ORIGINAL REPORT
Catastrophizing in Chronic Itch: Associations with Demographic, Clinical and Psychological Factors
Isabel NIEMEYER1![]() , Pascale SALAMEH1,2,3,4,5
, Pascale SALAMEH1,2,3,4,5![]() , Hanna H. LINẞ1
, Hanna H. LINẞ1![]() , Eva M. GREKOWITZ1,2
, Eva M. GREKOWITZ1,2![]() , Leonie S. HERZOG1,2
, Leonie S. HERZOG1,2![]() , Martin METZ1,2
, Martin METZ1,2![]() and Manuel P. PEREIRA1,2*
and Manuel P. PEREIRA1,2*![]()
1Institute of Allergology, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany, 2Fraunhofer Institute for Translational Medicine and Pharmacology ITMP, Immunology and Allergology, Berlin, Germany, 3Gilbert and Rose-Marie Chagoury School of Medicine, Lebanese American University, Beirut, Lebanon, 4Department of Primary Care and Population Health, University of Nicosia Medical School, 2417, Nicosia, Cyprus, and 5Institut National de Santé Publique d'Épidémiologie Clinique et de Toxicologie-Liban (INSPECT-LB), Beirut, Lebanon
Corr: Manuel P. Pereira, Charité – Universitätsmedizin Berlin, Institute of Allergology, Hindenburgdamm 30, 12203 Berlin, Germany. *Email: manuel.pereira@charite.de
Key words: chronic pruritus; itch; catastrophizing; chronic prurigo; chronic urticaria; chronic pruritus of unknown origin.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0083. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0083.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 8, 2025. Accepted after revision: Feb 19, 2026.
Published: Mar 2, 2026.
Competing interests and funding: The authors received no funding for this work.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
This study was approved by the local Ethics Committee (Charité – Universitätsmedizin Berlin, nr.: EA4/072/23). All study procedures were performed according to the Declaration of Helsinki and later revisions.
LSH has received travel fees from Celltrion and CSL Behring. MM is or was an investigator for Allakos, Amgen, AstraZeneca, Celldex, Escient, Galderma, Incyte, Jasper, Novartis, Sanofi, Third Harmonic Bio, Trevi; has received consulting fees from Advanz, Allegria, Arcus, Attovia, Blueprint, Deep Apple, Enanta, Evommune, FatiAbGen, Granular, Japan Tob., Lilly, Lycia, Ono, RAPT, Sanibel, Santa Ana Bio, Septerna, Tupos, Vifor; and has received honoraria as a speaker from AbbVie, ALK Abelló, Almirall, Amgen, Beiersdorf, Berlin-Chemie, Celldex, Celltrion, Enanta, Galderma, Genzyme, GSK, Johnson & Johnson, Novartis, Pfizer, Regeneron, Sanofi, Vifor. MPP has received research funding from Almirall, Clinuvel and Pfizer; is an investigator for Allakos, ARS Pharmaceuticals, Celldex Therapeutics, Escient, Incyte and Sanofi; has received consulting fees from Almirall, Galderma, Incyte and Sanofi; and has received speaker honoraria and/or travel fees from AbbVie, Amgen, Beiersdorf, Celltrion, CSL Behring, Doctorflix, Eli Lilly, Falk Foundation, FomF GmbH, GA2LEN, Galderma, Novartis, P.G. Unna Academy, Sanofi, StreamedUP, TouchMDT and Zai Lab. IN, PS, HH and EMG have no conflict of interest to declare.
Catastrophizing, defined as an overly negative evaluation of one’s situation, is associated with worse disease outcomes in patients with chronic pain but remains unexplored in pruritus medicine. In this cross-sectional study, we included patients with chronic prurigo (CPG, n=50), chronic pruritus on nonlesional skin (CPNL, n=50) and chronic spontaneous urticaria (CSU, n=50) to investigate catastrophizing and determine possible associations with demographic and clinical factors. Patients completed validated questionnaires assessing catastrophizing (Itch-Cognition-Questionnaire), itch intensity, disease control, quality of life, anxiety, depression, stress and attention to itch. We recorded median [interquartile range] catastrophizing scores of 19.0 [11.0; 29.0] for CPG, 17.0 [11.8; 24.3] for CPNL and 10.0 [5.0; 18.3] for CSU patients. Catastrophizing correlated positively with itch intensity (r=0.382–0.678, p<0.001–0.006), quality of life impairment (r=0.554–0.716, p<0.001) and vigilance and awareness to itch (r=0.407–0.591, p<0.001–0.003) across patient groups. Linear regression analysis revealed a lower likelihood of catastrophizing in CSU patients (CSU: β=−5.905, p<0.001; CPG: reference), a positive association of catastrophizing with average itch intensity (β=1.119, p=0.008) and attention to itch (β=0.150, p<0.001), and a negative association with age (β=−0.095, p=0.004) and short disease duration (β=−5.797, p=0.049). Catastrophizing represents a pivotal cognitive process, which is associated with worse clinical outcomes in chronic itch patients.
