SHORT COMMUNICATION
X-linked Recessive Ectodysplasin A Mutations Induced Hypohidrotic Ectodermal Dysplasia and Severe Atopic Dermatitis Successfully Treated with Dupilumab
Lu LU1–3  , Jindi FENG1–3 , Huimin HE1–3 , Yubin PENG1–3 , Shiyu ZHANG1–3 , Lu YANG1–3 , Yuehua LIU1–3 and Tao WANG1–3*
, Jindi FENG1–3 , Huimin HE1–3 , Yubin PENG1–3 , Shiyu ZHANG1–3 , Lu YANG1–3 , Yuehua LIU1–3 and Tao WANG1–3*
1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 2State Key Laboratory of Complex Severe and Rare Diseases, Beijing, and 3National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, China. *E-mail: wangtaopumch@126.com
Citation: Acta Derm Venereol 2026; 106: adv44646. DOI: https://doi.org/10.2340/actadv.v106.44646.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 18, 2025. Accepted after revision: Dec 11, 2025. Published: Jan 9, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
Ectodermal dysplasia (ED) is a group of congenital disorders from ectodermal tissue development abnormalities. Its hallmark is the abnormal development of skin appendages or oral mucosa during embryogenesis (1). Based on phenotypic, genotypic, and molecular pathway variations, ED has several subtypes (2), with hypohidrotic ectodermal dysplasia (HED) (OMIM 305100) being the most common. HED, an X-linked recessive disorder due to ectodysplasin A (EDA) gene mutations, is marked by sparse hair, missing teeth, and reduced sweating (1). Treatment mainly manages symptoms and prevents any issues. Skin care emphasizes maintaining hydration with emollients and avoiding high-temperature environments, especially during summer. Currently, no effective systemic treatment options are well established, thus, skin symptom management is especially important to maintain patients’ quality of life. This case report is the first to describe a child with HED and atopic dermatitis (AD) who exhibited significant improvement in skin symptoms following regular treatment with dupilumab during summer.
CASE REPORT
A 10-year-old child presented with recurrent erythema, papules, and dryness on the face, trunk, and limbs since early childhood, accompanied by pruritus. There was no previous history of atopic dermatitis. Heat exposure led to overheating, increased heart rate, and rapid breathing. The child also had dental and hair abnormalities. At 10 years old, the skin condition worsened with severe itching and ulceration on the arms. Physical examination showed a saddle nose, sparse scalp hair, no axillary hair, 3 conical teeth, and dry skin with multiple erythematous patches and papules on the face, neck, back, arms, and legs (Fig. 1). The EASI score was 19.2.

Fig. 1. Lesions before and after dupilumab treatment. (A–D) Multiple erythematous patches and papules over the face, back, and limbs before treatment. (E–H) 4 weeks after initiation of dupilumab treatment, skin lesions were improved.
Laboratory tests revealed elevated eosinophil counts (WBC 6.89×109/L, EOS% 7.7%, EOS# 0.53×109/L) and elevated total immunoglobulin E (T-IgE 1182.0 KU/L). The patient showed allergies to multiple allergens, including willow, hops, and cat dander. Whole-exome sequencing identified a hemizygous mutation in the EDA gene (c.602G>T (p.Gly201Val)). According to the ACMG guidelines, this mutation meets PM2+PM5+PP3+PP4 criteria and is considered likely pathogenic (3). The patient was diagnosed with HED and met the diagnostic criteria for AD.
Prior to admission, the patient had not received systematic treatment. After obtaining informed consent, the patient was started on dupilumab therapy (an initial dose of 600 mg subcutaneously, followed by 300 mg subcutaneously every 2 weeks). In addition, the patient received boric acid solution for the eroded areas, as well as topical corticosteroids and tacrolimus for erythema and papules. After 3 treatments, the patient experienced significant relief from pruritus, with marked resolution of erythema and papules. Total IgE levels decreased to 721 KU/L. The EASI score dropped to 6.4 (Fig. 2). The patient is currently under regular follow-up in our outpatient clinic, with stable control of the rash and a less restrictive school life in the summer.
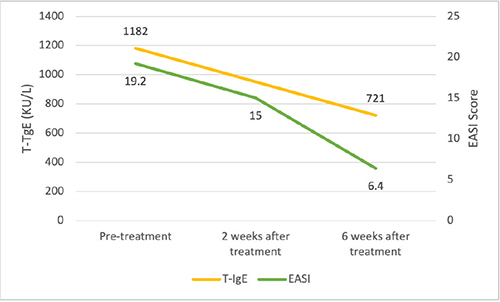
Fig. 2. EASI score and T-IgE before and after treatment.
