SHORT COMMUNICATION
Reduced Fibrinolysis Links Obesity to Cardiovascular Risk in Psoriasis Independently of Inflammation: A Novel Mechanistic Pathway
Eva Klara MERZEL ŠABOVIC1,2,  , Tadeja KRANER ŠUMENJAK3 and Miodrag JANIĆ2,4
, Tadeja KRANER ŠUMENJAK3 and Miodrag JANIĆ2,4
1Dermatovenereology Clinic, University Medical Centre Ljubljana, Ljubljana, 2Faculty of Medicine, University of Ljubljana, Ljubljana, 3Faculty of Agriculture and Life Sciences, University of Maribor, Hoče, and 4Clinical Department of Endocrinology, Diabetes and Metabolic Diseases, University Medical Centre Ljubljana, Ljubljana, Slovenia. E-mail: eva.klara.merzel.sabovic@kclj.si
Citation: Acta Derm Venereol 2025; 105: adv44720. DOI: https://doi.org/10.2340/actadv.v105.44720.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 30, 2025. Accepted after revision: Nov 25, 2025. Published: Dec 16, 2025.
Competing interests and funding: The authors have no conflicts of interest to declare.
This project is funded by the ARIS Slovenian Research and Innovation Agency research and infrastructure programme P3-0308 Atherosclerosis and thrombosis.
INTRODUCTION
Psoriasis is a chronic inflammatory disease characterized by immune dysregulation, oxidative stress, and endothelial dysfunction (1). Beyond its cutaneous manifestations, psoriasis increases cardiovascular risk, in line with recent ESC guidelines identifying chronic inflammation as a risk-enhancing condition (2), particularly in patients with concomitant obesity (3). Obesity itself promotes a pro-inflammatory and pro-thrombotic state through adipose tissue-derived mediators, including plasminogen activator inhibitor-1 (PAI-1), which suppresses fibrinolysis (4). While the links between systemic inflammation, endothelial dysfunction, and atherosclerosis in psoriasis have been extensively studied (5), the role of impaired fibrinolytic activity remains largely underexplored. The overall fibrinolytic potential (OFP), a sensitive integrative, mechanistically relevant marker of fibrinolytic activity and a component of the overall haemostasis potential (OHP) test, is a valuable tool for assessing fibrinolysis (6). Emerging evidence, including our current findings (7), suggests that reduced OFP may serve as a critical mechanistic pathway connecting excess adiposity to enhanced thrombo-inflammatory burden in psoriasis (8).
MATERIALS AND METHODS
Eighty young psoriasis patients (54 men, 26 women, aged 30–45) with well-controlled disease treated with biologics, methotrexate, or topical therapy were included. OFP and OHP were measured as previously described (6). Platelet-poor plasma was prepared, frozen at −80 °C, and analysed in duplicate (intra/inter-assay variability < 5%). OHP was assessed by thrombin- and calcium-induced fibrin formation, and OFP calculated as OHP minus the tPA-induced fibrin curve, reflecting fibrinolytic capacity. Plasma hs-CRP, E-selectin, and other markers were measured with standard immunoassays/enzymatic methods.
Statistical analysis
Patients were stratified by BMI into 2 (< 30 vs ≥ 30 kg/m2) or 3 groups (<25, 25–29.9, ≥ 30 kg/m2). Biomarker distributions (median, IQR) were visualized with violin/box plots. Between-group differences were tested using permutation-based linear regression (20,000 permutations), adjusted for age, sex, smoking, systolic blood pressure, disease duration, and treatment (biologic vs non-biologic). OFP values were logit-transformed to stabilize variance and enable regression analyses. Results are presented for 3 BMI groups (Fig. 1). Spearman correlations were calculated between logit (OFP) and hs-CRP/E-selectin within BMI groups, with trends visualized using geom_smooth. Analyses were performed in R (4.2.3) (R Foundation for Statistical Computing, Vienna, Austria).

Fig. 1. Biomarker distributions (OHP, OFP, hs-CRP and E-selectin) by BMI. Panel A shows biomarkers distributions in patients with BMI < 30 vs. ≥30, while panel B presents OFP across three BMI categories, with obesity associated with lower OFP (49), indicating impaired fibrinolysis. BMI, body mass index; hs-CRP, high sensitivity C-reactive protein; OFP, overall fibrinolysis potential; OHP, overall hemostasis potential.
