosis (ELF) test showed superior diagnostic performance to N-terminal propeptide of collagen type III (PIIINP) and may be preferred for fibrosis screening.
Key words: psoriatic disease; inflammatory skin disease; comorbidities; fatty liver disease; NAFLD; biomarkers.
Citation: Acta Derm Venereol 2026; 106: adv44445. DOI: https://doi.org/10.2340/actadv.v106.44445.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
Submitted: Jul 22, 2025. Accepted after revision: May 5, 2026. Published: Jun 15, 2026.
Corr: Charlotte Näslund-Koch, MD, PhD, Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte, Hellerup, Denmark. E-mail: charlotte.naeslund.koch@regionh.dk
Competing interests and funding: CNK has served as an investigator for Galderma, AbbVie, LEO Pharma, Novartis, and CSL Behring and she has received honoraria as consultant and/or speaker from LEO Pharma and UCB. LG has received research funding from Novo Nordisk, Alexion, Gilead, and Vingmed, and honoraria as consultant/speaker/expert testimony from Novo Nordisk, Boehringer Ingelheim, Astra Zeneca, Pfizer, Sobi International, Becton Dickinson, and Norgine. LS has received research funding from Novartis, Bristol-Myers Squibb, AbbVie, Janssen Pharmaceuticals, the Danish National Psoriasis Foundation, the LEO Foundation, and the Kgl. Hofbundtmager Aage Bang Foundation and honoraria as consultant and/or speaker for AbbVie, Eli Lilly, Novartis, Pfizer, and LEO Pharma, Janssen, UCB, Almirall, Galderma, Bristol-Myers Squibb, and Sanofi. LS has served as an investigator for AbbVie, Pfizer, Sanofi, Janssen, Boehringer Ingelheim, AstraZeneca, Eli Lilly, Novartis, Regeneron, Galderma, and LEO Pharma. The remaining authors report no conflict of interest.
This study was supported by the Ellab Foundation, the LEO Foundation [LF-ST-21-500002], and Copenhagen University Hospital – Herlev and Gentofte Hospital, Denmark. Siemens Healthcare provided the ELF test kits.
INTRODUCTION
Methotrexate (MTX) has been first-line systemic treatment for patients with moderate-to-severe psoriasis for decades. Concerns about hepatotoxicity emerged early, as hepatic fibrosis had been described in patients with leukaemia, treated with high doses of MTX (1). Later studies in psoriasis confirmed the risk of elevated liver enzymes and hepatic fibrosis (2). However, many of these studies were affected by selection bias, as only patients with suspected liver disease underwent liver biopsy, and important confounders were often not considered (3). Subsequent studies have demonstrated that patients with psoriasis exhibit a twofold increased risk of non-alcoholic fatty liver disease (NAFLD)(4), now termed metabolic dysfunction-associated steatotic liver disease (MASLD) (5). Obesity represents the most important risk factor for MASLD and is also a risk factor for incident psoriasis and disease progression (6, 7). The association between psoriasis and MASLD persists after adjustment for obesity and metabolic syndrome, suggesting that systemic inflammation may also contribute (8). While simple steatosis is harmless, 15–25% of the patients will progress to steatohepatitis with varying degree of fibrosis and finally cirrhosis (Fig. S1) (9). MASLD is defined as steatosis in the presence of cardiometabolic risk factors and is part of the broader umbrella term steatotic liver disease (SLD), also including alcohol-related and drug-induced liver injury. The histopathology of MTX-induced steatosis resembles what is seen in the presence of MASLD (10, 11). Thus, the underlying cause of hepatic fibrosis in patients with psoriasis could perhaps be the total burden of risk factors including cardiometabolic factors, alcohol consumption, systemic inflammation, and use of MTX. Currently, no international consensus exists on how to screen patients with psoriasis for hepatic fibrosis (12–15).
In this study, we examined the prevalence of SLD including fibrosis in patients with psoriasis and compared the diagnostic accuracy of the fibrosis-4 index (FIB-4), enhanced liver fibrosis (ELF) test, and N-terminal propeptide of collagen type III (PIIINP) for detecting fibrosis using transient elastography as the reference.
MATERIALS AND METHODS
Study cohort
The Copenhagen Translational Skin Immunology Biobank and Research Programme (BIOSKIN) is an ongoing observational cohort of patients with inflammatory skin diseases at the Department of Dermatology and Allergy, Copenhagen University Hospital – Herlev and Gentofte, Denmark (16). BIOSKIN is conducted according to the Declaration of Helsinki, approved by the Scientific Ethical Committee of the Capital Region, Denmark (H-21032986). All patients gave informed consent prior to inclusion in the study. This study was reported in concordance with STROBE guidelines (17).
