SHORT COMMUNICATION
Incidence and Prevalence of Prurigo Nodularis from 1995 to 2022: A Nationwide Registry Study from Finland
Laura HUILAJA1![]() , Jari JOKELAINEN2
, Jari JOKELAINEN2![]() and Suvi-Päivikki SINIKUMPU1
and Suvi-Päivikki SINIKUMPU1![]()
1Department of Dermatology, Oulu University Hospital, and Research Unit of Clinical Medicine, University of Oulu, Oulu, Finland, and 2Northern Finland Birth Cohorts, Arctic Biobank, and Infrastructure for Population Studies, University of Oulu, Oulu, Finland. Email: laura.huilaja@oulu.fi
Citation: Acta Derm Venereol 2025; 105: adv-2025-0011. DOI: https://doi.org/10.2340/actadv.v105.adv-2025-0011.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Sept 8, 2025. Accepted after revision: Sept 22, 2025.
Published: Dec 11, 2025.
Competing interests and funding: Our data are from the Finnish Care Register for Health Care (CRHC) maintained by the Finnish Institute of Health and Welfare. According to Finnish laws and regulations, the data in the social welfare and health care registers and documents are confidential. As a responsible authority, FinData can, on a case-by-case basis, grant permission to use the registers and documents for the purposes of scientific research. More information on research authorization applications can be found on www.findata.fi/en.
The study was exempted from institutional review board ethics review because it was retrospective and based only on data from medical records data.
LH has received educational grants from Takeda, Janssen-Cilag, Novartis, AbbVie and LEO Pharma, honoraria from Sanofi Genzyme, Novartis, Abbvie, LeoPharma, BioCryst, UCBPharma and OrionPharma for consulting and/or speaking, and is an investigator for Abbvie and Amgen. SPS has received honoraria from LeoPharma and Sanofi Genzyme for speaking and is an investigator for Abbvie and Amgen. JJ has no conflicts of interest to disclose.
Prurigo nodularis (PN), also called chronic nodular prurigo, is the most common subtype of chronic prurigo (1). A recent meta-analysis based on studies from Europe and the US reported a pooled prevalence of 0.083% (2). It is more frequent in older people than in younger age groups, but most cases are diagnosed in middle-age groups (2).
By using data obtained from the database of the Finnish Care Register for Health Care including information for all healthcare visits to Finnish hospitals, we analysed the incidence and prevalence of PN in Finland. All individuals with a diagnosis of PN recorded at least twice with the code L28.1 of the International Classification of Diseases Version 10, at ≥15 years of age were included. The point prevalence of PN in 2022, with 95% confidence intervals (CI), was calculated by dividing the number of cases by the actual average Finnish population, as reported by Statistics Finland. Crude incidence rates were calculated using annual population-at-risk data from Statistics Finland for the years 1995–2022. Age-standardized incidence rates were calculated using the direct method, with rates standardized to the 2013 European Standard Population. All statistical analyses were performed using the R software package (version 4.2.2; R Core Team, Vienna, Austria) within RStudio (version 2023.03.1 Build 446; RStudio, PBC, Boston, MA, USA).
In total, 4,247 individuals during the period of 1995–2022 fulfilled the inclusion criteria. The total incidence was 3.82/100,000 (95% CI 3.70–3.93), and it remained similar (3.80, 95% CI 3.69–3.92) when the European standard population was used as a reference. The incidence was higher in females than in males, and highest in older age groups (Fig. 1). The point prevalence of PN in 2022 was 7.74/10,000, varying by age groups from 0.29 (95% CI 0.15–0.44) in those aged 15–24 years to 41.6 (95% CI 38.37–44.72) in those aged ≥85 years (Table I).
