SHORT COMMUNICATION
Dimethyl Fumarate Treatment in Patients with Moderate-to-Severe Psoriasis: A 52-week Real-life Study
Laura GNESOTTO1#, Guido MIOSO1#*, Federico BARDAZZI2, Federica FILIPPI2, Vito DI LERNIA3, Alberto MOTOLESE3, Sergio DI NUZZO4, Andrea CONTI5, Federica ARGINELLI5, Monica CORAZZA6, Giulia ODORICI6, Alessandro BORGHI6, Paolo GISONDI7, Luigi NALDI8, Paolo DAPAVO9, Aurora PARODI10, Martina BURLANDO10 and Stefano PIASERICO1
1Dermatology Unit, Department of Medicine, University of Padova, Via Cesare Battisti 206, IT-35128 Padua, 2Department of Experimental, Diagnostic and Specialty Medicine- Division of Dermatology, University of Bologna, Bologna, 3Dermatology Unit, Arcispedale S. Maria Nuova, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, 4Dermatology, Department of Medicine and Surgery, University of Parma, Parma, 5Section of Dermatology, Department of Specialized Medicine, University of Modena and Reggio Emilia, Modena, 6Section of Dermatology and Infectious Diseases, Department of Medical Sciences, University of Ferrara, Ferrara, 7Section of Dermatology, Department of Medicine, University of Verona, Verona, 8Dermatology Unit, San Bortolo Hospital, Vicenza, 9Section of Dermatology, Department of Medical Sciences, University of Turin, Turin and 10University of Genova, DiSSal Section of Dermatology, San Martino Polyclinic Hospital IRCCS, Largo R. Benzi 10 16132 Genova, Italy. E-mail: guido.mioso@gmail.com
#These authors contributed equally to this work.
Citation: Acta Derm Venereol 2023; 103: adv4526. DOI https://doi.org/10.2340/actadv.v103.4526.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Jan 17, 2023; Published: Mar 28, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Psoriasis is a chronic inflammatory immune-mediated disease, with an estimated prevalence of 2–4% in Europe. Recently, a new oral formulation of dimethyl fumarate (DMF) has been approved for treating adults with moderate-to-severe chronic plaque psoriasis (1). The aim of this multicentre retrospective study was to evaluate the effectiveness and safety of DMF in a real-life setting, through collecting and analysing data from DMF-treated patients with moderate-to-severe psoriasis.
MATERIALS AND METHODS
The study retrospectively collected data from DMF-treated adult patients with moderate-to-severe psoriasis presenting to 10 dermatological referral centres located in the central parts of Northern Italy (Bologna, Ferrara, Genova, Modena, Padova, Parma, Reggio-Emilia, Torino, Verona, Vicenza) from January 2019 to March 2021.
Psoriasis Area and Severity Index (PASI) was evaluated at weeks 0, 12, 24, and 52. The study protocol was approved by the local ethics committee (protocol 0053012/ 2022) and informed consent was obtained by the participating subjects. The following data were extracted from electronic medical records: demographics (sex and age), body mass index (BMI), comorbidities, psoriasis duration, psoriatic arthritis (PsA), clinical or laboratory side-effects.
Statistical analysis
PASI reduction ≥ 50% and ≥ 75% from baseline (PASI 50 and PASI 75, respectively) were assessed using both intention-to-treat (ITT) and per-protocol analysis (PP). In the ITT analysis, patients who withdrew from the study for any reason were defined as non-responders. Differences between psoriasis patients at baseline and at short-term or intermediate-term therapy were analysed using repeated measures of 1-way analysis of variance (ANOVA). Analyses were performed using IBM-SPSS software v.25 (Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
RESULTS
Patient characteristics
The current study included 270 patients, 170 (63%) men, and 100 (37%) women, mean age ± standard deviation (SD) 55.8 ± 15.3 years (range 19–88 years), BMI 26.8 ± 4.4 kg/m2 and psoriasis duration 17.4 ± 12.9 years.
A total of 160 patients (69.9%) underwent systemic therapy before DMF initiation, whereas 14 patients (6.1%) had previously been treated with biological drugs. Co-morbid conditions were reported in 198 (73.3%) patients (Table SI). In the study population, 90 were elderly patients (> 65 years), 58 (64.4%) men, and 32 (35.6%) women, mean age ± SD 72.2 ± 5.9 years (range 65–88 years), BMI 27±3.9 kg/m2 and psoriasis duration 20.8±14.4 years.
Efficacy of dimethyl fumarate
Mean baseline PASI was 9.9 ± 5.7, which decreased to 4.6, 2.9, and 2.3 after 12, 24 and 52 weeks of treatment, respectively (p < 0.001). At 12 weeks, PASI 50 was achieved by 109 patients (40.4% of the ITT population and 61.9% of the PP population), while PASI 75 was obtained by 46 patients (17% ITT, 25.8% PP).