We included patients with psoriasis enrolled in BIOSKIN from February 2022 to April 2024. Patients were recruited either from our outpatient clinic or from private dermatological clinics in Copenhagen. Patients (≥ 18 years of age) with psoriasis who could provide informed consent were eligible for inclusion. At enrolment, all participants answered an extensive questionnaire concerning lifestyle factors and health status including educational level, alcohol and tobacco consumption, Dermatology Life Quality Index (DLQI), and presence of psoriatic arthritis and other comorbidities. Information on topical and systemic treatments, including current and previous MTX use, was collected at enrolment through review of medical records supplemented by patient self-report. Data on treatment duration and cumulative MTX dose were not available. A clinical examination was performed by a healthcare professional including anthropometrics and assessment of disease severity using Body Surface Area (BSA) and Psoriasis Area and Severity Index (PASI). Blood samples were collected for biochemical analyses. Liver steatosis and fibrosis were assessed using transient elastography (FibroScan® 530 Compact, Echosens, Paris, France) by a certified and trained clinician.
Blood samples
Metabolic markers included non-fasting haemoglobin A1c (HbA1c), triglycerides, total cholesterol, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol. Liver-specific measurements included platelets, albumin, total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and alkaline phosphatase. FIB-4 was calculated as previously described (Table SI) (18). All analyses were performed using standard hospital assays at the Department of Clinical Biochemistry, Copenhagen University Hospital – Herlev and Gentofte, Denmark. Phosphatidylethanol (PEth) was measured to estimate alcohol intake during the past 2–4 weeks (19). Levels < 0.05 µmol/L indicate low or occasional alcohol consumption and levels > 0.30 µmol/L suggest regular high alcohol intake (20).
Non-invasive tests of hepatic fibrosis
The ELF test was measured using the commercially available test (Atellica IM 1300. Siemens Healthmineers AG, Forchheim, Germany) and included hyaluronic acid (HA), tissue inhibitor of metalloproteinase-1 (TIMP-1), and PIIINP (21). In our analyses, we also included separate values of PIIINP (13). Cut-off values used for the assessment of steatosis and fibrosis are summarized in Table SI (18).
Steatosis was defined by Controlled Attenuation Parameter (CAP) and fibrosis by liver stiffness measurement (LSM) obtained from transient elastography (see Table SI) (22). Patients with signs of fibrosis were referred to the Gastro Unit, Copenhagen University Hospital – Hvidovre, Denmark, for further evaluation.
Covariates
Smoking habits were classified into 3 categories: never, former, and current smokers. Alcohol intake was grouped in categories as follows; ≤ 1 unit/week, 2–7 units/week, 8–15 units/week, 16–21 units/week, or > 21 units/week. Patients were also asked whether a doctor had ever diagnosed them with psoriatic arthritis, hypertension, dyslipidaemia, or diabetes mellitus type 2.
Moderate-to-severe psoriasis was defined as current systemic treatment (conventional or biologics), PASI ≥ 10, DLQI ≥ 10, or BSA ≥ 10.
Statistics
StataNow/SE 18.5 (https://www.stata.com/statanow/) was used to perform the statistical analyses. A two-sided p-value less than 0.05 was considered statistically significant. Parametric and non-parametric tests were applied depending on the distribution of data. Correlations were estimated using scatterplots and by calculating the Pearson correlation coefficient. The Area Under the Receiver Operating Characteristic Curve (AUROC) was calculated and compared for FIB-4, PIIINP, and ELF test with fibrosis on transient elastography as the reference. To visualize overlap between transient elastography (LSM ≥ 8 kPa) and elevated values of FIB-4 (≥ 1.3), ELF test (≥ 9.8) and PIIINP (> 11.0 µg/L for 18–40 years of age and > 9.5 µg/L for 41–70 years of age), a Venn diagram was generated. Potential risk factors for hepatic fibrosis were examined using logistic regression. The dependent variable was fibrosis, defined as LSM ≥ 8 kPa (yes/no). Independent variables included sex (men/women), age (≥ 65/< 65 years), severity of psoriasis (mild/moderate-to-severe), alcohol consumption (≥ 16/< 16 units/week), BMI (≥ 30/< 30 kg/m2), diabetes mellitus type 2 (yes/no), current use of MTX (yes/no), and previous use of MTX (yes/no). Analyses were restricted to univariable models to avoid overfitting. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs), as well as β1 coefficients (log-odds), were reported for each variable.
RESULTS
Clinical and demographic characteristics
Of the 403 patients included in this study, 82 (20%) had mild psoriasis and 321 (80%) had moderate-to-severe psoriasis, defined as current systemic treatment (conventional or biologics), PASI ≥ 10, DLQI ≥ 10, or BSA ≥ 10 (Table I). The mean age was 51 years, with 54% being men. Alcohol consumption was low, with 46% reporting only 0–1 units per week and 36% reporting 2–7 units per week. Overall, we found a moderate correlation between self-reported alcohol consumption and PEth, suggesting underreporting (Pearson correlation coefficient 0.45, p > 0.0001).