SIGNIFICANCE
Catastrophizing is the tendency to evaluate one’s situation overly negative and is associated with worse disease outcomes. We investigated catastrophizing in patients with chronic itch of different origins and its relation with demographic, clinical and psychological factors. Catastrophizing was associated with higher average itch intensity and attention to itch, with patients with chronic prurigo showing a higher likelihood of catastrophizing. Patients with well-controlled disease displayed lower catastrophizing levels, while a negative association between catastrophizing and age was observed. Catastrophizing is a significant cognitive process in chronic diseases and is particularly associated with poorer outcomes in chronic itch patients.
Catastrophizing is defined as the tendency to overrate the negative aspects of a certain situation (1). In a medical context, patients who catastrophize have a lower expectation and a more negative evaluation of the disease outcome and the treatment. Catastrophizing is well researched in the pain field, with higher levels of catastrophizing being associated with more pain (2). Additionally, patients with chronic pain conditions, such as fibromyalgia and chronic back pain, show higher catastrophizing than healthy controls (3, 4, 5).
In pruritus medicine, catastrophizing has rarely been investigated. A positive association between catastrophizing and itch intensity has been recorded in patients with atopic dermatitis (6). Moreover, in a study including patients with atopic dermatitis, psoriasis and dry skin, catastrophizing was associated with itch intensity, frequency and duration (7). Nevertheless, this phenomenon remains unexplored in other chronic pruritic conditions. Chronic pruritus (CP, i.e., lasting for ≥6 weeks) is highly heterogeneous in terms of origin and clinical presentation (8). CP may arise from dermatological and nondermatological conditions (e.g. systemic or neuropathic diseases) and occur on inflamed or nonlesional skin, or accompanied by chronic scratch lesions, such as chronic prurigo (CPG) (9). Previous studies revealed disparities in disease-associated burden across various CP conditions and clinical presentation (10, 11). The degree of catastrophizing may also vary across different forms of CP and may have varying impact on symptom severity and chronicity of the disease. Particularly, patients with visible skin lesions (as, e.g., in CPG) may exhibit more pronounced patterns of catastrophizing compared to those with CP on nonlesional skin (CPNL), while a more fluctuating itch as in chronic spontaneous urticaria (CSU) may differently influence catastrophizing compared to a more constant perceived itch experienced in other conditions.
The aim of the study was (i) to investigate catastrophizing in patients with CPG, CPNL and CSU; and (ii) to analyse demographic, clinical and psychological factors associated with catastrophizing across CP conditions.
METHODS
Patient population
Adult patients (≥18 years) with CPG, CPNL or CSU were recruited at the outpatient clinic of the Institute of Allergology, Charité – Universitätsmedizin Berlin (Germany) from May 2023 until March 2025. Only patients reporting a worst itch intensity on the numerical rating scale in the previous 24 h (WI-NRS-24h) of 3/10 or more were included. Patients unwilling or unable to complete the study questionnaires were excluded.
Study design
This was a prospective, cross-sectional study. After signing the informed consent, all patients were examined by a board-certified dermatologist. Physicians recorded patients’ medical history including demographics (age, sex, ethnicity), disease duration, current antipruritic therapy, comorbidities and co-medication. Patients completed validated questionnaires assessing catastrophizing, as well as itch intensity, disease control, impairment of quality of life due to itch, anxiety, depression and stress, and vigilance and awareness to itch.
Patient-reported outcome measures (PROMs)
Patients were instructed to record their worst and average itch intensity in the previous 24 h and 4 weeks on a numerical rating scale ranging from 0 (no itch) to 10 (worst imaginable itch; WI-NRS-24h/4w, AI-NRS-24h/4w) (12, 13). To assess the impact of CP on quality of life, patients completed the ItchyQol questionnaire. This instrument consists of 3 subscales (symptom, 6 items; function, 7 items; emotion, 9 items), each with a scoring range from 1 to 5 (14). Patients with CPG completed the disease-specific 5-item Prurigo Control Test (PCT) (15), which measures patients' overall control of the disease. The score ranges from 0 to 20, with scores ≥10 denoting well-controlled and scores <10 poorly controlled disease. Patients with CSU were instructed to complete the 4-item Urticaria Control Test (UCT; range 0-16) (16), also used to assess the overall control of the disease. A score of ≤12 indicates poorly controlled disease, whereas a score between 12 and 15 indicates a well-controlled disease and a score of 16 indicates a fully controlled disease.
To assess catastrophizing, all patients completed the Itch-Cognition-Questionnaire (Juckreiz-Kognitions-Fragebogen, JKF). This scale is used to measure the extent of negative cognitive evaluations and feelings of helplessness that patients experience in relation to their pruritus. It consists of 10 questions addressing helplessness, despair, sleep impairment and scratching behaviour (17). Moreover, the Vigilance and Awareness Questionnaire (18) was used to assess the patients' cognitive alertness and awareness. It contains 16 items with a scoring range from 0 to 80. To screen for anxiety, depression and stress disorders, the Depression Anxiety Stress Scales (DASS; range 0–42) (19) were used.