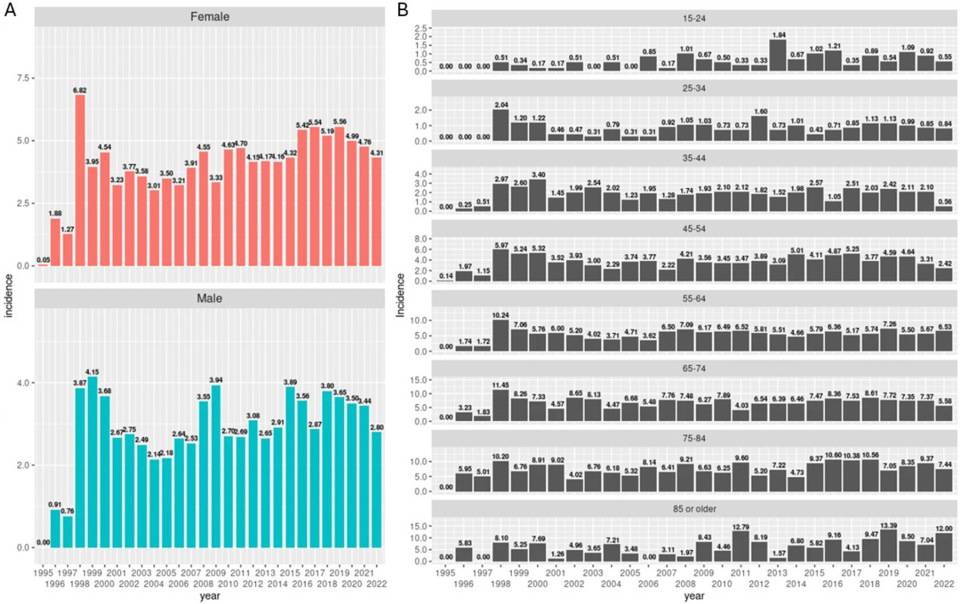
Fig. 1. Incidence of prurigo nodularis in Finland per 100,000 inhabitants. (A) Yearly incidence rates by sex. (B) Yearly incidence in different age groups.
Table I. Prevalence of prurigo nodularis per 10,000 for 2022 by age groups. The point prevalence of prurigo nodularis was calculated by dividing the number of cases by the actual average Finnish population, as reported by Statistics Finland
| Age group | Crude point prevalence | 95% confidence interval |
|---|---|---|
| All | 7.74 | 7.49–8.00 |
| 15–24 | 0.29 | 0.15–0.44 |
| 25–34 | 1.13 | 0.89–1.38 |
| 35–44 | 1.96 | 1.64–2.29 |
| 45–54 | 4.78 | 4.25–5.30 |
| 55–64 | 8.88 | 8.19–9.56 |
| 65–74 | 13.30 | 12.45–14.16 |
| 75–84 | 19.04 | 17.74–20.35 |
| ≥85 | 41.55 | 38.37–44.72 |
Previous studies of PN prevalence have reported varying results, most likely because of methodological differences: a US claims database study reported a similar prevalence (7.2/10,000) (3), whereas another US study that employed another data source and a more stringent definition of PN reported a prevalence of 3.3/10,000 (4). In England, a study across the primary care and inpatient settings reported a prevalence of 3.27/10,000 for 2018 (5). That study also found that PN was most prevalent among the oldest age groups (5). While this chimes with our own findings, it is worth noting that the prevalence in the ≥85 years of age was far higher in our population than that of the English population (13.7/10,000). A Polish study reported notably lower overall prevalence of 6.52/100,000 (6), and similar findings were reported from Germany (7). Interestingly, both the Polish and German studies counted a case of PN based on a single record entry for PN, which could have led to an overestimation of the numbers of cases. By contrast, two nationwide studies carried out in Denmark (8) and Sweden (9) reported point prevalence values of 1.41/10,000 and 1.24/10,000, respectively. Although both these studies also included cases based on a single record entry, they reported prevalence values markedly lower than our own study, which had stricter inclusion criteria.
