SHORT COMMUNICATION
Verruciform Xanthoma of the Prepuce Causing Secondary Phimosis and Urinary Dysfunction
Yuto YAMAMURA1![]() , Kazuyasu FUJII1*, Kazutoshi NISHIMURA1, Shunya USUI1 and Atsushi OTSUKA1
, Kazuyasu FUJII1*, Kazutoshi NISHIMURA1, Shunya USUI1 and Atsushi OTSUKA1
1Department of Dermatology, Kindai University Hospital, Osaka, Japan. *Email: kazuyasu.fujii@med.kindai.ac.jp
Citation: Acta Derm Venereol 2026; 106: adv-2026-0406. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0406.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 5, 2026. Accepted after revision: Mar 2, 2026.
Published: Mar 26, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Verruciform xanthoma is a benign tumour characterized histopathologically by papillary epidermal hyperplasia and an accumulation of foamy macrophages within the dermal papillae. It most commonly arises on the oral mucosa but may also occur at mucocutaneous junctions, including the genital skin. In dermatological practice, verruciform xanthoma predominantly affects the scrotum of elderly men, and involvement of the penis is relatively uncommon (1). The lesion is usually superficial, well circumscribed and slowly progressive, and is generally regarded as an asymptomatic condition (1).
In contrast, the external genitalia comprise a complex and highly mobile anatomical structure, in which the prepuce, glans and urethral meatus are closely integrated. Lesions arising in this region may therefore, depending on their location and long-term course, result in morphological alterations and functional impairment, including voiding disturbances (2).
However, reports describing such functional or anatomical consequences remain scarce and particularly limited in cases of verruciform xanthoma, including those arising on the penis. Here, we report an extremely uncommon case of verruciform xanthoma arising on the prepuce that, over a prolonged course, was associated with chronic mechanical traction and inflammation, leading to glans inversion, cicatricial narrowing of the prepuce, secondary phimosis and urinary dysfunction.
CASE REPORT
A man in his 90s with no history of phimosis, voiding dysfunction or urinary tract infection noticed a small nodule on the prepuce at the 6 o’clock position several years earlier. The lesion gradually enlarged, and as its weight increased, the prepuce was progressively pulled anteriorly, making retraction increasingly difficult. He subsequently developed an unstable urinary stream and marked difficulty during voiding, prompting referral for treatment. There was no associated urethritis or dysuria.
On physical examination, a red, papillomatous, pedunculated mass was observed on the distal prepuce. The adjacent prepuce showed no opening, and the glans could not be exposed (Fig. 1A). A pinhole-shaped opening was identified at the 12 o’clock position of the prepuce (Fig. 1B).
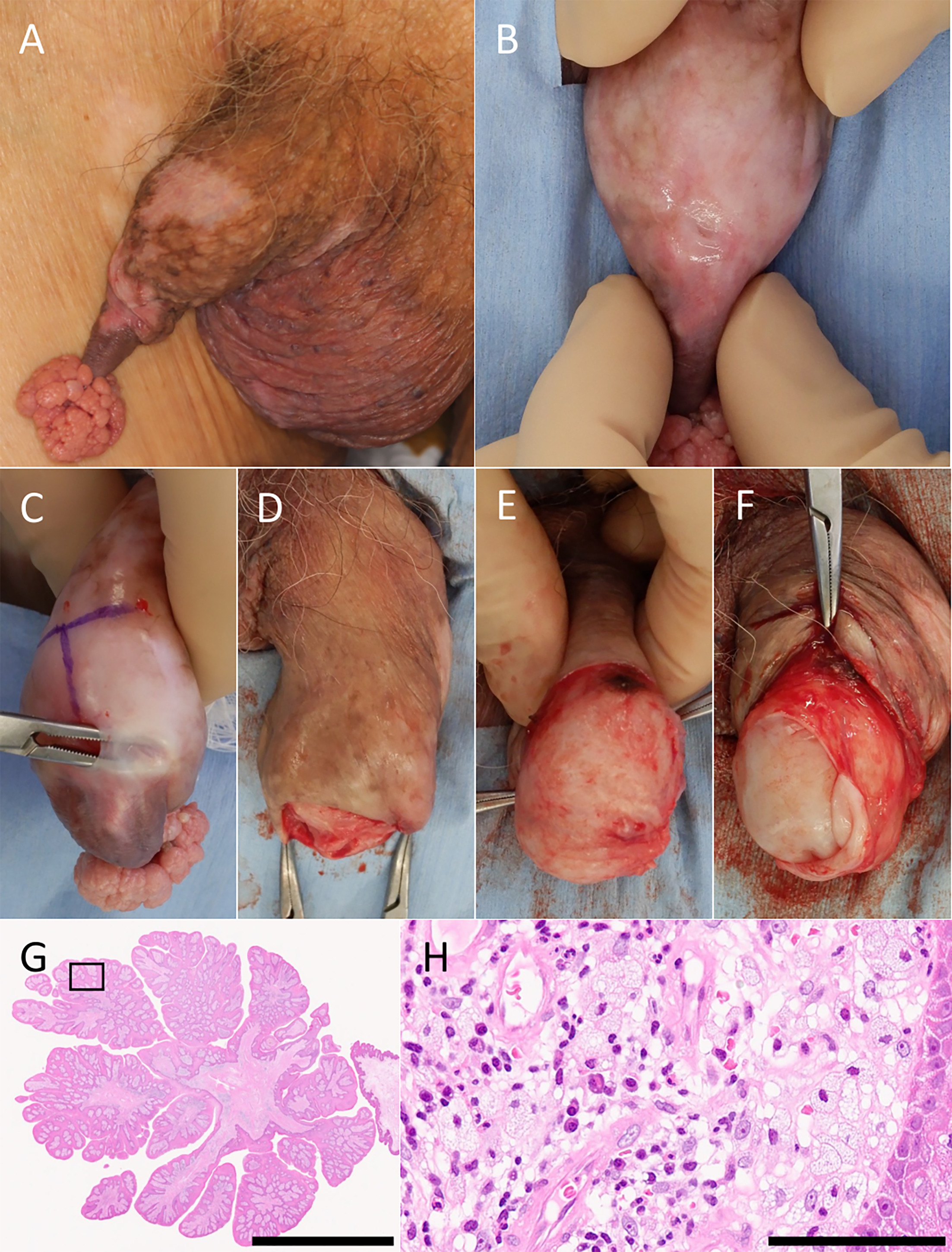
Fig. 1. Clinical, intraoperative and histopathological findings. A: A red, papillomatous mass at the distal prepuce. B: A pinhole-shaped opening at the 12 o’clock position of the prepuce, through which the patient voided. C: An attempt at blunt dissection by inserting dissecting forceps through the preputial fistula; dense adhesions were encountered proximally, making dissection difficult. D: Circumferential incision of the prepuce and excision of the tumour. E: The glans completely covered by a thin membranous structure, with a focal depression near the base of the tumour. F: Partial incision of the membranous structure allowed exposure of the inverted glans, which was manually reduced. G: Low-power view showing a pedunculated papillomatous lesion with papillary epidermal hyperplasia (hematoxylin and eosin stain; scale bar, 5 mm). H: High-power view demonstrating numerous foamy macrophages within the dermal papillae accompanied by inflammatory cell infiltration (hematoxylin and eosin stain; scale bar, 100 μm).