Statistics
The sample size calculation was based on a medium effect size of 0.15, a power of 80% and an alpha level of 5%, yielding a minimum of 139 participants (G*Power®, v. 30.0.10). To account for potential missing data, a total of 150 participants were planned.
The statistical analysis was carried out using IBM SPSS Statistics®, v. 29.0.1.1. Data are shown as number of cases (percentage) and median [interquartile range]. We used Spearman rank for correlation analyses, and the Mann–Whitney U test or Kruskal–Wallis test for group comparisons as appropriate. A linear regression analysis was performed to investigate associations between catastrophizing and demographic, clinical and psychological factors; the model assumptions were checked for the model before acceptance (linear relationship, residues’ normality, absence of collinearity and homoscedasticity). Ethnicity was entered as a binary variable (Caucasian vs non-Caucasian) due to the small number of non-Caucasian participants included in this study. Missing data were handled using complete case analysis. The significance level was defined as p<0.05.
RESULTS
Study population
The study included 150 patients (median age 61.5 years, range 20–89); of which, 96 (64.0%) were female and 54 (36.0%) were male. Most patients were Caucasian (n=131, 87.3%), while other ethnic backgrounds were less represented. Cardiac diseases were the most common comorbidities (n=66, 44.0%), followed by allergic (n=50, 33.3%) and endocrine (n=41, 27.3%) conditions (Table I).
| Parameters | Chronic prurigo n=50 |
Chronic pruritus n=50 |
Chronic urticaria n=50 |
|---|---|---|---|
| Sex (m/f), n (%) | m: 16 (32%) f: 34 (68%) |
m: 26 (52%) f: 24 (48%) |
m: 12 (24%) f: 38 (76%) |
| Age (years), median [IQR], n | 67.0 [55.8; 76.3], n=50 |
63.5 [43.8; 80.0] , n=50 |
49.0 [31.0; 63.3] , n=50 |
| Ethnicity, n (%) Caucasian Middle East Black/African-American South Asian Southeast Asian Hispanic-American/Latino Other |
43 (86%) 1 (2%) 0 (0%) 1 (2%) 1 (2%) 0 (0%) 4 (8%) |
44 (88%) 2 (4%) 2 (4%) 0 (0%) 0 (0%) 0 (0%) 2 (4%) |
44 (88%) 1 (2%) 0 (0%) 1 (2%) 1 (2%) 1 (2%) 2 (4%) |
| Comorbidities, n (%) Cardiologic Allergologic Endocrinologic Psychiatric Rheumatologic/Orthopaedic Nephrological Haematologic Hepatologic Neurological Pulmonologic Other |
29 (58%) 18 (36%) 18 (36%) 7 (14%) 7 (14%) 5 (10%) 2 (4%) 2 (4%) 1 (2%) 1 (2%) 29 (58%) |
26 (52%) 12 (24%) 13 (26%) 8 (16%) 4 (8%) 3 (6%) 4 (8%) 2 (4%) 1 (2%) 1 (2%) 27 (54%) |
11 (22%) 20 (40%) 10 (20%) 11 (22%) 6 (12%) 2 (4%) 1 (2%) 0 (0%) 2 (4%) 0 (0%) 26 (52%) |
|
Patients with chronic prurigo, chronic pruritus on nonlesional skin and chronic urticaria were included in this study. The sex distribution, median age, ethnicity and comorbidities are shown for each patient group. f:female; IQR:interquartile range; m:male. |
|||
Clinical features
All 3 patient groups (each n=50) showed moderate to severe itch intensities with median scores ranging from 3.0 to 8.0 (Table II). The WI-NRS-24h differed significantly between groups (p=0.009), with lower itch scores in CSU compared to CPG (p=0.004) and CPNL (p=0.016), while no difference was observed between CPG and CPNL patients (p=0.660). In addition to itch, other sensory qualities were frequently reported, especially pain (n=59, 39.3%), burning (n=58, 38.7%) and tingling (n=41, 27.3%; Table II).
Table II. Disease-specific characteristics
| Parameters | Chronic prurigo n=50 |
Chronic pruritus n=50 |
Chronic urticaria n=50 |
|---|---|---|---|
| Itch intensity, median [IQR] WI-NRS 24 h AI-NRS 24 h WI-NRS 4 w AI-NRS 4 w |
6.0 [4.0; 8.0] 5.0 [3.0; 7.0] 8.0 [4.8; 9.0] 5.0 [3.0; 7.0] |
6.0 [4.0; 8.0] 5.0 [3.0; 7.0] 7.0 [5.0; 8.3] 6.0 [4.0; 7.0] |
4.0 [3.0; 6.0] 3.0 [3.0; 5.0] 7.0 [4.0; 8.3] 4.0 [3.0; 7.0] |
| Sensory symptoms, n (%) Pain Burning Tingling Stinging |
25 (50%) 18 (36%) 12 (24%) 13 (26%) |
19 (38%) 19 (38%) 14 (28%) 16 (32%) |
15 (30%) 21 (42%) 15 (30%) 10 (20%) |
| PCT, median [IQR] Well-controlled, n (%) Poorly controlled, n (%) |
8.0 [3.0; 11.0] 15 (30%) 35 (70%) |
n.a. | n.a. |
| UCT, median [IQR] Well-controlled, n (%) Poorly controlled, n (%) |
n.a. | n.a. | 8.0 [4.5; 10.5] 10 (20%) 39 (80%) |
|
Itch intensity, frequency of sensory symptoms and disease control are shown for each patient group Data sets were complete for all variables with n=50 per group, except for UCT where one value was missing (n=49). AI-NRS-24h/4w:average itch intensity on the numerical rating scale in the last 24 hours/4 weeks; IQR:interquartile range; n.a.:not applicable; PCT:Prurigo Control Test; UCT:Urticaria Control Test; WI-NRS-24h/4w:worst itch intensity on the numerical rating scale in the last 24 hours/4 week. |
|||
Only 15 CPG patients (30%) showed a controlled condition according to the PCT. As for CSU, 10 patients (20.4%) showed a controlled disease, and 39 (79.6%) a poorly controlled condition (Table II).