| Baseline characteristics | All patients n = 403 |
Patients with mild psoriasis* n = 82 (20%) |
Patients with moderate-severe psoriasis* n = 321 (80%) |
||||||||
| Demographics | |||||||||||
| Age, years, mean (SD) | 51 (± 16) | 51 (± 17) | 51 (± 16) | ||||||||
| Men, n (%) | 217 (54%) | 33 (40%) | 184 (57%) | ||||||||
| Caucasian, n (%) | 375 (93%) | 78 (95%) | 297 (93%) | ||||||||
| Alcohol consumption | |||||||||||
| ≤ 1 unit/week, n (%) | 184 (46) | 27 (33) | 157 (49) | ||||||||
| 2–7 units/week, n (%) | 145 (36) | 34 (41) | 111 (35) | ||||||||
| 8–15 units/week, n (%) | 49 (12) | 15 (18) | 34 (11) | ||||||||
| 16–21 units/week, n (%) | 15 (3.7) | 3 (3.7) | 12 (3.7) | ||||||||
| > 21 units/week, n (%) | 6 (1.5) | 2 (2.4) | 4 (1.3) | ||||||||
| Smoking | |||||||||||
| Never, n (%) | 142 (35) | 33 (40) | 109 (34) | ||||||||
| Former, n (%) | 161 (40) | 34 (41) | 127 (40) | ||||||||
| Current, n (%) | 96 (24) | 14 (17) | 82 (26) | ||||||||
| Higher educational level, n (%) | 160 (40) | 37 (45) | 123 (38) | ||||||||
| Comorbidities | |||||||||||
| Hypertension, n (%) | 122 (30) | 21 (26) | 101 (31) | ||||||||
| Dyslipidaemia, n (%) | 111 (28) | 17 (21) | 94 (29) | ||||||||
| Diabetes mellitus type 2, n (%) | 24 (6.0) | 3 (3.7) | 21 (6.5) | ||||||||
| Anthropometrics | |||||||||||
| Systolic blood pressure, mmHg, mean (SD) | 140 (± 19) | 138 (± 17) | 140 (± 20) | ||||||||
| Diastolic blood pressure, mmHg, mean (SD) | 87 (± 12) | 87 (± 11) | 87 (± 12) | ||||||||
| BMI, kg/m2, median (IQR) | 27 (24–31) | 25 (23–28) | 28 (24–32) | ||||||||
| Waist circumference, cm, median (min–max) | 97 (± 16) | 92 (± 14) | 98 (± 16) | ||||||||
| Waist–hip ratio, median (min–max) | 0.90 (0.10) | 0.87 (0.09) | 0.91 (0.10) | ||||||||
| Disease characteristics | |||||||||||
| PASI, median (min–max) | 2.4 (0.0–40.8) | 2.8 (0.0–9.6) | 2.4 (0.0–40.8) | ||||||||
| BSA, median (min–max) | 2.0 (0.0–80.0) | 2.0 (0.0–9.0) | 1.5 (0.0–80) | ||||||||
| DLQI, median (min–max) | 2.0 (0.0–26.0) | 3.0 (0.0–19.0) | 1.5 (0.0–26.0) | ||||||||
| Psoriatic arthritis, n (%) | 95 (24) | 12 (15) | 83 (26) | ||||||||
| Current systemic treatment, n (%) | 309 (77) | 0 (0) | 309 (96) | ||||||||
| Current treatment with MTX, n (%) | 143 (35) | 0 (0) | 143 (45) | ||||||||
| Previous treatment with MTX, n (%) | 137 (34) | 14 (17) | 123 (38) | ||||||||
| Metabolic blood profile | |||||||||||
| HbA1c, mmol/mol, median (min–max) | 33 (24 – 116) | 33 (26–58) | 34 (24–116) | ||||||||
| Triglycerides, mmol/L, median (min–max) | 1.3 (0.4–13.2) | 1.3 (0.4–4.0) | 1.4 (0.4–13.2) | ||||||||
| Total cholesterol, mmol/L, mean (SD) | 4.8 (± 0.96) | 5.1 (± 0.90) | 4.8 (± 0.97) | ||||||||
| LDL cholesterol, mmol/L, mean (SD) | 2.7 (± 0.86) | 2.9 (± 0.81) | 2.7 (± 0.86) | ||||||||
| HDL cholesterol, mmol/L, mean (SD) | 1.4 (± 0.40) | 1.5 (± 0.37) | 1.4 (± 0.40) | ||||||||
| n: number; SD: standard deviation; BMI: body mass index; IQR: interquartile range; min: minimum; max: maximum; HbA1c: haemoglobin A1c; LDL: low-density lipoprotein; HDL; high-density lipoprotein. *Moderate-severe psoriasis was defined as current systemic treatment (conventional or biologics): PASI≥ 10: DLQI≥ 10: or BSA≥ 10. |
|||||||||||
Compared with patients with mild psoriasis, a higher proportion of patients with moderate-to-severe disease reported having hypertension (43% vs 28%), dyslipidaemia (41% vs 26%), and type 2 diabetes (10% vs 5%). Six patients were reported to have known liver disease at baseline including MASLD, primary sclerosing cholangitis, and Gilbert syndrome (Table SII). The median PASI was 2.4 (min.–max. 0.0–40.8) with slightly lower values observed in patients categorized as having moderate-to-severe psoriasis, indicating effective anti-psoriatic treatments in this group. A similar phenomenon was observed regarding BSA and DLQI. Missing values are presented in Table SIII.