RESULTS
Biomarker distributions by BMI are shown in Fig. 1. Significant group differences were observed for OHP, OFP, hsCRP, and E-selectin (Fig. 1), while P-selectin and fibrinogen levels did not differ significantly between patients with BMI < 30 and those with BMI ≥ 30 (P-selectin: 41.1 ± 7.9 vs 43.6 ± 6.5; fibrinogen: 3.2 ± 0.7 vs 3.3 ± 0.7). OFP stratification is shown in Fig. 1: Panel A (< 30 vs ≥ 30 kg/m²) and Panel B (3 BMI groups). In obesity, OFP was 49, with values ≤ 45 marking a threshold linked to reduced fibrinolysis and elevated endothelial activation. OFP values were similar across treatment groups, as follows: adalimumab 54.4 ± 10.0, secukinumab 53.8 ± 7.7, guselkumab 54.8 ± 10.3, methotrexate 56.0 ± 6.6, and topical therapy 58.7 ± 7.5. No significant differences were observed between biologic and non-biologic treatment groups, or among the 3 biologic agents’ groups. Correlation analyses showed a strong negative relationship between OHP and OFP in non-obese patients (rho = –0.68, p < 0.001), but not in obese patients, suggesting disruption of the haemostasis–fibrinolysis balance (Fig. 2). OFP correlated weakly and non-significantly with hs-CRP, independent of BMI (Fig. 2, panel A). In contrast, OFP was inversely correlated with E-selectin in both groups (BMI < 30: r = –0.31, p = 0.026; BMI ≥ 30: r = –0.39, p = 0.043) (Fig. 2, panel B), indicating a link between impaired fibrinolysis and endothelial activation, stronger in obesity.
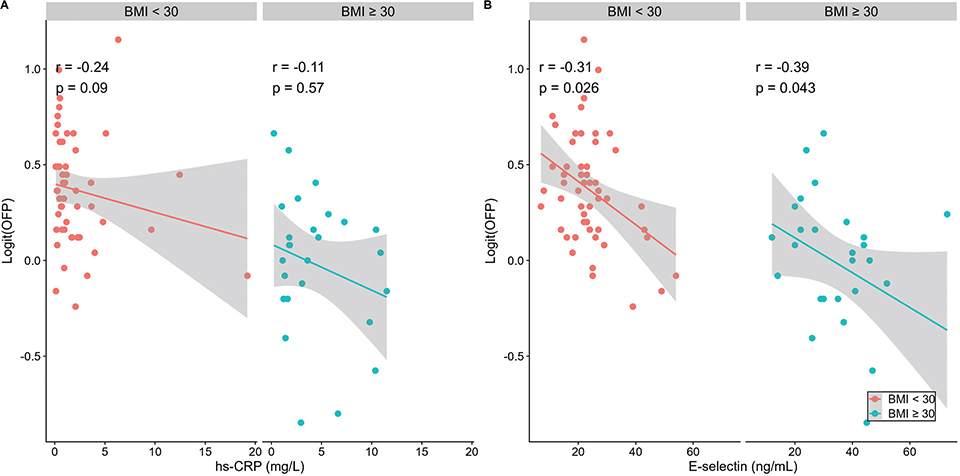
Fig. 2. Correlations of OFP with hs-CRP (panel A) and E-selectin (panel B) by BMI (< 30 and ≥ 30). BMI, body mass index; hs-CRP, high sensitivity C-reactive protein; OFP, overall fibrinolysis potential.
Multivariate regression confirmed obesity as an independent predictor of lower OFP (β = –3.8, p < 0.001), supporting a direct association between obesity and impaired fibrinolysis.
DISCUSSION
In this study, we demonstrate that obesity in psoriasis is associated with reduced OFP, independently of systemic inflammation and traditional confounders. This highlights impaired fibrinolysis as a novel, inflammation-independent mechanism linking excess adiposity to a pro-thrombotic state and endothelial activation, providing insight into how obesity accelerates cardiovascular risk beyond established inflammatory pathways.
Our findings align with evidence linking higher BMI to systemic inflammation and endothelial dysfunction, while identifying reduced OFP as an additional pathway contributing to cardiovascular risk (9). Lower OFP likely reflects obesity-related metabolic changes, including increased PAI-1 production from visceral adipose tissue (4). In our cohort, OFP < 45 consistently indicated impaired fibrinolysis and elevated endothelial activation, suggesting a clinically relevant threshold that requires validation in larger cohorts (10). OFP did not differ by treatment, indicating that biologics do not explain the obesity–fibrinolysis relationship.
OFP appears central to haemostatic balance. In non-obese individuals, OHP and OFP correlate inversely, reflecting preserved equilibrium, whereas this coordination is lost in obesity, indicating a shift towards a pro-thrombotic state. Thus, OFP provides a more specific marker of thrombotic risk than OHP in obesity. Impaired fibrinolysis may further promote endothelial dysfunction through fibrin deposition, inflammatory signalling, and increased PAI-1 release (11–13), creating a strongly pro-thrombotic environment.
Cardiovascular risk is multifactorial (14), and identifying mechanisms specific to obesity in psoriasis is essential. Future research should examine inflammation-independent effects of obesity, including hypofibrinolysis, metabolic changes, oxidative stress, and adipokine signalling. Study limitations include its cross-sectional design, absence of healthy controls, and modest sample size.