At 52 weeks, PASI 50 and PASI 75 were achieved by 53 patients (19.6% ITT, 88.3% PP) and 40 patients (14.8% ITT, 66.7% PP), respectively (Fig. 1). Among the 90 elderly patients, PASI 50 and PASI 75 were achieved by 42 (46.7% ITT, 71.2% PP) and 22 patients (24.4% ITT, 36.7% PP), respectively, at 12 weeks. At 52 weeks, PASI 50 and 75 were achieved by 22 (24.4% ITT, 95.7% PP) and 16 patients (17.8% ITT, 69.6%PP), respectively (Fig. 2).
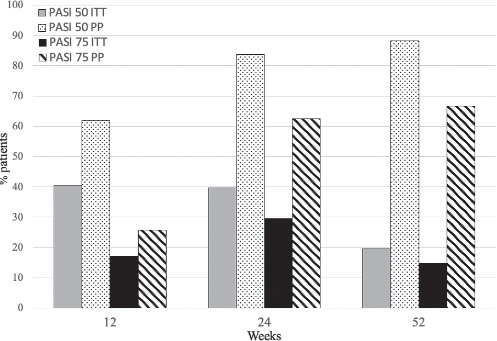
Fig. 1. Psoriasis Area and Severity Index (PASI) 50 and 75 rates after 12, 24 and 52 weeks (intention-to-treat (ITT) and per-protocol (PP) analysis).
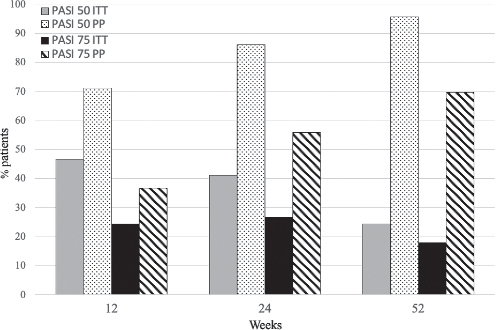
Fig. 2. Psoriasis Area and Severity Index (PASI) 50 and 75 rates in elderly patients (>65 years) after 12, 24 and 52 weeks (intention-to-treat (ITT) and per-protocol (PP) analysis).
Safety profile of dimethyl fumarate
At least 1 adverse event was experienced by 163 (60.4%) patients, while 71 patients (26.6%) experienced laboratory side-effects. Overall, 116 (42.9%) patients interrupted the treatment because of side-effects.
The most common were gastrointestinal disorders (Table SII). Among the elderly group, 35 patients (38.9%) interrupted the treatment because of side-effects. However, the percentage was lower, albeit not significantly, compared with that of the younger patients (45.8%).
DISCUSSION
This is the largest study of real-life use of DMF in adult patients with moderate-to-severe psoriasis, and the first to compare different evaluation methods (ITT and PP analyses) to handle a loss to follow-up. ITT and PP analyses revealed that PASI 75 was achieved by 14.8% and 66.7% of patients at 52 weeks, respectively.
Sparse data have been published regarding the real-world use of DMF (2–6). Moreover, most studies have focused on fumaric acid esters (FAE) (7–11). The find-ings of the current study are in agreement with those of a few studies on DMF. A real-life study by Malara et al. (2) on 36 patients reported a PASI 75 reached by 16% of patients at 16 weeks and by 61% of patients at 52 weeks (PP analysis). Other studies (3–6) confirmed DMF efficacy in a real-life scenario, revealing PASI 75 responses ranging from 17.5% to 33.3% of patients at the end of the observation period. Overall, PASI 75 achieved with DMF may not seem remarkable compared with other therapies for psoriasis. However, in a long-term analysis, a recent study showed that DMF has an efficacy comparable to other systemic treatments (6). In a subgroup population of 90 elderly patients it was found that PASI 50 and PASI 75 at 12, 24 and 52 weeks were higher than the entire population. DMF efficacy in elderly patients was also evaluated in a recent smaller retrospective multicentre study by Ricceri et al. (12). The mean PASI score at baseline was 9.8±4.1, which decreased to 4.3±3.2 at 16 weeks and 2.7±3.2 at 24 weeks. Previous randomized clinical trials reported that the main adverse events related to DMF therapy were gastrointestinal disorders (62.7%), especially diarrhoea (38.8%), upper abdominal pain (20.1%), and abdominal pain (19.7%) (13). Lijnen et al. (3) confirmed the high incidence of gastrointestinal disorders (58%) and reported a particularly great frequency of skin flushing (65%) and neutrophilia (65%).