Liver measurements
Liver tests including AST, ALT, albumin, platelets, total bilirubin, and alkaline phosphatase were within normal range for most patients (Table II). Based on transient elastography, 40% had liver steatosis (mean CAP 245, ± 55 dB/m) and 5% had fibrosis (median LSM 4.8 kPa, IQR 3.8–5.8). According to the self-reported alcohol consumption, all patients were categorized as MASLD, except for 3 patients who had ALD. Baseline characteristics and values of FIB-4, ELF test, and PIIINP on all 21 patients with fibrosis are presented in Table SIV.
The estimated proportion of individuals with fibrosis was 24% based on FIB-4 (median 0.90, IQR 0.63–1.28), 20% based on ELF test (median 9.0, IQR 8.3–9.6), and 14% based on PIIINP (median 6.9 µg/L, IQR 5.7–8.4) (Table II). As illustrated in the Venn diagram (Fig. S2), 8 patients showed evidence of fibrosis based on all 4 measurements, 31 on 3 measurements, and 69 patients on 2 measurements. Seven patients with suspected fibrosis underwent a liver biopsy showing MASH with fibrosis or MetALD with fibrosis (see Table SIII). The remaining patients were not biopsied due to lack of consent, medical contraindications, or because repeated non-invasive assessments did not support clinically significant fibrosis.
Pearson correlation coefficient between levels of fibrosis using LSM and blood tests was highest for FIB-4 with r = 0.57 (p < 0.0001), followed by the ELF test (r = 0.41, p < 0.0001), and PIIINP (r = 0.30, p < 0.0001) (Fig. S3).
In the univariable logistic regression analyses, higher age (OR 2.97, 95% CI 1.21–7.30), excessive alcohol consumption (OR 7.07, 95% CI 2.30–21.71), type 2 diabetes (OR 6.09, 95% CI 2.28–16.27), and previous MTX use (OR 2.74, 95% CI 1.13–6.68) were associated with liver fibrosis, whereas psoriasis severity, BMI, and current MTX use were not (Table III).
Diagnostic accuracy
The sensitivity for detecting fibrosis was highest for FIB-4 (0.86), followed by ELF test (0.76) and PIIINP (0.43) (Fig. 1A). Specificity was highest for PIIINP (0.88) followed by ELF and FIB-4 (0.83 and 0.79, respectively). FIB-4 and ELF test demonstrated superior diagnostic accuracy for identifying liver fibrosis than PIIINP with AUROC of 0.92 (0.87–0.97) for FIB-4, 0.90 (0.83–0.97) for ELF test, and 0.77 (0.66–0.87) for PIIINP (Fig. 1B). Pairwise comparisons confirmed that FIB-4 and ELF test outperformed PIIINP (p = 0.01) but were not significantly different from each other (p = 0.52). These findings remained consistent across subgroups stratified by age, alcohol intake, BMI, and sex (Fig. S4).
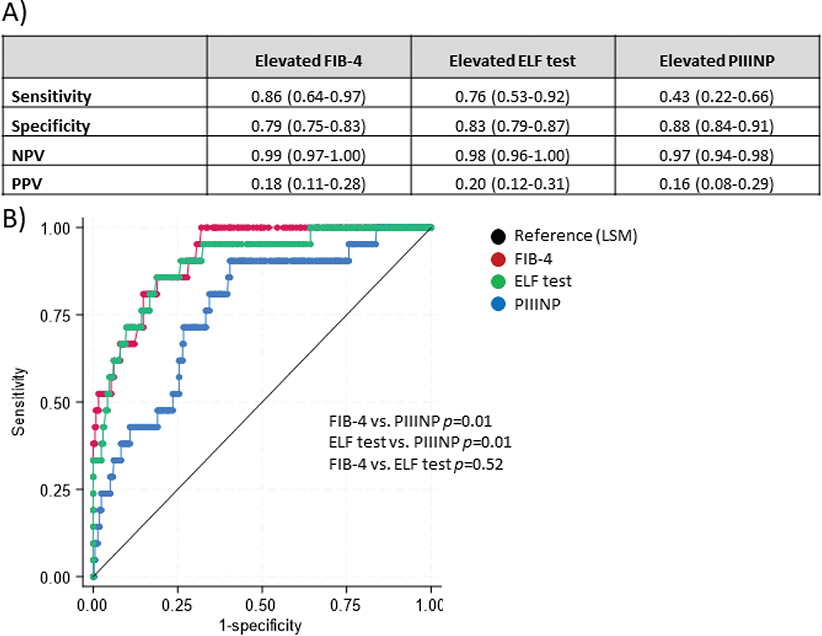
Fig. 1. Diagnostic accuracy of fibrosis-4 index (FIB-4), enhanced liver fibrosis (ELF) test, and procollagen 3 N-terminal peptide (PIIINP) for diagnosing hepatic fibrosis (reference = liver stiffness measurement [LSM] ≥ 8 kPa). (A) Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) of elevated FIB-4, ELF test, and PIIINP with transient elastography (LSM ≥ 8 kPa) as the reference. (B) Area Under the Receiver Operating Characteristic Curve (AUROC) for FIB-4, ELF test, and PIIINP. Fibrosis according to transient elastography (LSM ≥ 8 kPa) as the reference.