Based on these findings, verruciform xanthoma arising from the prepuce was clinically suspected, and surgical excision was planned. During surgery, the prepuce was incised through the pinhole opening (Fig. 1C). Circumferential incision was then performed, and the tumour was excised together with the prepuce (Fig. 1D).
After tumour removal, the glans was found to be completely covered by a thin membranous structure (Fig. 1E; Fig. S1). Partial incision and eversion of this structure allowed exposure of the glans (Fig. 1F). At that time, the glans was inverted with the pivot point at the 6 o’clock position of the urethral meatus, and manual reduction revealed a focal depression at the same site. The wound edges were approximated, and the operation was completed. Histopathological examination confirmed the diagnosis of verruciform xanthoma (Fig. 1G and H).
The postoperative course was uneventful. Voiding dysfunction resolved completely, and no wound complications or infections were observed.
DISCUSSION
Verruciform xanthoma is typically a superficial, well-circumscribed benign tumour that enlarges slowly and rarely causes marked morphological changes or functional impairment of surrounding anatomical structures (1). In contrast, in the present case, verruciform xanthoma arose on the highly mobile prepuce of the penis, a site prone to deformation, and over a prolonged course, tumour enlargement combined with persistent mechanical traction resulted in both morphological alteration and functional disturbance.
The distinctive morphological changes observed in this case may be explained by pedunculated tumour growth on the prepuce, which likely acted as a source of persistent mechanical traction over a prolonged period. In addition, glans inversion with a pivot point at the 6 o’clock position of the urethral meatus was observed, suggesting that traction applied to anatomically less mobile structures, such as the frenulum, may have contributed; however, this interpretation remains speculative.
In contrast, the mechanism underlying the pinhole-shaped preputial opening is most plausibly attributed to distal preputial narrowing caused by chronic inflammation of the inner prepuce, leading to fibrosis and reduced elasticity (Fig. S2). Such cicatricial narrowing is a well-recognized mechanism in the development of true phimosis (3). Lichen sclerosus is a representative organic disease associated with this process (4), whereas comparable mechanisms related to benign tumours, including verruciform xanthoma, have rarely been reported.
This case demonstrates that even benign tumours arising on the prepuce may, depending on their location and prolonged course, lead to anatomical remodelling and functional impairment through persistent mechanical effects and chronic inflammation. In addition, the ability to visually document morphological changes involving inversion of the glans and inner prepuce during the progression to true phimosis may help to complement current understanding of the pathophysiology of acquired phimosis from a dermatological perspective.
ACKNOWLEDGEMENTS
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
REFERENCES
- Stiff KM, Cohen PR. Vegas (verruciform genital-associated) xanthoma: a comprehensive literature review. Dermatol Ther 2017; 7: 65–79. https://doi.org/10.1007/s13555-016-0155-0
- Hsu FC, Yu DS, Pu TW, Wu MJ, Meng E. Unusual presentation of penile giant condyloma acuminatum with spontaneous prepuce perforation: a case report. World J Clin Cases 2023; 11: 7107–7112. https://doi.org/10.12998/wjcc.v11.i29.7107
- McGregor TB, Pike JG, Leonard MP. Pathologic and physiologic phimosis: approach to the phimotic foreskin. Can Fam Physician 2007; 53: 445–448.
- Powell JJ, Wojnarowska F. Lichen sclerosus. Lancet 1999; 353: 1777–1783. https://doi.org/10.1016/s0140-6736(98)08228-2