DISCUSSION
Dupilumab is a fully human monoclonal antibody targeting the interleukin-4 receptor alpha subunit (IL-4Rα), effectively inhibiting the IL-4/IL-13 signalling pathway and consequently blocking the downstream overexpression of IgE. It has been widely used for the treatment of atopic dermatitis, asthma, and chronic rhinosinusitis with nasal polyposis (4–6). An increasing number of reports have documented the off-label use of dupilumab in other genetic skin disorders, such as Hailey–Hailey disease and Netherton syndrome (7, 8).
Patients with HED suffered a high prevalence of allergic diseases (9). This may be related to the skin barrier dysfunction caused by HED, which predisposes individuals to atopic diathesis (10). Further studies on ceramide profiles have revealed that the ceramide spectrum in HED patients resembles that of AD patients, although HED patients exhibit significantly higher levels of ceramide 1 (11). This similarity may help explain the frequent comorbidity of these conditions.
In utero EDA replacement therapy may be an effective prenatal treatment (12–15). Treatment for the skin manifestations of HED primarily focuses on prevention, with limited reports of effective systemic therapies. Janus kinase (JAK) inhibitors, such as tofacitinib, have been reported in cases of HED associated with atopic dermatitis (16). Topical minoxidil is therapeutically effective for HED-related hair loss (17). Our case report is the first to describe the successful use of dupilumab in a patient with HED and AD, demonstrating its efficacy and providing a novel therapeutic option for managing HED during summer time. The mechanistic rationale may involve the following: the EDA gene orchestrates ectodermal organogenesis via downstream NF-κB and Wnt signalling pathways (18). Functionally, EDA contributes to epidermal morphogenesis, placode patterning, and keratin expression profiles (19), and in vitro evidence confirms its role in upregulating sweat gland-specific cytokeratins (CK5, CK10, CK14, CK18, CK19) (20). Notably, mutations in cytokeratin genes underlie other ectodermal dysplasias (e.g., ectodermal dysplasia 4, monilethrix) (2), reinforcing the centrality of structural proteins in these disorders. At the tissue level, desmosome – governed by desmocollin (Dsc) and desmoglein (Dsg) as core transmembrane adhesion molecules – is critical for epithelial cohesion. Murine models demonstrate EDA/NF-κB-mediated transcriptional activation of Dsc (21), suggesting that HED-associated EDA mutations may precipitate keratin–desmosome network dysfunction, thereby compromising cutaneous barrier homeostasis. Significantly, IL-4/IL-13 signalling suppresses the expression of key structural components (keratins, desmocollins, desmogleins) (22), implying that targeted IL-4/IL-13 blockade could counteract the molecular sequelae of EDA deficiency and ameliorate HED pathology. Future studies are needed to delineate the specific mechanisms by which dupilumab exerts its beneficial effects in HED.
ACKNOWLEDGEMENTS
This work was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-B-092, to Tao Wang), Beijing Municipal Natural Science Foundation (Z210017, to Tao Wang), Beijing Key Clinical Specialty Construction Project, and National Key Clinical Specialty Project of China.
Ethical approval: Written informed consent for publication was obtained from the patient’s guardian.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Reyes-Reali J, Mendoza-Ramos MI, Garrido-Guerrero E, Méndez-Catalá CF, Méndez-Cruz AR, Pozo-Molina G. Hypohidrotic ectodermal dysplasia: clinical and molecular review. Int J Dermatol 2018; 57: 965–972. https://doi.org/10.1111/ijd.14048
- Timothy W, Fete M, Schneider H, Zinser M, Koster MI, Clarke AJ, et al. Ectodermal dysplasias: classification and organization by phenotype, genotype and molecular pathway. Am J Med Genet A 2019; 179: 442–447. https://doi.org/10.1002/ajmg.a.61045
- Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 2015; 17: 405–424. https://doi.org/10.1038/gim.2015.30