In a sensitivity analysis applying age-adjusted FIB-4 thresholds (≥ 1.3 for < 65 years and ≥ 2.0 for ≥ 65 years), sensitivity decreased slightly (0.81 vs 0.86), while specificity improved (0.86 vs 0.79). The negative predictive value remained high (0.99), and the positive predictive value increased modestly (0.24 vs 0.18), indicating preserved rule-out performance.
DISCUSSION
In this clinical study of 403 patients with psoriasis, 5% showed evidence of hepatic fibrosis according to transient elastography. The blood-based biomarkers FIB-4 and ELF test had better diagnostic accuracy than PIIINP for identifying this. These findings support previous studies suggesting that the risk of MTX-related liver fibrosis may be overestimated, and may help inform the choice of screening tools in the absence of consensus on screening for hepatic fibrosis in psoriasis.
The global prevalence of MASLD is ≈25% but in overweight populations this ranges from 33–53% (23). In this context, the observed steatosis prevalence of 40% in our cohort falls within the range reported in overweight populations. However, as this study did not include a control group and comparable Danish population-based data are lacking, these comparisons should be interpreted cautiously. Similarly, the prevalence of hepatic fibrosis in the general population is ≈5% and even higher in at-risk groups (24). In our univariable analyses, psoriasis severity and current MTX use were not associated with fibrosis. Previous MTX use, however, showed an association with fibrosis. This should be interpreted cautiously as this may reflect discontinuation of MTX in patients with early liver abnormalities and a potential survivor effect, whereby patients tolerating MTX remain on treatment while those developing abnormalities discontinue.
Taken together, our findings do not suggest a markedly increased prevalence of steatosis or fibrosis due to psoriasis itself or to ongoing use of MTX; however, controlled studies using matched populations are needed to address this question more definitively.
The prevalence of steatosis and fibrosis was higher in patients with moderate-to-severe psoriasis compared with patients with mild disease (steatosis 45% vs 24%; fibrosis 5.9% vs 2.4%), which may be due to a higher prevalence of obesity and type 2 diabetes. In further support of our findings, a meta-analysis of randomized controlled trials (n = 13,177 participants) of MTX users including patients with rheumatoid arthritis, psoriasis, psoriatic arthritis, and inflammatory bowel disease, MTX was associated with increased risk of liver enzyme abnormalities but not fibrosis, cirrhosis, liver failure, or death (25). In addition, Atallah et al. examined ≈ 1,000 patients with psoriasis and rheumatoid arthritis using transient elastography, ELF test, and PIIINP and concluded that neither MTX cumulative dose nor duration was associated with liver fibrosis (26). However, in contrast to our findings, a systematic review found 22% increased risk of “any fibrosis” following use of MTX (3). Importantly, they did not find an increased risk of “significant fibrosis”, which is the clinically relevant outcome. Furthermore, they included only studies with biopsy-diagnosed fibrosis, which induce a high degree of selection bias. Lastly, they did not find any clear association between cumulative dose of MTX and fibrosis, which one would expect if MTX was the underlying cause of the fibrosis. Thus, the findings of our study suggest that metabolic risk factors may be more important than the use of MTX in the development of hepatic fibrosis, although a potential contribution of MTX cannot be excluded. Consequently, screening patients with psoriasis and cardiometabolic risk factors for hepatic fibrosis, especially before starting hepatotoxic drugs, may be more beneficial than focusing solely on patients on MTX treatment.
Immune-mediated mechanisms involving tumour necrosis factor (TNF) and interleukin (IL)-17 are increasingly recognized in the pathogenesis of steatohepatitis and liver fibrosis (27). As inhibitors of these pathways are widely used in psoriasis, use of biologics could plausibly modulate hepatic inflammation and fibrogenesis (28). Although speculative, such treatment-related effects may partly contribute to the absence of a clear association between psoriasis severity and liver fibrosis observed in our cohort.