The current study observed that 86.7% of patients experienced at least 1 side-effect; nausea (23.7%), diarrhoea (27.8%) and flushing (16.7%) being the most common. Overall, 43% of the patients studied had to discontinue the treatment due to side-effects. Similarly to the current study results, Walker et al. (8) reported that 43.4% of patients stopped FAE therapy due to an adverse event, mostly gastrointestinal disorders. In the current study population, 38 patients treated with DMF had an oncological history, and none experienced a relapse of malignancy during the follow-up period, as also reported by Corazza et al. (4). This may be related to the mild immunosuppressant effect of DMF.
The strengths of the current study include the large cohort of patients and the long period of observation (up to 52 weeks). Study limitations include the retrospective design and its multicentric nature, which could not allow a homogeneous patient selection.
In conclusion, the results of this study demonstrate the good effectiveness and excellent safety of treatment with DMF in a real-life setting in adult patients with moderate-to-severe psoriasis. DMF might not be the best choice when a high efficacy is needed, but its advantage may be the possibility to use this treatment in patients with multiple comorbidities and malignancy, even in elderly patients. However, further real-life studies are required to investigate treatment response patterns according to the heterogeneous psoriasis phenotypes, the long-term effectiveness and safety of the drug, and the identification of the best responder patient profile.
REFERENCES
- Mrowietz U, Barker J, Boehncke WH, Iversen L, Kirby B, Naldi L, et al. Clinical use of dimethyl fumarate in moderate-to-severe plaque-type psoriasis: a European expert consensus. J Eur Acad Dermatol Venereol 2018; 32: 3–14.
- Malara G, Fabbrocini G, Trifirò C, Burlando M. Dimethyl fumarate titration for the systemic treatment of moderate-to-severe plaque psoriasis. Drugs Context 2021; 10: 2020–12–4.
- Lijnen R, Otters E, Balak D, Thio B. Long-term safety and effectiveness of high-dose dimethylfumarate in the treatment of moderate to severe psoriasis: a prospective single-blinded follow-up study. J Dermatolog Treat 2016; 27: 31–36.
- Corazza M, Odorici G, Conti A, Di Lernia V, Motolese A, Bardazzi F, et al. Dimethyl fumarate treatment for psoriasis in a real-life setting: a multicentric retrospective study. Dermatol Ther 2021; 34: 15066.
- Esposito M, Campanati A, Giunta A, Calianno G, Bianchi L, Diotallevi F, et al. Dimethyl fumarate’s effectiveness and safety in psoriasis: a real-life experience during the COVID-19 pandemic. Dermatol Ther (Heidelb) 2022; 12: 671–681.
- Pezzolo E, Cazzaniga S, Di Leo S, Naldi L; PsoReal Study Group. Efficacy and safety of dimethyl fumarate in comparison with conventional therapy for psoriasis: an Italian real-world clinical experience. J Eur Acad Dermatol Venereol. 2022; 36: 534–537
- Hoefnagel JJ, Thio HB, Willemze R, Bouwes Bavinck JN. Long-term safety aspects of systemic therapy with fumaric acid esters in severe psoriasis. Br J Dermatol 2003; 149: 363–369.
- Walker F, Adamczyk A, Kellerer C, Belge K, Brück J, Berner T, et al. Fumaderm® in daily practice for psoriasis: dosing, efficacy and quality of life. Br J Dermatol 2014; 171: 1197–205.
- Dickel H, Bruckner T, Altmeyer P. Long-term real-life safety profile and effectiveness of fumaric acid esters in psoriasis patients: a single-centre, retrospective, observational study. J Eur Acad Dermatol Venereol 2018; 32: 1710–1727.
- Mrowietz U, Sorbe C, Reich K, Von Kiedrowski R, Weckbecker J, Radtke MA, et al. Fumaric acid esters for the treatment of psoriasis in Germany: characterising patients in routine care. Eur J Dermatol 2020; 30: 41–48.
- Termeer C, Reinhold U, Dirschka T, von Kiedrowski R, Kurzen H. Long-term use of fumaric acid esters for the treatment of psoriasis in daily practice. J Dermatolog Treat 2021; 32: 610–616.
- Ricceri F, Bardazzi F, Buggiani G, Burlando M, Campione E, Corazza M, et al. Efficacy and safety of dimethylfumarate in elderly psoriasis patients: a multicentric Italian study. J Dermatolog Treat 2021; 11: 1–4.
- Mrowietz U, Szepietowski JC, Loewe R, van de Kerkhof P, Lamarca R, Ocker WG, et al. Efficacy and safety of LAS41008 (dimethyl fumarate) in adults with moderate-to-severe chronic plaque psoriasis: a randomized, double-blind, Fumaderm®-and placebo-controlled trial (BRIDGE). Br J Dermatol 2017; 176: 615–623.