Treatment
At the study visit, most CPG patients were being treated with emollients (n=37; 74.0%) and topical corticosteroids (n=27, 54.0%). A total of 26 (52.0%) were under a biologic therapy (dupilumab: n=22, nemolizumab: n=3, tralokinumab: n=1), while 9 (18.0%) were receiving gabapentinoids. As for CPNL patients, emollients (n=35; 70.0%) and antihistamines (n=30, 60.0%) were the most commonly used therapies, whereas other treatments were rarely administered. The majority of patients with CSU received antihistamines (n=42, 84%) and 17 (34%) were under omalizumab therapy (Table SI).
Disease-related burden
Patients recorded a moderate to severe impact of itch on quality of life across all subscales of the ItchyQol (Table III). ItchyQol scores were significantly higher in CPG compared to CSU (p=0.005), while no significant differences were observed across the other patient groups. Most patients indicated a moderate to severe impairment of their quality of life (n=100, 66.7%) and of their sleep (n=90, 60%; Table III).
Table III. Disease-related burden
| Parameters | Chronic prurigo n=50 |
Chronic pruritus n=50 |
Chronic urticaria n=50 |
|---|---|---|---|
| JKF, median [IQR] | 19.0 [11.0; 29.0] | 17.0 [11.8; 24.3] | 10.0 [5.0; 18.3] |
| ItchyQol, median [IQR] Symptom Function Emotion Total score |
4.0 [3.0; 4.0] 3.0 [2.8; 4.0] 3.0 [2.0; 4.0] 3.0 [2.0; 4.0] |
3.0 [2.0; 4.0] 3.0 [2.0; 4.0] 3.0 [2.0; 4.0] 3.0 [2.0; 4.0] |
3.0 [2.0; 3.0] 3.0 [2.0; 3.0] 3.0 [2.0; 3.0] 3.0 [2.0; 3.0] |
| Vigilance and Awareness Questionnaire, median [IQR] | 41.0 [27.8; 54.0] | 39.5 [32.0; 49.3] | 36.0 [27.5; 46.0] |
| DASS Depression, median [IQR] Normal, n (%) Mild, n (%) Moderate, n (%) Severe, n (%) Extremely severe, n (%) |
8.0 [2.0; 16.0] 16 (32%) 7 (14%) 6 (12%) 3 (6%) 18 (36%) |
8.0 [2.0; 22.5] 19 (38%) 5 (10%) 3 (6%) 3 (6%) 20 (40%) |
8.0 [2.0; 16.5] 22 (44%) 0 (0%) 7 (14%) 4 (8%) 17 (34%) |
| Anxiety, median [IQR] Normal, n (%) Mild, n (%) Moderate, n (%) Severe, n (%) Extremely severe, n (%) |
6.0 [1.5; 12.0] 17 (34%) 6 (12%) 5 (10%) 5 (10%) 17 (34%) |
8.0 [0.0; 14.0] 16 (32%) 3 (6%) 3 (6%) 5 (10%) 23 (46%) |
9.0 [0.0; 16.0] 18 (36%) 3 (6%) 2 (4%) 2 (4%) 25 (50%) |
| Stress, median [IQR] Normal, n (%) Mild, n (%) Moderate, n (%) Severe, n (%) Extremely severe, n (%) |
14.0 [6.0; 22.5] 13 (26%) 2 (4%) 8 (16%) 8 (16%) 19 (38%) |
14.0 [6.0; 24.5] 16 (32%) 1 (2%) 5 (10%) 7 (14%) 21 (42%) |
16.0 [6.0; 22.0] 14 (28%) 3 (6%) 3 (6%) 6 (12%) 24 (48%) |
| Impairment QoL, n (%) Not at all Minimal Moderate Severe |
6 (12%) 8 (16%) 21 (42%) 15 (30%) |
1 (2 %) 13 (26%) 25 (50%) 11 (22%) |
3 (6 %) 19 (38%) 20 (40%) 8 (16%) |
| Impairment sleep, n (%) Not at all Minimal Moderate Severe |
10 (20%) 8 (16%) 14 (28%) 18 (36%) |
1 (2 %) 11 (22%) 21 (42%) 17 (34%) |
11 (22%) 19 (38%) 12 (24%) 8 (16%) |
|
Findings from questionnaires assessing catastrophizing, impairment of quality of life, sleep disruption, vigilance and awareness of itch, anxiety, depression and stress are reported. All data sets were complete with no missing data (n=50 per group). DASS:Depression Anxiety Stress Scale; IQR:interquartile range; ItchyQoL:Itchy Quality of Life Questionnaire; JKF:Itch-Cognition-Questionnaire; QoL:Quality of Life. |
|||
More than half of the patients showed signs of moderate to extremely severe depression, and severe to extremely severe anxiety and stress, as assessed by the DASS (Table III). No significant differences across diagnoses were found for DASS-Depression (p=0.650), DASS-Anxiety (p=0.782), or DASS-Stress (p=0.856).