PIIINP has been used to monitor hepatic fibrosis since the 1980s (29). It reflects type III collagen formation (= active fibrogenesis) but does not capture established fibrosis. Furthermore, PIIINP is not liver-specific and may be elevated in several other conditions, including psoriatic arthritis, post-surgery, smoking, and normal growth in children (13, 29–31). In this study, PIIINP had lower diagnostic accuracy than FIB-4 and the ELF test. However, it should be noted that British and European guidelines suggest serial measurements of PIIINP, which might increase diagnostic accuracy (12, 13, 15). The ELF test is a newer commercially available blood-based biomarker which combines PIIINP with 2 other serological markers including HA and TIMP-1. The ELF test is a reliable diagnostic tool in both healthy individuals and patients with alcoholic-related liver disease, MASLD, and chronic hepatitis (32). However, its application in patients with psoriasis remains understudied (33). FIB-4 is a simple and cheap blood-based algorithm, based on ALT, AST, platelets, and age, and is widely used as a first-line screening tool for hepatic fibrosis (18). A limitation is reduced specificity in older individuals (≥ 65 years) (34). However, in our sensitivity analyses using age-adjusted FIB-4 thresholds, the negative predictive value remained high, supporting the robustness of FIB-4 as a rule-out tool. In our study, FIB-4 and ELF showed better diagnostic accuracy than PIIINP in detecting hepatic fibrosis. In support of these findings, a small retrospective cohort study (n = 27) found that a single measurement of ELF test had higher diagnostic accuracy than serial PIIINP (35). The diagnostic accuracy of FIB-4 and ELF test was similar in our study; however, in another cohort study of the Danish general population (n = 155), the ELF test diagnosed fibrosis on liver biopsies significantly better than FIB-4 (36). In our study, the diagnostic accuracy of FIB-4, the ELF test, and PIIINP are calculated based on cut-off values for determining MASLD in the general population. One could speculate as to whether patients with psoriasis should have other cut-off values to allow for a mild and transient liver affection. However, van der Voort et al. (33) explored distribution and cut-off for the ELF test in patients with psoriasis, psoriatic arthritis, and rheumatoid arthritis and recommend existing cut-offs for healthy individuals. Similarly, in our data, we find that FIB-4 < 1.3 is the best cut-off value for patients with psoriasis in order to rule out fibrosis (data not shown).
Importantly, even though established non-invasive tools performed well in this study, they are limited by false-positive results. Emerging biomarker approaches, including OMIC-based markers, may offer improved specificity for MASLD activity and fibrosis and represent an important area for future research in patients with psoriasis.
Limitations
Some limitations need to be considered. We used transient elastography as reference when identifying hepatic fibrosis, and, even though this method is well validated, with high diagnostic and prognostic accuracy (18), it is not per se the truth. The gold standard for diagnosing hepatic fibrosis includes a liver biopsy but due to the invasiveness of this procedure, this cannot be used as a screening tool. Recently, another definition of fibrosis including FIB-4 ≥ 1.3 and LSM ≥ 8 has been suggested as a more reliable definition than only LSM. If we use this definition instead, we find a similar prevalence of fibrosis (4.5% vs 5.2%), confirming the validity of our findings. Another limitation with our study is the lack of data on cumulative dose and duration of MTX, which limits the ability to assess potential dose–response relationships with hepatic fibrosis. Furthermore, in Denmark, MTX treatment is accompanied by structured laboratory monitoring, which may introduce surveillance bias, as patients with early biochemical abnormalities may discontinue treatment, potentially attenuating the observed fibrosis risk. Lastly, patients living in the surroundings of our hospital are in general healthy with high socioeconomic status and a rather low burden of unfavourable lifestyle factors. Therefore, our results may not be generalizable to all patients with psoriasis.
Conclusion
In our study of 403 patients with psoriasis, 40% showed evidence of liver steatosis and 5% of fibrosis. The observed prevalence of steatosis and fibrosis falls within the range reported in other overweight populations, although direct comparisons are limited by the lack of a control group. Overall, our findings suggest that cardiometabolic risk factors may play a more prominent role in hepatic fibrosis than MTX use alone, although a potential contribution of MTX cannot be excluded. FIB-4 and the ELF test showed superior diagnostic accuracy to PIIINP and would be preferred as screening tools. Clinically, our findings support a risk-based approach, prioritizing patients with cardiometabolic risk factors rather than focusing solely on MTX. FIB-4 may serve as an initial rule-out tool, with transient elastography and/or ELF testing reserved for patients with elevated scores.
ACKNOWLEDGEMENTS
The authors are grateful for the important contributions of the staff and participants of BIOSKIN.
Data availability
The dataset presented in this article is not available because data from the BIOSKIN cohort are subject to protection from the national Danish Data Protection Agency. However, interested researchers can contact the corresponding author to request data access.
Ethics statement
This study was reviewed and approved by the National Committee on Health Research Ethics (H-21032986). The patients provided their written informed consent prior to inclusion in the study.