We found the overall incidence of PN to be 3.82/100,000, which is similar to the finding of an English study (2.88/100,000) (5). It is noteworthy that the English study included data from the primary care setting (while ours was based only on hospital data), and it calculated the incidence for the general population, not only for adults. A more recent study from England, which used primary care data, reported an increase in incidence from 3.61 to 9.31 per 100,000 between 2007 and 2019 (10), a pattern similar to that seen in our own data. However, as previously commented, the inclusion of cases based on a single record entry may have led to overestimation. A nationwide Danish study using hospital data had almost the same study period as ours. It showed that incidence of PN fluctuated between 1998 and 2021, but with a small increasing trend (8). Despite this similarity to our own study, and although the Danish study required only a single record entry for inclusion, it reported annual incidences of PN substantially lower (from 0.58 to 1.45 per 100,000) (8) than those seen in our own population. A steady 0.2% annual increase in incidence was reported over a 3-year period by a German study (7). We found that incidence increased most markedly in the youngest and the oldest age groups. With regard to the oldest age group, this increase could, perhaps, be explained by recent demographic shifts in Finland: particularly during last decade, the proportion of older people has increased drastically. As people live longer, they have more contacts with healthcare providers, which may increase the likelihood that previously undiagnosed skin conditions might be noticed.
The main strengths of this study are the high validity and completeness of its data source, and the minimal selection bias conferred by its registry-based design. On the other hand, the registry-based nature of the design left us unable to confirm the diagnoses. The reliability of the PN diagnosis in our study was increased by the stipulation that the code L28.1 had to appear at least twice in a patient record to qualify counting as a case. We conclude that it appears that PN is slightly more common in Finland than in other countries, and its incidence is increasing in Finland, especially among older people.
REFERENCES
- Thünemann J, Müller S, Steinbrink K, Ständer S, Zeidler C. Chronic prurigo. J Dtsch Dermatol Ges 2024; 22: 813–823. https://doi.org/10.1111/ddg.15317
- Alinaghi F, Jensen MB, Elberling J, Skov L, Loft N. Worldwide prevalence of prurigo nodularis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol 2025; 39: e767–e771. https://doi.org/10.1111/jdv.20585
- Huang AH, Canner JK, Khanna R, Kang S, Kwatra SG. Real-world prevalence of prurigo nodularis and burden of associated diseases. J Invest Dermatol 2020; 140: 480–483.e4. https://doi.org/10.1016/j.jid.2019.07.697
- Kwatra SG, Puelles J, Tran O, Brouillette M, Lillehaugen T, Parthasarathy V, et al. Prevalence of prurigo nodularis in the United States. JAAD Int 2025; 18: 134–136. https://doi.org/10.1016/j.jdin.2023.12.013
- Morgan CLl, Thomas M, Ständer S, Jabbar‐Lopez ZK, Piketty C, Gabriel S, et al. Epidemiology of prurigo nodularis in England: a retrospective database analysis. Br J Dermatol 2022; 187: 188–195. https://doi.org/10.1111/bjd.21032
- Ryczek A, Reich A. Prevalence of prurigo nodularis in Poland. Acta Derm Venereol 2020; 100: adv00155. https://doi.org/10.2340/00015555-3518
- Ständer S, Ketz M, Kossack N, Akumo D, Pignot M, Gabriel S, et al. Epidemiology of prurigo nodularis compared with psoriasis in Germany: a claims database analysis. Acta Derm Venereol 2020; 100: adv00309. https://doi.org/10.2340/00015555-3655
- Elberling J, Ibler KS, Thomsen SF, Bosman K, Olsen J, Torpet M. Incidence and prevalence of prurigo nodularis and associated comorbidities in Denmark from 1998 to 2021. Clin Exp Dermatol 2025; 50: 818–825. https://doi.org/10.1093/ced/llae514
- Antelmi A, Metsini A, Regnell SE, Carlberg M, Svensson Å, von Kobyletzki L. Prevalence of prurigo nodularis in Sweden. J Eur Acad Dermatol Venereol 2024; 38: e904–e906. https://doi.org/10.1111/jdv.19986
- Bahloul D, Hudson R, Balogh O, Mathias E, Heywood B, Hubbuck E, et al. Prevalence, incidence and treatment patterns of prurigo nodularis in England: a retrospective database analysis. Brit J Dermatol 2024; 191: 548–555. https://doi.org/10.1093/bjd/ljae207