Catastrophizing
We recorded median catastrophizing scores of 19.0 [11.0; 29.0] for CPG, 17.0 [11.8; 24.3] for CPNL and 10.0 [5.0; 18.3] for CSU patients, as assessed by the JKF scale (Fig. 1, Table III). The JKF scores differed significantly between groups (p<0.001). Patients with CSU reported lower scores compared to patients with CPNL (p=0.003) and CPG (p<0.001), whereas no difference was observed between CPNL and CPG patients (p=0.485). No sex differences were observed in catastrophizing (p=0.677), and no correlation was found between age and the JKF score (p=0.969). Patients with well-controlled disease showed lower JKF scores compared to those with poorly controlled disease, both in CPG (p<0.001) and CSU (p=0.022), as assessed by the PCT and UCT, respectively. However, patients receiving biologics or small molecules did not differ in catastrophizing scores across diagnoses (CPG: p=0.120; CPNL: p=0.478; CSU: p=0.774).
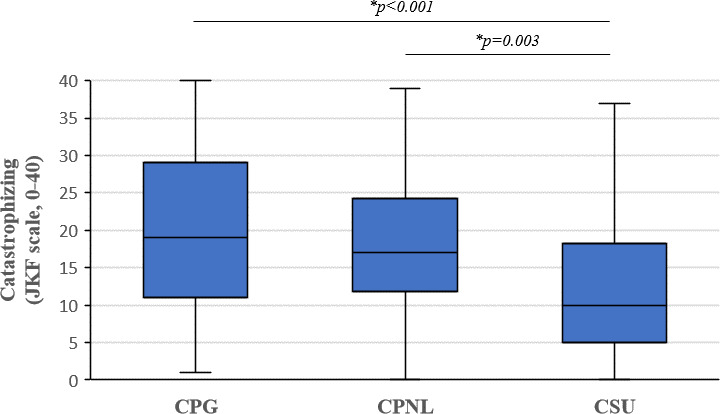
Fig. 1. Catastrophizing scores across pruritic conditions. Catastrophizing was assessed using the validated JKF questionnaire. We recorded higher catastrophizing in patients with CPG and CPNL compared to patients with CSU (Kruskal–Wallis test). Middle line: median; bottom/top of box: 1st/3rd quartile; whiskers: lowest/highest case within 1.5 times interquartile range. N=50 per patient group.
Median vigilance and awareness scores were 41.0 [27.8; 54.0] in CPG, 39.5 [32.0; 49.3] in CPNL and 36.0 [27.5; 46.0] in CSU patients (Table III), while no significant differences across diagnoses were observed (p=0.187).
We recorded weak-to-moderate positive correlations between JKF scores and itch intensity across all diagnoses (r=0.382–0.678, p<0.001–0.006). As for quality of life, there were moderate-to-strong positive correlations between the JKF score and the ItchyQol (r=0.554–0.716, p<0.001), with the strongest associations recorded for the subscale emotion. Except for the subscale anxiety in CSU patients, all 3 subscales of DASS correlated positively with the JKF across the 3 patient groups (r=0.348–0.658, p<0.001–0.013). Moreover, catastrophizing and vigilance scores correlated positively across all patient groups (r=0.407–0.591, p<0.001–0.003; Table SII).
Linear regression analysis (Table IV) revealed that patients with CSU were less likely to show high catastrophizing scores compared to CPG (CSU: β=−5.905, p<0.001; CPG: reference). Catastrophizing was negatively associated with age (β=−0.095, p=0.004) and a short disease duration of 6–12 months (β=−5.797, p=0.0049). Among itch intensity measures, only AI-NRS-24h showed a significant positive association with catastrophizing (β=1.119, p=0.008). In addition, vigilance and awareness of itch were strongly positively associated with catastrophizing (β=0.150, p<0.001).