REFERENCES
- Hutter RVP, Shipkey FH, Tan CTC, Murphy ML, Chowdhury M. Hepatic fibrosis in children with acute leukemia: a complication of therapy. Cancer 1960; 13: 288–307. https://doi.org/10.1002/1097-0142(196003/04)13:2<288::AID-CNCR2820130213>3.0.CO;2-L
- Dahl MGC, Gregory MM, Scheuer PJ. Liver damage due to methotrexate in patients with psoriasis. Br Med J 1971; 1: 625–630. https://doi.org/10.1136/bmj.1.5750.625
- Maybury CM, Jabbar-Lopez ZK, Wong T, Dhillon AP, Barker JN, Smith CH. Methotrexate and liver fibrosis in people with psoriasis: a systematic review of observational studies. Br J Dermatol 2014; 171: 17–29. https://doi.org/10.1111/bjd.12941
- Bellinato F, Gisondi P, Mantovani A, Girolomoni G, Targher G. Risk of non-alcoholic fatty liver disease in patients with chronic plaque psoriasis: an updated systematic review and meta-analysis of observational studies. J Endocrinol Invest 2022; 45: 1277–1288. https://doi.org/10.1007/s40618-022-01755-0
- Rinella ME, Lazarus JV., Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol 2023; 79: 1542–1556. https://doi.org/10.1016/j.jhep.2023.06.003
- Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes 2012; 2: e54. https://doi.org/10.1038/nutd.2012.26
- Budu-Aggrey A, Brumpton B, Tyrrell J, Watkins S, Modalsli EH, Celis-Morales C, et al. Evidence of a causal relationship between body mass index and psoriasis: a Mendelian randomization study. PLoS Med 2019; 16: e1002739. https://doi.org/10.1371/journal.pmed.1002739
- Mantovani A, Gisondi P, Lonardo A, Targher G. Relationship between non-alcoholic fatty liver disease and psoriasis: a novel hepato-dermal axis? Int J Mol Sci 2016; 17: 217. https://doi.org/10.3390/ijms17020217
- Spengler EK, Loomba R. Recommendations for diagnosis, referral for liver biopsy, and treatment of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Mayo Clin Proc 2015; 90: 1233–1246. https://doi.org/10.1016/j.mayocp.2015.06.013
- Gelfand JM, Wan J, Zhang H, Shin DB, Ogdie A, Syed MN, et al. Risk of liver disease in patients with psoriasis, psoriatic arthritis, and rheumatoid arthritis receiving methotrexate: a population-based study. J Am Acad Dermatol 2021; 84: 1636–1643. https://doi.org/10.1016/j.jaad.2021.02.019
- Raahimi MM, Livesey A, Hamilton J, Shipman AR, Aspinall RJ. Liver fibrosis for the dermatologist: a review. Clin Exp Dermatol 2023; 48: 303–309. https://doi.org/10.1093/ced/llac083
- Warren RB, Weatherhead SC, Smith CH, Exton LS, Mohd Mustapa MF, Kirby B, et al. British Association of Dermatologists’ guidelines for the safe and effective prescribing of methotrexate for skin disease 2016. Br J Dermatol 2016; 175: 23–44. https://doi.org/10.1111/bjd.14816
- Raaby L, Zachariae C, Østensen M, Heickendorff L, Thielsen P, Grønbæk H, et al. Methotrexate use and monitoring in patients with psoriasis: a consensus report based on a Danish expert meeting. Acta Derm Venereol 2017; 97: 426–432. https://doi.org/10.2340/00015555-2599
- Menter A, Gelfand JM, Connor C, Armstrong AW, Cordoro KM, Davis DMR, et al. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J Am Acad Dermatol 2020; 82: 1445–1486. https://doi.org/10.1016/j.jaad.2020.02.044
- Nast A, Smith C, Spuls PI, Avila Valle G, Bata-Csörgö Z, Boonen H, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris – Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol 2020; 34: 2461–2498. https://doi.org/10.1111/jdv.16915
- Løvendorf MB, Johansen JD, Skov L. BIOSKIN: a protocol for the Copenhagen Translational Skin Immunology Biobank and Research Programme. BMJ Open 2024; 14: e077207. https://doi.org/10.1136/bmjopen-2023-077207
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370: 1453–1457. https://doi.org/10.1016/S0140-6736(07)61602-X
- Berzigotti A, Tsochatzis E, Boursier J, Castera L, Cazzagon N, Friedrich-Rust M, et al. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis – 2021 update. J Hepatol 2021; 75: 659–689. https://doi.org/10.1016/j.jhep.2021.05.025
- Perilli M, Toselli F, Franceschetto L, Cinquetti A, Ceretta A, Cecchetto G, et al. Phosphatidylethanol (PEth) in blood as a marker of unhealthy alcohol use: a systematic review with novel molecular insights. Int J Mol Sci 2023; 24: 12175. https://doi.org/10.3390/ijms241512175