- Guttman-Yassky E, Bissonnette R, Ungar B, Suárez-Fariñas M, Ardeleanu M, Esaki H, et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J Allergy Clin Immunol 2019; 143: 155–172. https://doi.org/10.1016/j.jaci.2018.08.022
- Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med 2018; 378: 2486–2496. https://doi.org/10.1056/NEJMoa1804092
- Bachert C, Han JK, Desrosiers M, Hellings PW, Amin N, Lee SE, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019; 394: 1638–1650. https://doi.org/10.1016/S0140-6736(19)31881-1
- Debeuf M-EPH, Vlaanderen P, van Geel M, Steijlen PM, Verstraeten VLRM. Dupilumab for Hailey–Hailey disease. J Dermatolog Treat 2025; 36: 2557477. https://doi.org/10.1080/09546634.2025.2557477
- Nakayama S, Yonekura S, Murase K, Nakagawa I, Izawa K, Nakajima S, et al. Dupilumab improves skin microbiome in a paediatric case of Netherton syndrome. J Eur Acad Dermatol Venereol 2025; 39: e1060–e1062. https://doi.org/10.1111/jdv.70006
- Inazawa-Terada M, Namiki T, Omigawa C, Fujimoto T, Munetsugu T, Ugajin T, et al. An epidemiological survey of anhidrotic/hypohidrotic ectodermal dysplasia in Japan: high prevalence of allergic diseases. J Dermatol 2022; 49: 422–431. https://doi.org/10.1111/1346-8138.16278
- Koguchi-Yoshioka H, Wataya-Kaneda M, Yutani M, Murota H, Nakano H, Sawamura D, et al. Atopic diathesis in hypohidrotic/anhidrotic ectodermal dysplasia. Acta Derm Venereol 2015; 95: 476–479. https://doi.org/10.2340/00015555-1978
- Jungersted JM, Høgh JK, Hellgren LI, Agner T, Jemec GBE. Ceramide profile in hypohidrotic ectodermal dysplasia. Clin Exp Dermatol 2012; 37: 153–155. https://doi.org/10.1111/j.1365-2230.2011.04200.x
- Schneider H, Schweikl C, Faschingbauer F, Hadj-Rabia S, Schneider P. A causal treatment for x-linked hypohidrotic ectodermal dysplasia: long-term results of short-term perinatal ectodysplasin A1 replacement. Int J Mol Sci 2023; 24: 7155. https://doi.org/10.3390/ijms24087155
- Schneider H, Hadj-Rabia S, Faschingbauer F, Bodemer C, Grange DK, Norton ME, et al. Protocol for the phase 2 EDELIFE Trial investigating the efficacy and safety of intra-amniotic ER004 administration to male subjects with X-linked hypohidrotic ectodermal dysplasia. Genes (Basel) 2023; 14: 153. https://doi.org/10.3390/genes14010153
- Schneider H, Faschingbauer F, Schuepbach-Mallepell S, Körber I, Wohlfart S, Dick A, et al. Prenatal correction of X-linked hypohidrotic ectodermal dysplasia. N Engl J Med 2018; 378: 1604–1610. https://doi.org/10.1056/NEJMoa1714322
- Gaide O, Schneider P. Permanent correction of an inherited ectodermal dysplasia with recombinant EDA. Nat Med 2003; 9: 614–618. https://doi.org/10.1038/nm861
- Li X, Wu X, Elston Dm, Zhang J, Zhou C. Hypohidrotic ectodermal dysplasia with c.28delG mutation in ectodysplasin A gene and severe atopic dermatitis treated successfully with tofacitinib. Acta Derm Venereol 2021; 101: 1466. https://doi.org/10.2340/00015555-3707
- Lee H-E, Chang I-K, Im M, Seo Y-J, Lee J-H, Lee Y. Topical minoxidil treatment for congenital alopecia in hypohidrotic ectodermal dysplasia. J Am Acad Dermatol 2013; 68: e139–e140. https://doi.org/10.1016/j.jaad.2012.10.019
- Kowalczyk-Quintas C, Schneider P. Ectodysplasin A (EDA): EDA receptor signalling and its pharmacological modulation. Cytokine Growth Factor Rev 2014; 25: 195–203. https://doi.org/10.1016/j.cytogfr.2014.01.004
- Mokry J, Pisal R. Development and maintenance of epidermal stem cells in skin adnexa. Int J Mol Sci 2020; 21: 9736. https://doi.org/10.3390/ijms21249736
- Ji S-F, Zhou L-X, Sun Z-F, Xiang J-B, Cui S-Y, Li Y, et al. Small molecules facilitate single factor-mediated sweat gland cell reprogramming. Mil Med Res 2022; 9: 13. https://doi.org/10.1186/s40779-022-00372-5
- Tokonzaba E, Chen J, Cheng X, Den Z, Ganeshan R, Müller EJ, et al. Plakoglobin as a regulator of desmocollin gene expression. J Invest Dermatol 2013; 133: 2732–2740. https://doi.org/10.1038/jid.2013.220
- Omori-Miyake M, Yamashita M, Tsunemi Y, Kawashima M, Yagi J. In vitro assessment of IL-4- or IL-13-mediated changes in the structural components of keratinocytes in mice and humans. J Invest Dermatol 2014; 134: 1342–1350. https://doi.org/10.1038/jid.2013.503