Table IV. Linear regression analysis investigating the association between catastrophizing and demographic, clinical and psychological factors (n=150)
| Demographic and clinical factors | Beta | Standard error | 95% confidence interval | p-value |
|---|---|---|---|---|
| Diagnosis CPG CPNL CSU |
Reference –2.342 –5.905 |
1.443 1.592 |
–5.170–0.486 –9.026–-2.784 |
0.105 <0.001 |
| Sex: female | 1.288 | 1.235 | –1.132–3.709 | 0.297 |
| Age | –0.095 | 0.033 | –0.158–-0.031 | 0.004 |
| Ethnicity Non-Caucasian Caucasian |
Reference –1.660 |
1.757 | –5.104–1.784 | 0.345 |
| Itch intensity WI-NRS-24h AI-NRS-24h WI-NRS-4w AI-NRS-4w |
-0.674 1.119 0.526 0.347 |
0.458 0.424 0.409 0.410 |
–1.572–0.225 0.287–1.950 –0.275–1.327 –0.456–1.151 |
0.142 0.008 0.198 0.397 |
| Disease duration >6 weeks to 6 months 6–12 months 1–10 years >10 years |
Reference –5.797 –4.723 –1.178 |
2.945 2.688 2.871 |
–11.568–-0.026 –9.991–0.545 –6.805–4.449 |
0.049 0.079 0.682 |
| Vigilance and awareness | 0.150 | 0.040 | 0.072–0.228 | <0.001 |
| QoL impairment None Mild Moderate Severe |
Reference 0.622 2.559 4.541 |
2.663 2.806 3.221 |
–4.597–5.840 –2.940–8.058 –1.771–10.853 |
0.815 0.362 0.159 |
| Sleep impairment None Mild Moderate Severe |
Reference 0.902 3.869 4.518 |
2.092 2.322 2.467 |
–3.198–5.002 –0.682–8.421 –0.316–9.352 |
0.666 0.096 0.067 |
|
Catastrophizing was assessed using the JKF scale. A positive beta represents a positive association, while a negative beta represents an inverse association. Significant factors are highlighted in bold. AI-NRS-24h/4w:average itch intensity on the numerical rating scale in the last 24 hours/4weeks; CPG:chronic prurigo; CPNL:chronic pruritus on non-lesional skin; CSU:chronic spontaneous urticaria; JKF:Itch-Cognition-Questionnaire; QoL:quality of life; WI-NRS-24h/4w:worst itch intensity on the numerical rating scale in the last 24 hours/4weeks. |
||||
DISCUSSION
Catastrophizing scores, as measured by the JKF, were significantly higher in CPG and CPNL compared to CSU patients and correlated with itch intensity, impairment of quality of life, depression, anxiety, stress as well as with vigilance and awareness to itch. The regression analysis confirmed the positive relationship between catastrophizing and average itch intensity and degree of vigilance and revealed a negative association with age.
The episodic course of CSU with fluctuating itch may explain lower levels of catastrophizing compared to CPG or CPNL, in which itch tends to be persistent and present every day. Moreover, the regression analysis indicated that catastrophizing was strongest in CPG, suggesting that the presence of visible skin lesions may contribute to additional negative cognitive appraisal. These findings align with previous observations in atopic dermatitis, which demonstrated associations of catastrophizing with itch intensity and impaired quality of life, highlighting its relevance in conditions with persistent symptoms and visible lesions (6).
Our regression analysis did not reveal an independent effect of impairment of quality of life or sleep disturbance on catastrophizing. However, we observed consistent positive correlations across all patient groups between these variables, as well as between catastrophizing and anxiety, depression and stress. Notably, several of the observed associations showed moderate to strong correlation coefficients (and not only statistical significance alone), suggesting a true association with clinical relevance. These findings are in line with previous observations in chronic pain studies, where catastrophizing has been shown to aggravate quality of life, sleep and emotional distress with increased levels of anxiety, depression and stress (5, 20, 21, 22). Similarly, in patients with atopic dermatitis, catastrophizing correlated positively with impairment of quality of life and psychological burden (6). Our data thus argue for an association between catastrophizing and overall psychosocial disease burden in CP, even though its independent contribution appears to be less pronounced when accounting for multiple covariates.
In our cohort, vigilance and awareness of itch showed a positive moderate association with catastrophizing, in accordance with a previous study on atopic dermatitis, in which vigilance to itch also showed a positive correlation with catastrophizing, although it did not remain significant in multivariate models (6). Our data suggest thus that a pronounced attention to itch may contribute to increased catastrophizing levels and as a result to worse clinical outcomes and higher psychological distress.
The findings of this study are in part consistent with the existing literature on chronic pain and catastrophizing in elderly individuals, demonstrating that older adults exhibit a reduced tendency to catastrophize compared to younger individuals, particularly in domains such as helplessness and rumination (23). The observed phenomenon may be explained by the concept of age-related resilience, which refers to a decrease in emotional reactivity with age (24). This suggests that younger patients may benefit more from cognitive-behavioural therapeutic support. A shorter disease duration of 6–12 months was negatively associated with catastrophizing. However, this observation was marginally significant and should therefore be interpreted with caution.