- Helander A, Hansson T. The alcohol biomarker phosphatidylethanol (PEth)-test performance and experiences from routine analysis and external quality assessment. Scand J Clin Lab Invest 2023; 83: 424–431. https://doi.org/10.1080/00365513.2023.2253734
- Vali Y, Lee J, Boursier J, Spijker R, Löffler J, Verheij J, et al. Enhanced liver fibrosis test for the non-invasive diagnosis of fibrosis in patients with NAFLD: a systematic review and meta-analysis. J Hepatol 2020; 73: 252–262. https://doi.org/10.1016/j.jhep.2020.03.036
- Xu X, Jin J, Liu Y. Performance of FibroScan in grading steatosis and fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Arab J Gastroenterol 2023; 24: 189–197. https://doi.org/10.1016/j.ajg.2023.08.003
- Quek J, Chan KE, Wong ZY, Tan C, Tan B, Lim WH, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2023; 8: 20–30. https://doi.org/10.1016/S2468-1253(22)00317-X
- Ginès P, Castera L, Lammert F, Graupera I, Serra-Burriel M, Allen AM, et al. Population screening for liver fibrosis: toward early diagnosis and intervention for chronic liver diseases. Hepatology 2022; 75: 219–228. https://doi.org/10.1002/hep.32163
- Conway R, Low C, Coughlan RJ, O’Donnell MJ, Carey JJ. Risk of liver injury among methotrexate users: a meta-analysis of randomised controlled trials. Semin Arthritis Rheum 2015; 45: 156–162. https://doi.org/10.1016/j.semarthrit.2015.05.003
- Atallah E, Grove JI, Crooks C, Burden-Teh E, Abhishek A, Moreea S, et al. Risk of liver fibrosis associated with long-term methotrexate therapy may be overestimated. J Hepatol 2023; 78: 989–997. https://doi.org/10.1016/j.jhep.2022.12.034
- Huby T, Gautier EL. Immune cell-mediated features of non-alcoholic steatohepatitis. Nat Rev Immunol 2022; 22: 429–443. https://doi.org/10.1038/s41577-021-00639-3
- González Fernández J, Prieto-Torres L, Ara Martín M, Martínez-Domínguez SJ. MASLD and liver fibrosis in patients with psoriasis receiving IL-17 or IL-23 inhibitors: a systematic review. Therap Adv Gastroenterol 2025; 18. https://doi.org/10.1177/17562848251335824
- Maybury CM, Samarasekera E, Douiri A, Barker JN, Smith CH. Diagnostic accuracy of noninvasive markers of liver fibrosis in patients with psoriasis taking methotrexate: a systematic review and meta-analysis. Br J Dermatol 2014; 170: 1237–1247. https://doi.org/10.1111/bjd.12905
- Zachariae H, Muhammad Aslam H, Bjerring P, Søgaard H, Zachariae E, Heickendorff L. Serum aminoterminal propeptide of type III procollagen in psoriasis and psoriatic arthritis: relation to liver fibrosis and arthritis. J Am Acad Dermatol 1991; 25: 50–53. https://doi.org/10.1016/0190-9622(91)70173-Y
- Crofton PM, Wade JC, Taylor MRH, Holland CV. Serum concentrations of carboxyl-terminal propeptide of type I procollagen, amino-terminal propeptide of type III procollagen, cross-linked carboxyl-terminal telopeptide of type I collagen, and their interrelationships in schoolchildren. Clin Chem 1997; 43: 1577–1581. https://doi.org/10.1093/clinchem/43.9.1577
- Sharma C, Cococcia S, Ellis N, Parkes J, Rosenberg W. Systematic review: accuracy of the enhanced liver fibrosis test for diagnosing advanced liver fibrosis and cirrhosis. J Gastroenterol Hepatol 2021; 36: 1788–1802. https://doi.org/10.1111/jgh.15482
- van der Voort EAM, Wakkee M, Veldt-Kok P, Darwish Murad S, Nijsten T. Enhanced liver fibrosis test in patients with psoriasis, psoriatic arthritis and rheumatoid arthritis: a cross-sectional comparison with procollagen-3 N-terminal peptide (P3NP). Br J Dermatol 2017; 176: 1599–1606. https://doi.org/10.1111/bjd.15220
- McPherson S, Hardy T, Dufour JF, Petta S, Romero-Gomez M, Allison M, et al. Age as a confounding factor for the accurate non-invasive diagnosis of advanced NAFLD fibrosis. Am J Gastroenterol 2017; 112: 740–751. https://doi.org/10.1038/ajg.2016.453
- Martyn-Simmons CL, Rosenberg WMC, Cross R, Wong T, Smith CH, Barker JNWN. Validity of noninvasive markers of methotrexate-induced hepatotoxicity: a retrospective cohort study. Br J Dermatol 2014; 171: 267–273. https://doi.org/10.1111/bjd.12782
- Kjaergaard M, Lindvig KP, Thorhauge KH, Andersen P, Hansen JK, Kastrup N, et al. Using the ELF test, FIB-4 and NAFLD fibrosis score to screen the population for liver disease. J Hepatol 2023; 79: 277–286. https://doi.org/10.1016/j.jhep.2023.04.002