Targeting impaired fibrinolysis represents a promising therapeutic approach. Weight loss, dietary modification, and physical activity can reduce PAI-1 and improve fibrinolytic balance (15). Pharmacological strategies such as SGLT2 inhibitors and GLP-1 receptor agonists may also enhance fibrinolysis and reduce thrombotic risk (16), warranting investigation in psoriasis.
From a translational perspective, incorporating OFP into routine cardiovascular risk assessment in psoriasis could enhance risk stratification and support more personalized interventions. Assessing fibrinolytic activity may therefore help capture the specific impact of adiposity-driven pro-thrombotic alterations.
Taken together, these findings underscore reduced fibrinolytic activity, measured as OFP, as both a mechanistic mediator and a potential therapeutic target within the psoriasis–obesity–cardiovascular disease axis. Interventions aimed at restoring fibrinolytic activity through weight reduction, lifestyle modification, and novel pharmacological strategies may provide an effective approach to reduce the heightened cardiovascular risk in this patient population.
ACKNOWLEDGEMENTS
IRB approval status: The study was approved by the Slovenian National Medical Ethics Committee (approval number 0120-422/2021/6).
REFERENCES
- Yamanaka K, Yamamoto O, Honda T. Pathophysiology of psoriasis: a review. J Dermatol 2021; 48: 722–731. https://doi.org/10.1111/1346-8138.15913
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2021; 42: 3227–3237. https://doi.org/10.1093/eurheartj/ehab484
- Gisondi P, Bellinato F, Girolomoni G, Albanesi C. Pathogenesis of chronic plaque psoriasis and its intersection with cardio-metabolic comorbidities. Front Pharmacol 2020; 25: 11. https://doi.org/10.3389/fphar.2020.00117
- Wang L, Chen L, Liu Z, Liu Y, Luo M, Chen N, et al. PAI-1 exacerbates white adipose tissue dysfunction and metabolic dysregulation in high fat diet-induced obesity. Front Pharmacol 2018; 26; 9. https://doi.org/10.3389/fphar.2018.01087
- Cai J, Cui L, Wang Y, Li Y, Zhang X, Shi Y. Cardiometabolic comorbidities in patients with psoriasis: focusing on risk, biological therapy, and pathogenesis. Front Pharmacol 2021; 4: 12. https://doi.org/10.3389/fphar.2021.774808
- Antovic A. The overall hemostasis potential: a laboratory tool for the investigation of global hemostasis. Semin Thromb Hemost 2010; 26: 772-779. https://doi.org/10.1055/s-0030-1265294
- Merzel Šabović EK, Kraner Šumenjak T, Božič Mijovski M, Janić M. Overall hemostatic potential as a marker of subclinical hypercoagulability in treated psoriasis patients. Front Med (Lausanne) 2025; 21: 12. https://doi.org/10.3389/fmed.2025.1611827
- Visser MJE, Venter C, Roberts TJ, Tarr G, Pretorius E. Psoriatic disease is associated with systemic inflammation, endothelial activation, and altered haemostatic function. Sci Rep 2021; 22: 13043. https://doi.org/10.1038/s41598-021-90684-8
- Visser MJE, Tarr G, Pretorius E. Thrombosis in psoriasis: cutaneous cytokine production as a potential driving force of haemostatic dysregulation and subsequent cardiovascular risk. Front Immunol 2021; 16: 12. https://doi.org/10.3389/fimmu.2021.688861
- Gue YX, Ding WY, Lip GY, Gorog DA. Assessment of endogenous fibrinolysis in clinical practice using novel tests: ready for clinical roll-out? SN Appl Sci 2021; 3: 524. https://doi.org/10.1007/s42452-021-04517-4
- Stark K, Massberg S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat Rev Cardiol 2021; 18: 666–682. https://doi.org/10.1038/s41569-021-00552-1
- Jennewein C, Tran N, Paulus P, Ellinghaus P, Eble JA, Zacharowski K. Novel aspects of fibrin(ogen) fragments during inflammation. Mol Med 2011; 4: 568–573. https://doi.org/10.2119/molmed.2010.00146
- Dehghani T, Panitch A. Endothelial cells, neutrophils and platelets: getting to the bottom of an inflammatory triangle. Open Biol 2020; 14: 10. https://doi.org/10.1098/rsob.200161
- Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 2020; 41: 255–323. https://doi.org/10.1093/eurheartj/ehz486
- Bladbjerg EM, Stolberg CR, Juhl CB. Effects of obesity surgery on blood coagulation and fibrinolysis: a literature review. Thromb Haemost 2020; 120: 579–591. https://doi.org/10.1055/s-0040-1702224
- Garg V, Verma S, Connelly K. Mechanistic insights regarding the role of SGLT2 inhibitors and GLP1 agonist drugs on cardiovascular disease in diabetes. Prog Cardiovasc Dis 2019; 62: 349–357. https://doi.org/10.1016/j.pcad.2019.07.005