Overall, our findings agree with conceptual models of CP, which theorize that cognitive factors, such as catastrophizing, mediate the impact of physiological stressors on symptom perception and disease burden (25). As demonstrated previously in the field of chronic pain, catastrophizing has been shown to increase symptom perception and psychological distress (26). It can be hypothesized that a similar relationship exists between catastrophizing and itch, emphasizing the need for a multidimensional approach to managing patients with CP, as opposed to a purely biomedical perspective (6).
It is unclear what impact effective antipruritic therapies such as biologics and small molecules have on catastrophizing. In our data, we found no differences in catastrophizing between patients being treated with biologics or Janus kinase inhibitors compared to those with conventional therapies. However, our findings that patients with controlled disease catastrophize less than those with poorly controlled disease support the importance of early and effective therapy in preventing catastrophizing, as this can also lead to worsening of the symptoms and further comorbidities, particularly mental disorders.
Psychological approaches, including habit reversal training, relaxation techniques, cognitive restructuring, mindfulness-based stress reduction and acceptance and commitment therapy, have exhibited efficacy in reducing catastrophizing or habitual scratching in CP (27). Future studies should evaluate the effect of appropriate psychological interventions on catastrophizing in patients with CP. In addition, longitudinal and interventional studies are needed to clarify causality and determine whether modifying catastrophizing leads to sustained improvement in itch-related outcomes.
Clinically, our findings suggest that identifying and addressing high levels of catastrophizing may contribute to improved management of CP. However, such implications must be interpreted with caution given the cross-sectional design of the study.
Although we used the JKF total score in line with common practice, it is important to note that the JKF comprises subscales capturing different cognitive domains, such as helplessness, negative emotional appraisal, sleep-related cognitions and scratching-related cognitions. These subdomains may relate differently to itch intensity, quality of life impairment, psychological burden or disease control, and acknowledging them provides additional conceptual clarity.
Our study is strengthened by the use of validated tools, most notably the JKF with its long-standing psychometric validation. Nevertheless, our study has a few limitations. We included mostly patients of Caucasian ethnicity, which limits generalizability of findings to other ethnic groups and hinders the identification of possible differences in catastrophizing across ethnicities. Disease control could only be assessed for CPG and CSU using the PCT and UCT, respectively, while no equivalent validated measure is available for CPNL. Moreover, due to the design of the study, no causal relationship can be inferred from the observed associations. As this is an exploratory study, we did not correct for multiple testing. Therefore, type I errors cannot be ruled out. Given the large number of correlations and group comparisons performed, the risk of false-positive findings is increased, particularly for marginally significant p-values. Additionally, a relatively high number of predictors was included in the regression analysis. Accordingly, all results should be interpreted with caution, placing greater emphasis on the magnitude and consistency of the observed effect sizes (e.g. correlation coefficients) rather than on statistical significance alone.
Catastrophizing is a central and understudied cognitive process in CP. Integrating screening of high catastrophizers into routine clinical practice could support the identification of patients, who would benefit from targeted psychological approaches. Future studies should investigate interventions aimed at reducing catastrophizing to enhance clinical outcomes in CP.
REFERENCES
- Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother 2009; 9: 745–758. https://doi.org/10.1586/ern.09.34
- Strulov L, Zimmer EZ, Granot M, Tamir A, Jakobi P, Lowenstein L. Pain catastrophizing, response to experimental heat stimuli, and post-cesarean section pain. J Pain 2007; 8: 273–279. https://doi.org/10.1016/j.jpain.2006.09.004
- Burri A, Ogata S, Rice D, Williams F. Pain catastrophizing, neuroticism, fear of pain, and anxiety: Defining the genetic and environmental factors in a sample of female twins. PLoS One 2018; 13: e0194562. https://doi.org/10.1371/journal.pone.0194562
- Angst F, Lehmann S, Sandor PS, Benz T. Catastrophizing as a prognostic factor for pain and physical function in the multidisciplinary rehabilitation of fibromyalgia and low back pain. Eur J Pain 2022; 26: 1569–1580. https://doi.org/10.1002/ejp.1983
- Edwards RR, Bingham CO 3rd, Bathon J, Haythornthwaite JA. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum 2006; 55: 325–332. https://doi.org/10.1002/art.21865
- Lüßmann K, Montgomery K, Thompson A, Gieler U, Zick C, Kupfer J, et al. Mindfulness as predictor of itch catastrophizing in patients with atopic dermatitis: Results of a cross-sectional questionnaire study. Front Med 2021; 8: 627611. https://doi.org/10.3389/fmed.2021.627611
- Granot M, Yakov S, Kuperman P, Yosipovitch G, Ramon M. Catastrophizing thinking towards itch and pain in chronic itch patients. J Eur Acad Dermatol Venereol 2021; 35: e241–e242. https://doi.org/10.1111/jdv.16975
- Weisshaar E, Müller S, Szepietowski JC, Dalgard F, Garcovich S, Kupfer J, et al. European S2k guideline on chronic pruritus. Acta Derm Venereol 2025; 105: adv44220. https://doi.org/10.2340/actadv.v105.44220
- Ständer S, Weisshaar E, Mettang T, Szepietowski JC, Carstens E, Ikoma A, et al. Clinical classification of itch: A position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–294. https://doi.org/10.2340/00015555-0305
- Zeidler C, Pereira MP, Dugas M, Augustin M, Storck M, Weyer-Elberich V, et al. The burden in chronic prurigo: patients with chronic prurigo suffer more than patients with chronic pruritus on non-lesional skin: A comparative, retrospective, explorative statistical analysis of 4,484 patients in a real-world cohort. J Eur Acad Dermatol Venereol 2021; 35: 738–743. https://doi.org/10.1111/jdv.16929
- Brenaut E, Halvorsen JA, Dalgard FJ, Lien L, Balieva F, Sampogna F, et al. The self-assessed psychological comorbidities of prurigo in European patients: a multicentre study in 13 countries. J Eur Acad Dermatol Venereol 2019; 33: 157–162. https://doi.org/10.1111/jdv.15145
- Phan NQ, Blome C, Fritz F, Gerss J, Reich A, Ebata T, et al. Assessment of pruritus intensity: prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Derm Venereol 2012; 92: 502–507. https://doi.org/10.2340/00015555-1246
- Storck M, Sandmann S, Bruland P, Pereira MP, Steinke S, Riepe C, et al. Pruritus intensity scales across Europe: A prospective validation study. J Eur Acad Dermatol Venereol 2021; 35: 1176–1185. https://doi.org/10.1111/jdv.17111
- Krause K, Kessler B, Weller K, Veidt J, Chen SC, Martus P, et al. German version of ItchyQoL: validation and initial clinical findings. Acta Derm Venereol 2013; 93: 562–568. https://doi.org/10.2340/00015555-1544
- Metz M, Zeidler C, Hawro T, Pereira M, Maurer M, Bonnekoh H, et al. Development and validation of a patient-reported outcome measure to assess disease control in chronic prurigo. JAMA Dermatol 2024; 160: 187–193. https://doi.org/10.1001/jamadermatol.2023.5519
- Weller K, Groffik A, Church MK, Hawro T, Krause K, Metz M, et al. Development and validation of the Urticaria Control Test: a patient-reported outcome instrument for assessing urticaria control. J Allergy Clin Immunol 2014; 133: 1365–1372. https://doi.org/10.1016/j.jaci.2013.12.1076
- Heckman CJ, Schut C, Riley M, Ehlers A, Valdes-Rodriguez R, Kupfer J, et al. Development and psychometrics of the English version of the Itch Cognitions Questionnaire. PLoS One 2020; 15: e0230585. https://doi.org/10.1371/journal.pone.0230585
- Kunz M, Capito ES, Horn-Hofmann C, Baum C, Scheel J, Karmann AJ, et al. Psychometric properties of the German version of the Pain Vigilance and Awareness Questionnaire (PVAQ) in pain-free samples and samples with acute and chronic pain. Int J Behav Med 2017; 24: 260–271. https://doi.org/10.1007/s12529-016-9585-4
- Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol 2005; 44: 227–239. https://doi.org/10.1348/014466505X29657
- Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: Development and validation. Psychol Assess 1995; 7: 524–532. https://doi.org/10.1037/1040-3590.7.4.524
- Abeler K, Friborg O, Engstrøm M, Sand T, Bergvik S. Sleep characteristics in adults with and without chronic musculoskeletal pain: The role of mental distress and pain catastrophizing. Clin J Pain 2020; 36: 707–715. https://doi.org/10.1097/AJP.0000000000000854
- McPeak AE, Allaire C, Williams C, Albert A, Lisonkova S, Yong PJ. Pain catastrophizing and pain health-related quality-of-life in endometriosis. Clin J Pain 2018; 34: 349–356. https://doi.org/10.1097/AJP.0000000000000539
- Petrini L, Arendt-Nielsen L. Pain catastrophizing in the elderly: An experimental pain study. Scand J Pain 2024; 24: 24. https://doi.org/10.1515/sjpain-2023-0035
- Rolandi E, Rossi M, Colombo M, Pettinato L, Del Signore F, Aglieri V, et al. Lifestyle, cognitive, and psychological factors associated with a resilience phenotype in aging: A multidimensional approach on a population-based sample of oldest-old (80+). J Gerontol B Psychol Sci Soc Sci 2024; 79: gbae132. https://doi.org/10.1093/geronb/gbae132
- Silverberg JI, Kantor RW, Dalal P, Hickey C, Shaunfield S, Kaiser K, et al. A comprehensive conceptual model of the experience of chronic itch in adults. Am J Clin Dermatol 2018; 19: 759–769. https://doi.org/10.1007/s40257-018-0381-6
- Turner JA, Jensen MP, Warms CA, Cardenas DD. Catastrophizing is associated with pain intensity, psychological distress, and pain-related disability among individuals with chronic pain after spinal cord injury. Pain 2002; 98: 127–134. https://doi.org/10.1016/s0304-3959(02)00045-3
- Schut C, Mollanazar NK, Kupfer J, Gieler U, Yosipovitch G. Psychological interventions in the treatment of chronic itch. Acta Derm Venereol 2016; 96: 157–161. https://doi.org/10.2340/00015555-2177